
Abstract
Purpose
The aim of this study was to look specifically at patients readmitted in our previously published study. We wanted to assess the percentage of avoidable readmissions among patients receiving an early geriatric follow-up visit compared to a control group receiving usual care.
Method
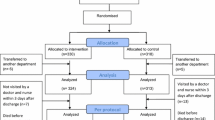
The original population was geriatric patients primarily admitted to hospital with one of nine medical diagnoses and included in a quasi randomized controlled trial. They received either an early geriatric follow-up visit or usual care after hospital discharge. Only patients with an unplanned readmission were included in this subgroup analysis. Medical records of the readmitted patients were assessed by two reviewers. Each readmission was classified as either avoidable or unavoidable. An avoidable readmission was defined as being clinically related to index admissions.
Results
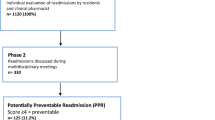
Between June 2014 and November 2015, 2076 patients were included in the original study. Of these, 216 patients were readmitted. Almost half of avoidable readmissions happened during the first week after hospital discharge. Thirty-four (41%) of 83 readmissions in the intervention group were assessed as avoidable compared to 72 (54%) of 133 readmissions in the control group (p = 0.06).
Conclusion
An early follow-up visit after hospital discharge seems to reduce avoidable readmissions among geriatric patients.


Similar content being viewed by others
References
Pedersen MK, Nielsen GL, Uhrenfeldt L, Rasmussen OS, Lundbye-Christensen S (2017) Description of OPRA: a danish database designed for the analyses of risk factors associated with 30-day hospital readmission of people aged 65 + years. Scand J Public Health 45(6):595–604. https://doi.org/10.1177/1403494817715399
Benbassat J, Taragin M (2000) Hospital readmissions as a measure of quality of health care: advantages and limitations. Arch Intern Med 160(8):1074–1081
Burke D, Link N, Bails D, Fang Y, Janjigian MP (2016) A taxonomy of seven-day readmissions to an urban teaching hospital. J Hosp Med 11(1):33–38. https://doi.org/10.1002/jhm.2481
Goldfield NI, McCullough EC, Hughes JS et al (2008) Identifying potentially preventable readmissions. Health Care Financ Rev 30(1):75–91
Clarke A (1990) Are readmissions avoidable? BMJ 301(6761):1136–1138
van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ (2011) Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ 183(7):E391–E402. https://doi.org/10.1503/cmaj.101860
van Walraven C, Jennings A, Forster AJ (2012) A meta-analysis of hospital 30-day avoidable readmission rates. J Eval Clin Pract 18(6):1211–1218. https://doi.org/10.1111/j.1365-2753.2011.01773.x
Koekkoek D, Bayley KB, Brown A, Rustvold DL (2011) Hospitalists assess the causes of early hospital readmissions. J Hosp Med 6(7):383–388. https://doi.org/10.1002/jhm.909
Balla U, Malnick S, Schattner A (2008) Early readmissions to the department of medicine as a screening tool for monitoring quality of care problems. Medicine (Baltimore) 87(5):294–300. https://doi.org/10.1097/md.0b013e3181886f93
Auerbach AD, Kripalani S, Vasilevskis EE et al (2016) Preventability and causes of readmissions in a national cohort of general medicine patients. JAMA Intern Med 176(4):484–493. https://doi.org/10.1001/jamainternmed.2015.7863
Edmans J, Bradshaw L, Franklin M, Gladman J, Conroy S (2013) Specialist geriatric medical assessment for patients discharged from hospital acute assessment units: randomised controlled trial. BMJ 347:f5874. https://doi.org/10.1136/bmj.f5874
Naylor MD, Hirschman KB, Hanlon AL et al (2014) Comparison of evidence-based interventions on outcomes of hospitalized, cognitively impaired older adults. J Comp Eff Res 3(3):245–257. https://doi.org/10.2217/cer.14.14
Caplan GA, Williams AJ, Daly B, Abraham K (2004) A randomized, controlled trial of comprehensive geriatric assessment and multidisciplinary intervention after discharge of elderly from the emergency department—the DEED II study. J Am Geriatr Soc 52(9):1417–1423. https://doi.org/10.1111/j.1532-5415.2004.52401.x
Coleman EA, Parry C, Chalmers S, Min SJ (2006) The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 166(17):1822–1828. https://doi.org/10.1001/archinte.166.17.1822
Sejr Kirring L, Gregersen M, Damsgaard EM (2013) Can readmissions be reduced by a hospital-at-home multidisciplinary geriatric team? Eur Geriatr Med 4:S170
Pedersen LH, Gregersen M, Barat I, Damsgaard EM (2016) Early geriatric follow-up after discharge reduces readmissions—a quasi-randomised controlled trial. Eur Geriatr Med 7(5):443–448. https://doi.org/10.1016/j.eurger.2016.03.009
Ouslander JG, Bonner A, Herndon L, Shutes J (2014) The interventions to reduce acute care transfers (INTERACT) quality improvement program: an overview for medical directors and primary care clinicians in long term care. J Am Med Dir Assoc 15(3):162–170. https://doi.org/10.1016/j.jamda.2013.12.005
Kane RL, Huckfeldt P, Tappen R et al (2017) Effects of an intervention to reduce hospitalizations from nursing homes: a randomized implementation trial of the INTERACT program. JAMA Intern Med 177(9):1257–1264. https://doi.org/10.1001/jamainternmed.2017.2657
Bianco A, Mole A, Nobile CG, Di Giuseppe G, Pileggi C, Angelillo IF (2012) Hospital readmission prevalence and analysis of those potentially avoidable in southern Italy. PLoS One 7(11):e48263. https://doi.org/10.1371/journal.pone.0048263
Munshi SK, Lakhani D, Ageed A, Evans SN, Mackness E (2002) Readmissions of older people to acute medical units. Nurs Older People 14(1):14–16. https://doi.org/10.7748/nop2002.03.14.1.14.c2195
van Walraven C, Jennings A, Taljaard M et al (2011) Incidence of potentially avoidable urgent readmissions and their relation to all-cause urgent readmissions. CMAJ 183(14):E1067–E1072. https://doi.org/10.1503/cmaj.110400
Gohil SK, Datta R, Cao C et al (2015) Impact of hospital population case-mix, including poverty, on hospital all-cause and infection-related 30-day readmission rates. Clin Infect Dis 61(8):1235–1243. https://doi.org/10.1093/cid/civ539
Funding
The research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There were no conflicts of interest.
Ethical approval
The study was reviewed by The Ethical Committee in The Central Denmark Region and was performed in accordance to the ethical standards of the Helsinki declaration. The Ethical committee approved that patients did not sign a consent form, because of the organizational design. Patients could decline to participate in the study at any time.
Informed consent
For this type of study formal consent is not required.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Pedersen, L.H., Brynningsen, P., Foss, C.H. et al. Avoidable readmissions seem to be reduced by early follow-up visits for geriatric patients discharged from hospital. Eur Geriatr Med 9, 613–621 (2018). https://doi.org/10.1007/s41999-018-0078-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41999-018-0078-7