
Abstract
Background
Pancreatic cancer can be difficult to diagnose. Fine-needle aspiration (FNA) biopsies may be negative even when malignancy is present.
Aims
To identify endosonographic features predictive of malignancy that will separate patients into high- and low-risk groups, in whom a negative FNA effectively rules out malignancy.
Methods
Patients presenting for endoscopic ultrasound (EUS) evaluation for suspected pancreatic mass were prospectively enrolled. If a mass or abnormal lymph nodes were present, sampling via fine-needle aspiration (FNA) was performed. The characteristics of patients with cancer were compared to the characteristics of patients without cancer using Chi-square testing and t-tests.
Results
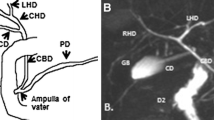
Seventy-three patients were enrolled. Thirty-three patients had cancer and 40 had benign disease. On multivariate analysis, only vascular or organ invasion and dilation of the pancreatic duct (PD) were significantly associated with cancer. PD dilation was examined as a stand-alone feature. The presence of a dilated PD placed patients into a group with a 65% prevalence of malignancy. In the non-dilated PD group, the prevalence of malignancy was only 17%, and in this group, the negative predictive value of FNA was 100%, compared to an NPV of 73% in the entire cohort.
Conclusions
The most significant negative predictive endosonographic finding in patients with suspected pancreatic cancer is a non-dilated PD. If a patient with suspected pancreatic cancer does not have a dilated PD and the FNA is negative for malignancy, the likelihood of cancer is low.


Similar content being viewed by others


References
Smith CD, Behrns KE, van Heerden JA, Sarr MG. Radial pancreaticoduodenectomy for misdiagnosed pancreatic mass. Br J Surg. 1994;81:585–589.
Thompson JS, Murayama KM, Edney JA, Rikkers LF. Pancreaticoduodenectomy for suspected but unproven malignancy. Am J Surg. 1994;168:571–575.
van Gulik TM, Moojen TM, van Geenen R, Rauws EA, Obertop H, Gouma DJ. Differential diagnosis of focal pancreatitis and pancreatic cancer. Ann Oncol. 1999;10(Suppl 4):85–88.
Van Gulik M, Reeders JW, Bosma A, et al. Incidence and clinical findings of benign, inflammatory disease in patients resected for presumed pancreatic head cancer. Gastrointest Endosc. 1997;46:417–423.
Nakaizumi A, Uehara H, Iishi H, et al. Endoscopic ultrasonography in diagnosis and staging of pancreatic cancer. Dig Dis Sci. 1995;40:696–700.
Mertz HR, Sechopoulos P, Delbeke D, et al. EUS, PET, and CT scanning for evaluation of pancreatic adenocarcinoma. Gastrointest Endosc. 2000;52:367–371.
Snady H, Cooperman A, Siegel J. Endoscopic ultrasonography compared with computed tomography with ERCP in patients with obstructive jaundice or small peri-pancreatic mass. Gastrointest Endosc. 1992;38:27–34.
Raut CP, Graut AM, Staerkel GA, et al. Diagnostic accuracy of endoscopic ultrasound-guided fine-needle aspiration in patients with presumed pancreatic cancer. J Gastrointest Surg. 2003;7:118–126.
Harewood G, Wiersema M. Endosonography-guided fine needle aspiration in the evaluation of pancreatic masses. Am J Gastroenterol. 2002;97:1386–1391.
Gress F, Gottlieb K, Sherman S, et al. Endoscopic ultrasonography-guided fine-needle aspiration biopsy of suspected pancreatic cancer. Ann Intern Med. 2001;134:459–464.
Hunt G, Faigel D. Assessment of EUS for diagnosing, staging, and determining resectability of pancreatic cancer: a review. Gastrointest Endosc. 2002;55:232–237.
Lerma E, Musulen E, Cuatrecasas M, et al. Fine needle aspiration cytology in pancreatic pathology. Acta Cytol. 1996;40:683–686.
Chang KJ, Nguyen P, Erickson RA, et al. The clinical utility of endoscopic ultrasound-guided fine-needle aspiration in the diagnosis and staging of pancreatic adenocarcinoma. Gastrointest Endosc. 1997;45:387–393.
Bret PM, Nicolet V, Labadie M. Percutaneous fine-needle aspiration biopsy of the pancreas. Diagn Cytopathol. 1986;2:221–227.
Eloubeidi MA, Jhala D, Chhieng D, et al. Yield of endoscopic ultrasound guided fine needle aspiration biopsy in patients with suspected pancreatic carcinoma. Cancer. 2003;99:285–292.
Takahashi A, Yamao K, Okubo K, et al. Differential diagnosis of pancreatic cancer and focal pancreatitis by using EUS-guided FNA. Gastrointest Endosc. 2005;61:76–79.
Varadarajulu S, Tamhane A, Eloubeidi M. Yield of EUS-guided FNA of pancreatic masses in the presence or absence of chronic pancreatitis. Gastrointest Endosc. 2005;62:728–736.
Agarwal B, Abu-Hamda E, Molke KL, et al. Endoscopic ultrasound guided fine needle aspiration and multidetector spiral CT in the diagnosis of pancreatic cancer. Am J Gastroenterol. 2004;99:844–850.
Moskaluk CA, Kern SE. Molecular genetics of pancreatic cancer. In: Reber HA, ed. Pancreatic Cancer. Totowa: Humana Press; 1998:3–20.
Howe HL, Wu X, Ries L. Annual report to the nation on the status of cancer, 1975–2003, featuring cancer among U.S. Hispanic/Latino populations. Cancer. 2006;107:1711–1742.
Ghaneh P, Neoptolemos J. Pancreatic exocrine tumors. In: Weinstein WM, Hawkey CJ, Bosch J, eds. Clinical Gastroenterology and Hepatology 2005. London: Elsevier; 2005:521–533.
Inoue K, Ohuchida J, Ohtsuka T, et al. Severe localized stenosis and marked dilation of the main pancreatic duct are indicators of pancreatic cancer instead of chronic pancreatitis on endoscopic retrograde balloon pancreatography. Gastrointest Endosc. 2003;58:510–515.
Edge MD, Hoteit M, Patel A, et al. Clinical significance of main pancreatic duct dilation on computed tomography: single and double duct dilation. World J Gastroenterol. 2007;13:1701–1705.
Jani ND, Brody D, Kaushik N. Yield of endoscopic ultrasound in patients referred for isolated pancreatic duct dilation. Gastrointest Endosc. 2007;65:AB307.
Tessler DA, Catanzaro A, Velanovich V, et al. Predictors of cancer in patients with suspected pancreatic malignancy without a tissue diagnosis. Am J Surg. 2006;191:191–197.
Cooperman A, Fader A, Cushin B, et al. Surgery and cancer of the pancreas: will common sense become common practice? Hematol Oncol Clin N Am. 2002;16:81–94.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rodriguez, S., Faigel, D. Absence of a Dilated Duct Predicts Benign Disease in Suspected Pancreas Cancer: A Simple Clinical Rule. Dig Dis Sci 55, 1161–1166 (2010). https://doi.org/10.1007/s10620-009-0889-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-009-0889-y