
Abstract
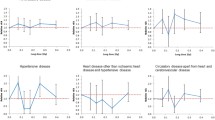
High-dose ionizing radiation is associated with circulatory disease. Risks from lower-dose fractionated exposures, such as from diagnostic radiation procedures, remain unclear. In this study we aimed to ascertain the relationship between fractionated low-to-medium dose radiation exposure and circulatory disease mortality in a cohort of 13,568 tuberculosis patients in Massachusetts, some with fluoroscopy screenings, between 1916 and 1961 and follow-up until the end of 2002. Analysis of mortality was in relation to cumulative thyroid (cerebrovascular) or lung (all other circulatory disease) radiation dose via Poisson regression. Over the full dose range, there was no overall radiation-related excess risk of death from circulatory disease (n = 3221; excess relative risk/Gy −0.023; 95 % CI −0.067, 0.028; p = 0.3574). Risk was somewhat elevated in hypertensive heart disease (n = 89; excess relative risk/Gy 0.357; 95 % CI −0.043, 1.030, p = 0.0907) and slightly decreased in ischemic heart disease (n = 1950; excess relative risk/Gy −0.077; 95 % CI −0.130, −0.012; p = 0.0211). However, under 0.5 Gy, there was a borderline significant increasing trend for all circulatory disease (excess relative risk/Gy 0.345; 95 % CI −0.032, 0.764; p = 0.0743) and for ischemic heart disease (excess relative risk/Gy 0.465; 95 % CI, −0.032, 1.034, p = 0.0682). Pneumolobectomy increased radiation–associated risk (excess relative risk/Gy 0.252; 95 % CI 0.024, 0.579). Fractionation of dose did not modify excess risk. In summary, we found no evidence of radiation-associated excess circulatory death risk overall, but there are indications of excess circulatory death risk at lower doses (<0.5 Gy). Although consistent with other radiation-exposed groups, the indications of higher risk at lower doses are unusual and should be confirmed against other data.

Similar content being viewed by others

References
United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). UNSCEAR 2006 Report. Annex A. Epidemiological Studies of Radiation and Cancer. New York: United Nations; 2008. p. 13–322.
Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation NRC. Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII—Phase 2. Washington, DC: National Academy Press; 2006. p. 1-406.
Little MP, Kleinerman RA, Stovall M, Smith SA, Mabuchi K. Analysis of dose response for circulatory disease after radiotherapy for benign disease. Int J Radiat Oncol Biol Phys. 2012;84(5):1101–9. doi:10.1016/j.ijrobp.2012.01.053.
Darby SC, Ewertz M, McGale P, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368(11):987–98. doi:10.1056/NEJMoa1209825.
Mulrooney DA, Yeazel MW, Kawashima T, et al. Cardiac outcomes in a cohort of adult survivors of childhood and adolescent cancer: retrospective analysis of the Childhood Cancer Survivor Study cohort. BMJ. 2009;339:b4606.
Tukenova M, Guibout C, Oberlin O, et al. Role of cancer treatment in long-term overall and cardiovascular mortality after childhood cancer. J Clin Oncol. 2010;28(8):1308–15. doi:10.1200/JCO.2008.20.2267.
Shimizu Y, Kodama K, Nishi N, et al. Radiation exposure and circulatory disease risk: Hiroshima and Nagasaki atomic bomb survivor data, 1950–2003. BMJ. 2010;340:b5349.
Little MP, Azizova TV, Bazyka D, et al. Systematic review and meta-analysis of circulatory disease from exposure to low-level ionizing radiation and estimates of potential population mortality risks. Environ Health Perspect. 2012;120(11):1503–11. doi:10.1289/ehp.1204982.
McMillan TJ, Bennett MR, Bridges BA, et al. Circulatory disease risk. Report of the independent Advisory Group on Ionising Radiation. Health Protection Agency, Holborn Gate, 330 High Holborn, London; 2010. p. 1–116.
Boice JD Jr, Preston D, Davis FG, Monson RR. Frequent chest X-ray fluoroscopy and breast cancer incidence among tuberculosis patients in Massachusetts. Radiat Res. 1991;125(2):214–22.
Howe GR. Lung cancer mortality between 1950 and 1987 after exposure to fractionated moderate-dose-rate ionizing radiation in the Canadian fluoroscopy cohort study and a comparison with lung cancer mortality in the atomic bomb survivors study. Radiat Res. 1995;142(3):295–304.
Howe GR, McLaughlin J. Breast cancer mortality between 1950 and 1987 after exposure to fractionated moderate-dose-rate ionizing radiation in the Canadian fluoroscopy cohort study and a comparison with breast cancer mortality in the atomic bomb survivors study. Radiat Res. 1996;145(6):694–707.
Little MP, Boice JD Jr. Comparison of breast cancer incidence in the Massachusetts tuberculosis fluoroscopy cohort and in the Japanese atomic bomb survivors. Radiat Res. 1999;151(2):218–24.
Davis FG, Boice JD Jr, Hrubec Z, Monson RR. Cancer mortality in a radiation-exposed cohort of Massachusetts tuberculosis patients. Cancer Res. 1989;49(21):6130–6.
Zablotska LB, Little MP, Cornett RJ. Potential increased risk of ischemic heart disease mortality with significant dose fractionation in the Canadian fluoroscopy cohort study. Am J Epidemiol. 2014;179(1):120–31. doi:10.1093/aje/kwt244.
Boice JD Jr. Follow-up methods to trace women treated for pulmonary tuberculosis, 1930–1954. Am J Epidemiol. 1978;107(2):127–39.
Boice JD Jr, Rosenstein M, Trout ED. Estimation of breast doses and breast cancer risk associated with repeated fluoroscopic chest examinations of women with tuberculosis. Radiat Res. 1978;73(2):373–90.
Boice JD, Monson RR, Rosenstein M. Cancer mortality in women after repeated fluoroscopic examinations of the chest. J Natl Cancer Inst 1981;66(5):863–7.
Ridker PM. Inflammation, infection, and cardiovascular risk: how good is the clinical evidence? Circulation. 1998;97(17):1671–4.
Gura T. Infections: a cause of artery-clogging plaques? Science 1998;281(5373):35–7.
McCullagh P, Nelder JA. Generalized linear models. 2nd edition. Monographs on statistics and applied probability 37. Boca Raton, FL: Chapman and Hall/CRC; 1989. p. 1–526.
Preston DL, Lubin JH, Pierce DA, McConney ME. Epicure release 2.10. Seattle: Hirosoft International; 1998.
Austin PC, Tu JV. Automated variable selection methods for logistic regression produced unstable models for predicting acute myocardial infarction mortality. J Clin Epidemiol. 2004;57(11):1138–46. doi:10.1016/j.jclinepi.2004.04.003.
Akaike H. Information theory and an extension of the maximum likelihood principle. In: Petrov BN, Czáki F, editors. 2nd International symposium on information theory. Budapest: Akadémiai Kiadó; 1973. p. 267–81.
Akaike H. Likelihood of a model and information criteria. J Econ. 1981;16(1):3–14.
R Project. R version 3.1.1 http://www.r-project.org/. 2014.
Hastie T, Tibshirani R. Generalized additive models for medical research. Stat Methods Med Res. 1995;4(3):187–96.
Little MP, Tawn EJ, Tzoulaki I, et al. A systematic review of epidemiological associations between low and moderate doses of ionizing radiation and late cardiovascular effects, and their possible mechanisms. Radiat Res. 2008;169(1):99–109. doi:10.1667/RR1070.1.
Schultz-Hector S, Trott KR. Radiation-induced cardiovascular diseases: is the epidemiologic evidence compatible with the radiobiologic data? Int J Radiat Oncol Biol Phys. 2007;67(1):10–8. doi:10.1016/j.ijrobp.2006.08.071.
Mitchel REJ, Hasu M, Bugden M, et al. Low-dose radiation exposure and atherosclerosis in ApoE −/− mice. Radiat Res. 2011;175(5):665–76. doi:10.1667/RR2176.1.
Adams MJ, Grant EJ, Kodama K, et al. Radiation dose associated with renal failure mortality: a potential pathway to partially explain increased cardiovascular disease mortality observed after whole-body irradiation. Radiat Res. 2012;177(2):220–8. doi:10.1667/RR2746.1.
Lenarczyk M, Lam V, Jensen E, et al. Cardiac injury after 10 Gy total body irradiation: indirect role of effects on abdominal organs. Radiat Res. 2013;180(3):247–58. doi:10.1667/RR3292.1.
Rosenstein M. Personal communication to Mark Little. 2014.
Kusunoki Y, Kyoizumi S, Hirai Y, et al. Flow cytometry measurements of subsets of T, B and NK cells in peripheral blood lymphocytes of atomic bomb survivors. Radiat Res. 1998;150(2):227–36.
Danesh J, Whincup P, Lewington S, et al. Chlamydia pneumoniae IgA titres and coronary heart disease. Prospective study and meta-analysis. Eur Heart J. 2002;23(5):371–5. doi:10.1053/euhj.2001.2801.
Whincup P, Danesh J, Walker M, et al. Prospective study of potentially virulent strains of Helicobacter pylori and coronary heart disease in middle-aged men. Circulation. 2000;101(14):1647–52.
Grayston JT, Kronmal RA, Jackson LA, et al. Azithromycin for the secondary prevention of coronary events. N Engl J Med. 2005;352(16):1637–45. doi:10.1056/NEJMoa043526.
Cannon CP, Braunwald E, McCabe CH, et al. Antibiotic treatment of Chlamydia pneumoniae after acute coronary syndrome. N Engl J Med. 2005;352(16):1646–54. doi:10.1056/NEJMoa043528.
Lowe D, Raj K. Premature aging induced by radiation exhibits pro-atherosclerotic effects mediated by epigenetic activation of CD44 expression. Aging Cell. 2014;13(5):900–10. doi:10.1111/acel.12253.
Little MP, Gola A, Tzoulaki I. A model of cardiovascular disease giving a plausible mechanism for the effect of fractionated low-dose ionizing radiation exposure. PLoS Comput Biol. 2009;5(10):e1000539. doi:10.1371/journal.pcbi.1000539.
Fuster V, Moreno PR, Fayad ZA, Corti R, Badimon JJ. Atherothrombosis and high-risk plaque: part I: evolving concepts. J Am Coll Cardiol. 2005;46(6):937–54. doi:10.1016/j.jacc.2005.03.074.
Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque. J Am Coll Cardiol. 2006;47(8 Suppl):C13–8. doi:10.1016/j.jacc.2005.10.065.
Little MP, Tawn EJ, Tzoulaki I, et al. Review and meta-analysis of epidemiological associations between low/moderate doses of ionizing radiation and circulatory disease risks, and their possible mechanisms. Radiat Environ Biophys. 2010;49(2):139–53. doi:10.1007/s00411-009-0250-z.
Little MP, Zablotska LB, Lipshultz SE. Ischemic heart disease after breast cancer radiotherapy. N Eng J Med. 2013;368(26):2523–4. doi:10.1056/NEJMc1304601#SA1.
Burns DM. Epidemiology of smoking-induced cardiovascular disease. Prog Cardiovasc Dis. 2003;46(1):11–29. doi:10.1016/S0033-0620(03)00079-3.
Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998;97(18):1837–47.
Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–52. doi:10.1016/S0140-6736(04)17018-9.
Yamada M, Wong FL, Fujiwara S, Akahoshi M, Suzuki G. Noncancer disease incidence in atomic bomb survivors, 1958–1998. Radiat Res. 2004;161(6):622–32. doi:10.1667/RR3183
Azizova TV, Muirhead CR, Druzhinina MB, et al. Cardiovascular diseases in the cohort of workers first employed at Mayak PA in 1948–1958. Radiat Res. 2010;174(2):155–68. doi:10.1667/RR1789.1.
Azizova TV, Haylock RGE, Moseeva MB, Bannikova MV, Grigoryeva ES. Cerebrovascular diseases incidence and mortality in an extended Mayak Worker Cohort 1948–1982. Radiat Res. 2014;182(5):529–44. doi:10.1667/RR13680.1.
International Commission on Radiological Protection. ICRP statement on tissue reactions and early and late effects of radiation in normal tissues and organs - threshold doses for tissue reactions in a radiation protection context. ICRP publication 118. Ann. ICRP. 2012;41(1–2):1–322. doi:10.1016/j.icrp.2007.10.003.
Schöllnberger H, Kaiser JC, Jacob P, Walsh L. Dose-responses from multi-model inference for the non-cancer disease mortality of atomic bomb survivors. Radiat Environ Biophys. 2012;51(2):165–78. doi:10.1007/s00411-012-0410-4.
Little MP, Azizova TV, Bazyka D, et al. Comment on “Dose-responses from multi-model inference for the non-cancer disease mortality of atomic bomb survivors” (Radiat. Environ. Biophys (2012) 51:165–178) by Schöllnberger et al. Radiat Environ Biophys 2013;52(1):157–9. doi:10.1007/s00411-012-0453-6.
McGeoghegan D, Binks K, Gillies M, Jones S, Whaley S. The non-cancer mortality experience of male workers at British Nuclear Fuels plc, 1946-2005. Int J Epidemiol. 2008;37(3):506–18. doi:10.1093/ije/dyn018.
Muirhead CR, O’Hagan JA, Haylock RGE, et al. Mortality and cancer incidence following occupational radiation exposure: third analysis of the National Registry for Radiation Workers. Br J Cancer. 2009;100(1):206–12. doi:10.1038/sj.bjc.6604825.
Vrijheid M, Cardis E, Ashmore P, et al. Mortality from diseases other than cancer following low doses of ionizing radiation: results from the 15-Country Study of nuclear industry workers. Int J Epidemiol. 2007;36(5):1126–35. doi:10.1093/ije/dym138.
Krestinina LY, Epifanova S, Silkin S, et al. Chronic low-dose exposure in the Techa River Cohort: risk of mortality from circulatory diseases. Radiat Environ Biophys. 2013;52(1):47–57. doi:10.1007/s00411-012-0438-5.
Grosche B, Lackland DT, Land CE, et al. Mortality from cardiovascular diseases in the Semipalatinsk historical cohort, 1960–1999, and its relationship to radiation exposure. Radiat Res. 2011;176(5):660–9. doi:10.1667/RR2211.1.
Acknowledgments
MPL and AVB were supported by the Intramural Research Program of the National Institutes of Health, the National Cancer Institute (NCI), Division of Cancer Epidemiology and Genetics, and LBZ by NCI grants 5K07CA132918 and 1R03CA188614. The authors are grateful for the detailed and helpful comments of Dr Marvin Rosenstein and a referee.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no financial conflicts of interest.
Appendices
Appendix 1: Background models selected
See Tables 8, 9, 10, 11, 12, 13 and 14.
Appendix 2: Effect of alternative background models selected via minimizing Akaike information criterion
In this appendix we consider an alternative set of explanatory background models for each endpoint, selected via an automatic variable selection process, by minimizing the Akaike information criterion (AIC) [24, 25]. Minimizing AIC is a standard method of variable selection that avoids over-parameterised (and therefore over-fitted) models. AIC penalizes against overfitting by adding 2 × [number of fitted parameters] to the model deviance. We used an iterative mixed-forward–backward stepwise procedure to minimize AIC using models with Poisson error via R [26].
The models used the set of candidate variables listed in Table 15, in which the optimal models chosen are also indicated. We provide the analog of Table 2 using these alternative background models in Table 16.
Appendix 3: Generalized additive models (GAM)
See Table 17.
Rights and permissions
About this article

Cite this article
Little, M.P., Zablotska, L.B., Brenner, A.V. et al. Circulatory disease mortality in the Massachusetts tuberculosis fluoroscopy cohort study. Eur J Epidemiol 31, 287–309 (2016). https://doi.org/10.1007/s10654-015-0075-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-015-0075-9