
Abstract
Introduction
Previous studies have demonstrated the superior efficacy of a novel aerosol foam formulation of fixed combination calcipotriene 0.005% (Cal) and betamethasone dipropionate 0.064% (BD), compared with the ointment formulation. The aim of this study is to ascertain whether enhanced bioavailability of the active ingredients due to supersaturation and/or occlusive properties can explain the observed greater clinical efficacy.
Methods
Solubility and evaporation experiments were conducted to examine the abilities of Cal/BD aerosol foam ingredients to create a supersaturated environment. Optical microscopy, Raman imaging and X-ray powder diffraction were used to examine the physical state of Cal and BD in the formulations after application, and determine whether a supersaturated state remained stable for clinically relevant time periods. In vitro skin penetration and ex vivo biomarker assays were conducted to compare the skin penetration and bioavailability of Cal and BD from the aerosol foam and ointment formulations, respectively. Occlusive properties were examined via transepidermal water loss.
Results
Solubility studies showed that Cal and BD solubility increased with increasing dimethyl ether (DME) content. Both active ingredients are completely dissolved in the final aerosol foam formulation. DME rapidly evaporates after spraying, and the amount was reduced to 0.5% of the initial amount after 2 min. This led to the formation of a supersaturated environment, where Cal and BD crystals were absent for at least 26 h after application. Cal/BD aerosol foam had significantly greater in vitro skin penetration and had increased bioavailability compared with Cal/BD ointment. Both formulations effectively occluded the skin.
Conclusion
A stable supersaturated solution of Cal/BD in the aerosol foam leads to increased bioavailability and explains the improved clinical effect when compared to the Cal/BD ointment.
Funding
The studies included in the paper are all conducted by LEO Pharma A/S or CROs on behalf of LEO Pharma A/S.
Similar content being viewed by others


Introduction
Psoriasis is a chronic, immune-mediated inflammatory disorder characterized by scaly plaques of thickened skin [1, 2]. Many patients with psoriasis are treated topically with vitamin D3 analogues and corticosteroids, either as separate products used together or as a fixed combination treatment [3]. The fixed combination calcipotriene 0.005% (Cal) and betamethasone dipropionate 0.064% (BD) in ointment and gel formulations are established as routine treatments for psoriasis [4]. Adherence to topical therapies is often poor due to the inconvenient and cumbersome nature of available therapies [5], but also due to low efficacy of these therapies [6]. Hence, adherence to the topical treatment could potentially be enhanced by designing a topical product with improved cosmetic properties, easier application and improved efficacy. Considerable research has been undertaken to improve drug delivery as the effect of medication depends on the bioavailability of the active ingredients [7].
In response to patients’ needs, a novel alcohol-free and surfactant-free aerosol foam formulation of Cal/BD has been developed [8–13]. The Cal/BD aerosol foam is a pressurized formulation of a vehicle base with Cal and BD dissolved in an innovative mixture of volatile propellants, butane and dimethyl ether (DME). When the formulation is sprayed from the can, the propellants evaporate rapidly and a thin layer of foam is formed on the skin. Compared with the Cal/BD ointment, improved skin blanching and clinical efficacy of the Cal/BD aerosol foam have been confirmed in previously reported studies [13, 14].
To be effective, topical treatments require penetration of the active ingredient into the skin; poor penetration can lead to low or lack of clinical efficacy [7, 15, 16]. The ability for a given active ingredient to penetrate the stratum corneum (SC) depends on several factors [16–19]:
-
Condition of the skin barrier.
-
Physicochemical properties of the active ingredient.
-
Partitioning of the active ingredients between vehicle and skin.
-
Concentration of active ingredient dissolved into the vehicle and its subsequent thermodynamic activity.
The condition of the skin barrier and the physicochemical properties of the active ingredient (e.g. shape, size, lipophilicity, charge) are key factors to consider when designing new topical therapies. The physicochemical properties of the active ingredients and vehicle influence the partition of the active ingredients between vehicle and skin. To enhance penetration of the active ingredient, approaches such as addition of chemical penetration enhancers have been used [20, 21], however these can result in drying of the skin, irritation or inflammatory reactions [20, 22, 23].
The rate of skin penetration is proportional to the concentration of dissolved active ingredients in the vehicle as increased thermodynamic activity drives the active ingredients into the skin [16]. Several studies have shown increased skin penetration or clinical effect of topical therapies with more versus less dissolved active ingredient in a vehicle [7, 24, 25]. Various ways of increasing the ratio of dissolved:solid active ingredient in a vehicle have been described previously [16, 18, 26]. One method to dissolve more active ingredient is to prepare a supersaturated solution of the active ingredient in the vehicle, thus increasing the concentration of dissolved active ingredient and subsequently increasing the thermodynamic activity of the drug. However, for the system to be effective in a clinical setting, the supersaturation should be stable for clinically relevant time ranges, e.g. 24 h, and should not readily form crystals, as crystallization will decrease penetration of the active ingredient [16].
Occlusion, by plastic wraps, tape, impermeable dressings or vehicles containing fats or polymer oils, are well-known methods to increase the effect of a topical therapy. The SC effectively limits water evaporation from the body [17, 27] and its permeability and hydration depend on the activity of water on the outer surface [28]. Thus, occlusion of the skin will alter the SC hydration level and can subsequently increase the permeability of drugs [28, 29].
The Cal/BD aerosol foam and ointment contain the same active ingredients and pharmaceutical excipients, except for the propellents of the aerosol foam. None of the excipients are considered chemical penetration enhancers, and the two formulations are used to treat the same disease. Thus, the condition of the skin, physicochemical properties of the active ingredients and vehicles, and chemical penetration enhancers will not be considered further.
The objective of this study is to investigate the factors influencing skin penetration of the active ingredients in the two formulations; specifically to assess whether the stable supersaturated solution of the active ingredients and/or occlusive properties of Cal/BD aerosol foam account for the observed increased clinical efficacy compared with Cal/BD ointment.
Methods
Solubility Studies
Solubility curves for Cal and BD as a function of percentage DME in the propellant composition (w/w) were constructed. Solutions were prepared by adding varying amounts of DME and butane (totaling 47 mL) to compositions containing 13 mg Cal (as monohydrate), 67 mg BD and 20 g vehicle base (liquid paraffin, white soft paraffin and PPG-11-stearyl ether). Samples were shaken vigorously until the contents appeared homogenous, after which they were left overnight, resulting in sedimentation. Samples for analysis were taken from the top of the composition, placed in a water bath at 40 °C for 5 h until the propellant had fully evaporated, and subsequently cooled for 1 h at room temperature. The amount of Cal and BD present in each sample was determined using high-performance liquid chromatography.
Evaporation Studies
The evaporation of DME and butane from the sprayed dose of Cal/BD aerosol foam was determined following passive evaporation. Samples were obtained by spraying 0.20 g Cal/BD aerosol foam (equivalent to 0.08 g foam base) onto a piece of paper, which was then spread to obtain an even surface. The samples were then allowed to stand for passive evaporation, thereby mimicking the intended clinical administration of the product. At appropriate time points samples were withdrawn for analysis. The experiment was performed in triplicate at an ambient temperature (20–25 °C). For determination of the initial amount of propellants in the sprayed dose, additional samples were prepared: (i) by capturing all Cal/BD aerosol foam base and propellants expelled by spraying directly into gas-tight vials; and (ii) by transferring the sample into gas-tight vials after escape of propellants not bound to the foam base in the sprayed dose, obtained by spraying Cal/BD aerosol foam onto a piece of paper and allowing it to stand for 30 s.
The amount of propellants present in the samples of Cal/BD aerosol foam was determined quantitatively using a gas chromatography headspace method with flame ionization detection, which allowed for simultaneous measurements of the two propellants.
Identification of Crystals and/or Crystal Formation
The Cal/BD aerosol foam and ointment samples were prepared for crystal identification by placing a small amount of the product on an objective glass and smearing it with a cover glass to obtain a thin film. Cal/BD aerosol foam was assessed as a function of time whereas Cal/BD ointment, a static system, was assessed immediately after application. For optical microscopy, the sample was placed under a Leica M205 stereomicroscope (Leica Microsystems GmbH, Wetzlar, Germany) equipped with circular polarizers and viewed in transmitted light; pictures were taken at 200× magnification.
For the Raman imaging, the sample was placed under a Renishaw Invia Raman microscope (Renishaw plc, Gloucestershire, United Kingdom) and viewed in both reflected and transmitted light. Reference spectra of Cal monohydrate, Cal anhydrate, BD and two placebo formulations (ointment and aerosol foam) were acquired as single-point measurements. Streamline imaging maps were made on both sample types. For the aerosol foam, the same area of the sample was then scanned at different time points, creating a series of maps that would demonstrate if solid particles of BD or Cal had formed. The time study continued for 26 h and the recorded image size was up to 100 × 300 µm with a spartial resolution of 2 × 2 μm or 3 × 3 μm.
X-ray powder diffraction (XRPD) patterns were collected with a PANalytical Empyrian diffractometer (Panalytical, Almelo, The Netherlands). Cal/BD aerosol foam and ointment diffraction patterns were measured in the sample holder 7 days and 5 min after application, respectively, and compared against reference patterns for Cal monohydrate, Cal anhydrate and BD. The XRPD patterns were collected in the 2-theta range from 5° to 17°, with a stepsize of 0.013° and a counting time of 11,993 s. Furthermore, the sample was spun to ensure better particle statistics.
In Vitro Penetration Analysis
Foam formulations with different ratios of DME:butane were prepared (Table 1) by filling aerosol containers with the vehicle base, crimping the valves and adding the propellants through the valves.
The concentrations of Cal and BD in the foam compositions, pre-application (as a solution in the can) and post-application (in the sprayed foam), are shown in Table 2.
The in vitro penetration of Cal and BD was studied as a function of percentage DME in the composition into and through intact pig ear skin using the preparations above (Table 1). PermeGear® (PermeGear Inc, Hellertown, PA, USA) diffusion cells (n = 6), with a recipient phase consisting of 0.04 M isotonic phosphate buffer (pH 7.4) and 4% bovine serum albumin, were used. The formulations (6 mg/cm2) were applied to the pig ear skin and samples were collected after 21 h. Non-absorbed medication was removed with a cotton swab, followed by tape-stripping twice using Transpore® (3M, St. Paul, MN, USA) tape. The skin biopsy was subsequently added to a digestion buffer of proteinase K enzyme and placed in a water bath for pulsatory sonication. A sample from the resulting homogenate and from the recipient fluid was precipitated with ethanol and methanol, respectively, prior to analysis. Concentrations of Cal and BD were assessed using liquid chromatography-mass spectrometry to determine distributions of the active ingredients. A non-parametric analysis of variance (Kruskal-Wallis) was used to analyze the influence of % DME in the composition on the amount of Cal and BD in the skin and the recipient fluid. P values below 0.05 were considered to be statistically significant.
Human Skin Explant Biomarker Study
Anonymized human skin samples from abdominoplasty surgery were acquired from Biopredic International, France (female donor, 53 years old) and from the Department of Plastic Surgery, Herlev Hospital, Denmark (male donors, 29 and 53 years old) upon written informed consent of the donors. For each donor, 16 µL of Cal/BD aerosol foam (n = 6), ointment (n = 6) or vehicle (n = 3) were applied to full-thickness skin in a static PermeGear diffusion cell setup (total of three donors). After 21 h, biopsies were taken to assess the bioavailability of Cal and BD in the living layers of the skin. The gene expression of cytochrome P450 24A1 (CYP24A1), which is induced upon target engagement of the vitamin D receptor, was used to monitor the bioavailability of Cal in the skin. The reference genes PPIA, GAPDH and ACTB were used for normalization. The percentage of B-17-P, a metabolite of BD primarily formed in the viable layers of the skin, was measured in relation to total BD in the epidermis. A two-way ANOVA test was used to analyze the influence of donor and formulation on the amount of CYP24A1 mRNA and B-17-P in the skin.
Occlusion Studies
Beakers (50 mL) were filled with milliQ water and covered with pig ear skin (separated from the fat and cartilage) so skin was in contact with the water. The skin samples were secured using plastic strips and placed on a 35 °C heating plate at a room temperature of 23 °C and humidity of 33%. The skin was allowed to equilibrate for 20 min before baseline transepidermal water loss (TEWL) measurements were taken (expressed as g/m2/h). For each skin sample, 0.14 g of each formulation was spread on an area of 7 cm2. After 5 min, the TEWL values were measured non-invasively by gently placing a vapometer (Delfin, Kuopio, Finland) on the skin. The measurements were comprised of mean values from five skin samples, and each were measured three times with the vapometer. The percentage evaporation compared with untreated skin was determined as (TEWL[after application]/TEWL[baseline] × 100).
Results
Solubility Studies
In order to obtain a formulation in which the active ingredients are dissolved in the propellants, the solubility of the active ingredients in various compositions of DME and butane was determined.
The solubility of Cal and BD appears to rise with increasing concentrations of DME and decreasing concentrations of butane (Fig. 1). An estimated minimum of 6% and 11% of DME in the composition (w/w) is required to dissolve Cal and BD, respectively. The percentage of DME in the final Cal/BD aerosol foam is 27% (Table 1). Thus, the BD and Cal available in the Cal/BD aerosol foam are completely dissolved at this ratio.

Solubility of a Cal and b BD as a function of % DME in composition (w/w). The solubility of Cal (a) or BD (b) does not increase beyond 18% or 27% DME, respectively, as all added Cal or BD is dissolved; potentially the solubility could be increased further at higher % DME compositions. The dotted lines show the solubility of Cal or BD in the final Cal/BD aerosol foam (27% DME of composition), and the dashed lines illustrates the strength of Cal and BD in the aerosol foam (20 µg/g Cal and 0.264 mg/g BD, corresponding to 50 µg/g Cal and 0.5 mg/g betamethasone, respectively, in the sprayed foam). BD betamethasone dipropionate, Cal calcipotriene, DME dimethyl ether
Evaporation Studies
To investigate the amount of solvent remaining in the sprayed foam, an evaporation study was conducted. Evaporation of DME and butane in Cal/BD aerosol foam as a function of time is depicted in Fig. 2. DME had a faster evaporation rate than butane at room temperature (20 °C; vapor pressure 510 vs 220 kPa, respectively). Within 30 s, the amount of DME was reduced to <2% of the initial amount by passive evaporation, corresponding to 4 mg/g foam base. Within 2 min of application, the total amount of DME and butane was reduced to 0.5% and 4% of the initial dose, respectively (Fig. 2).

Evaporation of DME and butane over time. DME had a faster evaporation rate than butane and within 2 min the total amount of DME and butane had reduced to 0.5% and 4% of the initial amount, respectively. DME dimethyl ether
Identification of Crystals and/or Crystal Formation
After the propellants have evaporated the active ingredients can either remain in solution to create a supersaturated solution, or crystallize. The foam and ointment were analyzed to identify crystals.
Microscopic images of Cal/BD ointment showed both Cal (needle-shaped) and BD (small corn-shaped) crystals immediately after application. In contrast, crystals were not observed in microscopic images of Cal/BD aerosol foam up to 18 hours after application. After 15 days crystals were observed (Fig. 3). These observations were supported by Raman imaging, where Cal and BD crystals were identified in Cal/BD ointment but not in the CaI/BD aerosol foam within the time frame of 26 h after application (Fig. 4). XRPD patterns of Cal and BD as reference, and Cal/BD aerosol foam and Cal/BD ointment patterns are shown in Fig. 5. Patterns of Cal/BD foam and Cal/BD ointment were captured 7 days after application to the sample holder and BD diffraction patterns were not detected in the Cal/BD aerosol foam formulation; however, it was identified in Cal/BD ointment. Cal crystals were not detected as concentrations were below the limit of detection.

Microscopic imaging. a Microscopic images of Cal/BD ointment, where both Cal (needle-shaped) and BD (small corn-shaped) crystals are observed when the formulation is applied. b Microscopic images of Cal/BD aerosol foam over time. No Cal or BD crystals were observed up to 18 hours after application. After 15 days crystals were observed. BD betamethasone dipropionate, Cal calcipotriene

Raman imaging. Left Overlay Raman image map identifying a needle-shaped Cal crystal and a small corn-shaped BD crystal in the Cal/BD ointment at application. Pixel size: 3 × 3 µm. Right Overlay Raman image map of Cal/BD aerosol foam at 26 h after application; no cal or BD crystals could be identified. Pixel size: 2 × 2 µm. Cal is shown in green, BD in red and vehicle in blue. BD betamethasone dipropionate, Cal calcipotriene

Comparison of the XRPD patterns of Cal (monohydrate and anhydrate) and BD with the pattern of Cal/BD ointment and aerosol foam, 7 days after application. BD crystals were observed in the ointment, while no crystals were observed in the aerosol foam, even after 7 days. The amount of Cal crystals in suspension were below the limit of detection. BD betamethasone dipropionate, Cal calcipotriene, XRPD X-ray powder diffraction
In Vitro Penetration Analysis
Penetration of Compositions of Increasing DME Concentrations
The percentage of BD penetrated into the skin is significantly higher with formulation B containing 32% (6.8 ± 1.8%) and formulation C containing 40% (7.2 ± 2.3%) DME compared with the Cal/BD ointment (2.5 ± 1.2%, illustrated as 0% DME in Fig. 6). The percentage of BD from formulation A containing 9% of DME was not statistically significantly different to all other formulations investigated.

Penetration of BD into skin or receptor medium as a function of percentage DME of composition (w/w; mean ± SD). Penetration of BD from the Cal/BD ointment is indicated by 0% DME and open symbols. BD betamethasone dipropionate, Cal calcipotriene, DME dimethyl ether
Similar results were observed for Cal in in vitro skin penetration experiments: higher Cal skin penetration occurred as % DME in the formulation increased from 0 (Cal/BD ointment) to 32% DME (formulation B; data on file, LEO Pharma A/S).
Penetration of the Final Cal/BD Aerosol Formulation Compared with the Ointment
A concentration of 27% DME in the composition was chosen for the final Cal/BD aerosol foam formulation.
Administration of the final Cal/BD aerosol foam formulation led to significantly higher levels of Cal (P < 0.001) and BD (P = 0.002) in pig ear skin compared with ointment (Table 3). The levels of Cal and BD that permeated through the skin into the recipient phase were generally very low or below the level of detection, with the exception of Cal at 21 h (aerosol foam, 34 ± 13%; ointment 15 ± 12%; P = 0.026 between products).
Human Skin Explant Biomarker Study
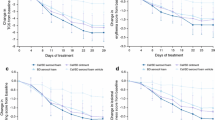
Treatment for 24 h with Cal/BD ointment and Cal/BD aerosol foam strongly induced the gene expression of CYP24A1 compared with the vehicle control (Fig. 7a). Treatment with Cal/BD aerosol foam resulted in higher expression levels of CYP24A1 than Cal/BD ointment (Fig. 7a). Similarly, the relative amounts of B-17-P after application of Cal/BD aerosol foam were higher than after application of Cal/BD ointment (Fig. 7b). In summary, the bioavailability of both Cal and BD in the living layers of the skin was higher after Cal/BD aerosol foam application compared with Cal/BD ointment, although this effect was not statistically significant using a total of three donors.

Bioavailability of Cal and BD in the skin a CYP24A1 mRNA, and b % B-17-P of total BD-related material in human skin samples (mean ± SD; n = 3 donors). BD betamethasone dipropionate, Cal calcipotriene
Occlusion Studies
The TEWL measurements from pig ear skin through the Cal/BD aerosol foam and Cal/BD ointment compared with untreated skin is shown in Fig. 8. The Cal/BD ointment tends to be more occlusive than the Cal/BD aerosol foam, although this was not statistically significant. Both formulations were shown to have extensive occlusive properties.

Evaporation of water from skin following no treatment, Cal/BD aerosol foam or Cal/BD ointment (mean ± SD). BD betamethasone dipropionate, Cal calcipotriene, SD standard deviation
Discussion
Clinical studies have shown Cal/BD aerosol foam to be more efficacious than Cal/BD ointment in patients with psoriasis vulgaris [9, 13]. In this study we have investigated the factors influencing skin penetration of the active ingredients in the two formulations.
Supersaturated cutaneous formulations using DME as the volatile solvent have not been investigated before. DME and butane, commonly used as propellants in hair sprays, deodorants and other consumer products, are liquids when under high pressure and gases when exposed to atmospheric pressure. In the pressurized aerosol foam formulation, DME serves as a solvent for the vehicle base as well as the active ingredients, Cal and BD. The solubility studies showed that the amount of DME in the Cal/BD aerosol foam ensures the active ingredients are fully dissolved inside the container. The change in concentration of dissolved Cal and BD from a pressurized liquid state in the can to a foam state on the skin, is illustrated in Fig. 9.

Change in concentration of active ingredients dissolved in the aerosol foam formulation over application time. BD betamethasone dipropionate, Cal calcipotriene
As the aerosol foam is sprayed from the can and the formulation is no longer under pressure, DME and butane undergo phase transition and evaporate as gas. We found that a very limited amount of DME and butane remained in the foam 2 min after application. The rapid evaporation allows the dissolved Cal and BD to be distributed in the sprayed foam on the skin as a supersaturated solution. Supersaturated solutions can often be unstable and crystallize readily [20, 30]; however, the lack of crystallization of Cal and BD in the sprayed foam observed in this study illustrates the formation of a supersaturated environment that is stable during clinical use.
It is evident from our data that a greater amount of Cal and BD from the supersaturated solution of Cal/BD foam diffuses into the skin compared with Cal/BD ointment. We also showed that the degree of skin penetration depends on the amount of the active ingredients dissolved in the propellant mixture, as shown by increasing the % DME of composition. When fully dissolved (Cal/BD aerosol foam), the penetration of active ingredients exceeds that in which the active ingredients are partly suspended (Cal/BD ointment).
In addition, we investigated the bioavailability of Cal and BD in human skin, which supported an increased penetration of Cal/BD aerosol foam into the skin compared with Cal/BD ointment. Both the ointment and the sprayed foam were found to be occlusive. Although this finding supports the clinical efficacy of both fixed combination Cal/BD products, alone it does not explain why Cal/BD aerosol foam is more effective than ointment.
Conclusion
In conclusion this study shows that a stable supersaturated solution of the active ingredients is formed when the solvent for the active ingredients evaporates rapidly after application. This phenomenon leads to greater skin penetration of the active ingredients and thereby an increased bioavailability explaining the superior efficacy of Cal/BD aerosol foam compared to the ointment.
References
Menter A, Gottlieb A, Feldman SR, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. J Am Acad Dermatol. 2008;58:826–50.
Schön MP, Boehncke W-H. Psoriasis. N Engl J Med. 2005;352:1899–912.
Menter A, Korman NJ, Elmets CA, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. Section 3. Guidelines of care for the management and treatment of psoriasis with topical therapies. J Am Acad Dermatol. 2009;60:643–59.
Laws PM, Young HS. Topical treatment of psoriasis. Expert Opin Pharmacother. 2010;11:1999–2009.
Thorneloe RJ, Bundy C, Griffiths CE, Ashcroft DM, Cordingley L. Adherence to medication in patients with psoriasis: a systematic literature review. Br J Dermatol. 2013;168:20–31.
Feldman SR, Horn EJ, Balkrishnan R, et al. Psoriasis: improving adherence to topical therapy. J Am Acad Dermatol. 2008;59:1009–16.
Surber C, Smith EW. The mystical effects of dermatological vehicles. Dermatology. 2005;210:157–68.
Hollesen Basse L, Olesen M, Lacour JP, Queille-Roussel C. Enhanced in vitro skin penetration and antipsoriatic effect of fixed combination calcipotriol plus betamethasone dipropionate in an innovative foam vehicle. J Invest Dermatol. 2014;134:S33 (abst 192).
Queille-Roussel C, Olesen M, Villumsen J, Lacour JP. Efficacy of an innovative aerosol foam formulation of fixed combination calcipotriol plus betamethasone dipropionate in patients with psoriasis vulgaris. Clin Drug Investig. 2015;35:239–45.
Leonardi C, Bagel J, Yamauchi P, et al. Efficacy and safety of calcipotriene plus betamethasone dipropionate aerosol foam in patients with psoriasis vulgaris—a randomized phase III study (PSO-FAST). J Drugs Dermatol. 2015;14:1468–77.
Taraska V, Tuppal R, Olesen M, Bang Pedersen C, Papp K. A novel aerosol foam formulation of calcipotriol and betamethasone has no impact on HPA axis and calcium homeostasis in patients with extensive psoriasis vulgaris. J Cutan Med Surg. 2015;20:44–51.
Lebwohl M, Tyring S, Bukhalo M, et al. Fixed combination aerosol foam calcipotriene 0.005% (Cal) plus betamethasone dipropionate 0.064% (BD) is more efficacious than Cal or BD aerosol foam alone for psoriasis vulgaris: a randomized, double-blind, multicenter, three-arm, phase II study. J Clin Aesthet Dermatol. 2016;9:34–41.
Koo J, Tyring S, Werschler WP, et al. Superior efficacy of calcipotriene and betamethasone dipropionate aerosol foam versus ointment in patients with psoriasis vulgaris—a randomized phase II study. J Dermatolog Treat. 2016;27:120–7.
Paul C, Stein Gold L, Warren RB, et al. Superior efficacy of the fixed combination calcipotriol plus betamethasone dipropionate aerosol foam versus gel, in patients with psoriasis vulgaris—the phase III PSO-ABLE study. In: 24th Congress of the European academy of dermatology and venereology. Copenhagen, Denmark, 7–11 October 2015: abst COP15-1087.
Castela E, Archier E, Devaux S, et al. Topical corticosteroids in plaque psoriasis: a systematic review of efficacy and treatment modalities. J Eur Acad Dermatol Venereol. 2012;26(Suppl 3):36–46.
Hadgraft J, Lane ME. Drug crystallization-implications for topical and transdermal delivery. Expert Opin Drug Deliv. 2016;6:817–30.
Marks R. The stratum corneum barrier: the final frontier. J Nutr. 2004;134:2017S–21S.
Barrett CW, Hadgraft JW, Caron GA, Sarkany I. The effect of particle size and vehicle on the percutaneous absorption of fluocinolone acetonide. Br J Dermatol. 1965;77:576–8.
Ghafourian T, Samaras EG, Brooks JD, Riviere JE. Validated models for predicting skin penetration from different vehicles. Eur J Pharm Sci. 2010;41:612–6.
Santos P, Watkinson AC, Hadgraft J, Lane ME. Enhanced permeation of fentanyl from supersaturated solutions in a model membrane. Int J Pharm. 2011;407:72–7.
Guy RH. Current status and future prospects of transdermal drug delivery. Pharm Res. 1996;13:1765–9.
Barry BW. Mode of action of penetration enhancers in human skin. J Control Release. 1987;6:85–97.
Smith EW, Maibach HI. Future perspectives for penetration enhancers. In: Smith EW, Maibach HI, editors, Percutaneous penetration enhancers. Boca Raton: CRC Press; 1995. p. 481–484.
Moser K, Kriwet K, Froehlich C, Kalia YN, Guy RH. Supersaturation: enhancement of skin penetration and permeation of a lipophilic drug. Pharm Res. 2001;18:1006–11.
Woodford R, Barry BW. Bioavailability and activity of topical corticosteroids from a novel drug delivery system, the aerosol quick-break foam. J Pharm Sci. 1977;66:99–103.
Coldman MF, Poulsen BJ, Higuchi T. Enhancement of percutaneous absorption by the use of volatile: nonvolatile systems as vehicles. J Pharm Sci. 1969;58:1098–102.
Schaefer H, Redelmeier TE. Skin barrier: principles of percutaneous absorption. New York: Karger; 1996.
Bjorklund S, Engblom J, Thuresson K, Sparr E. A water gradient can be used to regulate drug transport across skin. J Control Release. 2010;143:191–200.
Zhai H, Maibach HI. Effects of skin occlusion on percutaneous absorption: an overview. Skin Pharmacol Appl Skin Physiol. 2001;14:1–10.
Iervolino M, Cappello B, Raghavan SL, Hadgraft J. Penetration enhancement of ibuprofen from supersaturated solutions through human skin. Int J Pharm. 2001;212:131–41.
Acknowledgments
Sponsorship and article processing charges for this study were funded by LEO Pharma A/S. Editorial assistance was provided by Mai Kurihara PhD, Mudskipper Business Ltd, funded by LEO Pharma A/S.
We would like to thank: Gritt Rasmussen, Karina Villefrance and Anne Munch for performing the solubility measurements; Marianne Groenberg for technical assistance with the evaporation study; Lone Lerbech Dolleris for technical assistance with the XRPD data collection; Jakob Thyr, Lars Hälldahl and Feng-I Tai from Kagaku Analys AB for helping with the Raman imaging; Dina Wennike, Malene Beitzel and Tina Leonhardt Hjorth for technical assistance with skin penetration and bioavailability studies; Marianne Madvig Jensen for technical assistance with the occlusive investigation.
All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis.
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
Disclosures
M. Lind, K. T. Nielsen, L. H. Schefe, K. Nørremark, A. H. Eriksson, H. Norsgaard, B. T. Pedersen and K. Petersson are or were employees of LEO Pharma A/S when the study was conducted.
Compliance with Ethics Guidelines
Written informed consent was obtained from the donors of the skin samples.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/79D4F0607B3E1840.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Lind, M., Nielsen, K.T., Schefe, L.H. et al. Supersaturation of Calcipotriene and Betamethasone Dipropionate in a Novel Aerosol Foam Formulation for Topical Treatment of Psoriasis Provides Enhanced Bioavailability of the Active Ingredients. Dermatol Ther (Heidelb) 6, 413–425 (2016). https://doi.org/10.1007/s13555-016-0125-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-016-0125-6