
Abstract
Pathological gambling (PG) is associated with maladaptive perseverative behavior, but the underlying mechanism and neural circuitry is not completely clear. Here, the hypothesis was tested that PG is characterized by response perseveration and abnormalities in reward and/or punishment sensitivity in the ventral frontostriatal circuit. Executive functioning was assessed to verify if these effects are independent of the dorsal frontostriatal circuit. A group of smokers was also included to examine whether impairments in PG generalize to substance use disorders. Response perseveration and reward/punishment sensitivity were measured with a probabilistic reversal-learning task, in which subjects could win and lose money. Executive functioning was measured with a planning task, the Tower of London. Performance and fMRI data were acquired in 19 problem gamblers, 19 smokers, and 19 healthy controls. Problem gamblers showed severe response perseveration, associated with reduced activation of right ventrolateral prefrontal cortex in response to both monetary gain and loss. Results did not fully generalize to smokers. Planning performance and related activation of the dorsal frontostriatal circuit were intact in both problem gamblers and smokers. PG is related to response perseveration and diminished reward and punishment sensitivity as indicated by hypoactivation of the ventrolateral prefrontal cortex when money is gained and lost. Moreover, intact planning abilities and normal dorsal frontostriatal responsiveness indicate that this deficit is not due to impaired executive functioning. Response perseveration and ventral prefrontal hyporesponsiveness to monetary loss may be markers for maladaptive behavior seen in chemical and nonchemical addictions.
Similar content being viewed by others


INTRODUCTION
Pathological gambling (PG) is a psychiatric disorder with an estimated lifetime prevalence of 0.4–1.6% in the United States and Canada (Petry et al, 2005; Slutske, 2006). It is associated with psychosocial problems (Lejoyeux et al, 2002), criminal offences (Rosenthal and Lorenz, 1992), and sometimes even suicide (Petry and Kiluk, 2002). Although classified as an impulse control disorder (American Psychiatric Association, 1994), PG is often considered a behavioral addiction (Petry, 2006; Potenza, 2006; Tamminga and Nestler, 2006) and shares many clinical characteristics with substance dependence, such as psychiatric comorbidity (Petry et al, 2005), genetic vulnerability (Eisen et al, 2001; Ibanez et al, 2003), and responsiveness to specific pharmacological treatments (Eisen et al, 2001; Grant and Kim, 2006; Hollander et al, 2005b; Ibanez et al, 2003). An alternative view emphasizes the similarities between PG and obsessive-compulsive disorder (OCD; Hollander et al, 2007).
Neuroimaging studies in PG are sparse and have demonstrated increased cue reactivity in response to gambling cues similar to alcohol and drug craving (Crockford et al, 2005; Potenza et al, 2003b). In addition, decreased ventral frontostriatal activation relative to control subjects was reported in a Stroop task measuring attention and inhibition (Potenza et al, 2003a) and in a gambling task using monetary reward (Reuter et al, 2005). Finally, in an FDG-PET study, gambling for money led to a higher relative metabolic rate than gambling for points only in pathological gamblers, confirming the relevance of monetary reward in PG (Hollander et al, 2005a).
The ventral frontostriatal reward circuit has been implicated in the development and maintenance of drug addiction (Volkow et al, 2004). Reduced activation of this circuit in response to monetary reward has also been reported in PG (Reuter et al, 2005), suggesting that PG is characterized by a similar blunted response to rewarding stimuli as found in substance dependence. The Reuter et al study, however, employed a gambling paradigm in which the subject had no influence on receiving reward or punishment; moreover, no neutral stimuli were presented. Therefore, neither reward-based learning nor separate contributions of reward and punishment to the reported activations could be assessed. A paradigm that taps into reward and punishment evaluation, and activates ventral frontostriatal brain regions, is the probabilistic reversal-learning task (PRLT; Clark et al, 2004; Cools et al, 2002; Dias et al, 1996; O’Doherty et al, 2001, 2003; Remijnse et al, 2005; Remijnse et al, 2006). In this paradigm, subjects acquire stimulus–reward associations, after which reward and punishment contingencies are reversed and subjects have to adjust their strategy to the altered stimulus–reinforcement associations. This process is referred to as ‘affective switching’, and the inability to learn these altering associations results in response perseveration. Therefore, in the present study, not only evaluation of reward and punishment was assessed, but also its effect on behavior. Reversal learning has been largely overlooked in research on addictive behaviors (Clark et al, 2004), although a recent preliminary study reported impaired reversal learning in PG (Patterson et al, 2006).
In addition to deficits in punishment and reward evaluation, several studies have reported executive function (EF) deficits in substance use disorders (Lundqvist, 2005; Montgomery et al, 2005; Noel et al, 2001; Verdejo-Garcia and Perez-Garcia, 2007; Verdejo-Garcia et al, 2005) and, to a lesser extent, in PG (Goudriaan et al, 2006; Kertzman et al, 2006; Rugle and Melamed, 1993). EFs are supervisory cognitive functions that are mainly mediated by dorsal frontostriatal circuitry. Neuroimaging studies have found prefrontal dysfunctions during performance of EFs in substance users (Forman et al, 2004; Hester and Garavan, 2004; Kaufman et al, 2003). A key EF is planning, which is the ability to achieve a goal through a series of intermediate steps. Planning has been widely investigated with the Tower of London (ToL; Shallice, 1982). In this task, subjects rearrange colored balls on pegs from a start-state into a goal-state in as few moves as possible. Performance on the ToL has been shown to be impaired in alcohol dependence (Noel et al, 2001). Neuroimaging studies have confirmed involvement of the dorsal striatum and the dorsolateral prefrontal cortex (DLPFC) during performance of the ToL (Owen et al, 1996; van den Heuvel et al, 2003). Using a task sensitive to dorsal frontostriatal function (ie the ToL) and a task sensitive to ventral frontostriatal function (ie the PRLT) enabled us to investigate whether impairment in PRLT performance is associated with similar impairments when performing the ToL. To test whether any findings in PG generalize to another (chemical) addiction, we also included a group of substance-dependent subjects. Similar abnormalities in PG and nicotine dependence (ND) may point to a common mechanism across several types of addictive behaviors, chemical and nonchemical.
In summary, we expected response perseveration and decreased ventral frontostriatal responsiveness to reward in problem gamblers and smokers relative to healthy controls. In addition, employing the ToL, we expected diminished planning abilities and dorsal frontostriatal hypoactivation in problem gamblers and smokers, compared to healthy controls.
MATERIALS AND METHODS
Subjects
A total of 19 problem gamblers (4 left-handed), 19 smokers (3 left-handed), and 19 healthy controls (1 left-handed) participated in this study. Gamblers were recruited from two Dutch addiction treatment centers where they received cognitive behavioral therapy. Smokers and healthy controls were recruited through advertisements in local newspapers. Because most treatment-seeking gamblers are men, only male participants were included. Smokers and healthy controls were matched to the problem gamblers for age and educational level. The ethical review board of the Academic Medical Center approved the study, and all participants provided written informed consent. The main inclusion criterion for problem gamblers was current treatment for gambling problems. In addition, problem gamblers were interviewed according to DSM-IV-TR criteria using the Dutch version of section T of the Diagnostic Interview Schedule (DIS; Robins et al, 1998), to assess whether they fulfilled criteria for a formal PG diagnosis. The South Oaks Gambling Screen (SOGS; Lesieur and Blume, 1987) was administered to obtain a sensitive measure of gambling severity (Strong et al, 2003). Smokers were included if they smoked at least 15 cigarettes per day. The Fagerström interview (Heatherton et al, 1991) served as an additional measure of ND severity on a scale of 0–10. Healthy controls were all nonsmokers and were not allowed to engage in a gambling activity more than twice a year. Smokers were instructed to abstain from smoking 10 h before entering the experimental session. Similarly, gamblers were instructed to abstain from gambling at least 10 h before the start of the experimental session.
Exclusion criteria for all groups were: lifetime diagnosis of schizophrenia and psychotic episodes, 12-month diagnosis of manic disorder (section F of the Dutch Composite International Diagnostic Interview (CIDI); World Health Organization, 1997), treatment for mental disorders other than those under study in the past 12 months, use of psychotropic medication, difficulty reading Dutch, age under 18 years, positive urine screen for alcohol, amphetamines, benzodiazepines, opioids or cocaine, consumption of more than 21 standard units (10 g) of alcohol per week, history of or current: treatment by a neurologist, systemic disease, brain trauma, exposure to neurotoxic factors. Groups were mutually exclusive with regard to the psychiatric disorder under study. For instance, problem gamblers and healthy controls did not smoke (with the exception of two problem gamblers who smoked less than five cigarettes a day). Additional exclusion criteria for healthy controls and smokers, but not for problem gamblers, were: anxiety disorders (CIDI, section D), depression (CIDI, section E), OCD (CIDI, section K), post-traumatic stress disorder (CIDI, section K), and attention deficit hyperactivity disorder (ADHD), assessed with Conners’ Adult ADHD Rating Scales (CAARS; Conners et al, 1999). Severity of depressive symptoms was assessed with the Beck Depression Inventory (BDI; Beck et al, 1961). Problematic alcohol use was screened with the Alcohol Use Disorders Identification Test—Consumption (AUDIT-C; Bush et al, 1998).
Paradigms
We used a self-paced, PRLT including an affectively neutral condition (Figure 1) and a pseudorandomized self-paced version of the ToL (Figure 2). Both tasks have been described in detail elsewhere (Remijnse et al, 2005; van den Heuvel et al, 2003). The scanning session began with the reversal-learning task and ended with the ToL. In between, a structural MRI was acquired. After a break, a second scanning session was used that consisted of two other tasks (a stop-signal task and a cue reactivity task). Data from these tasks will be reported elsewhere.

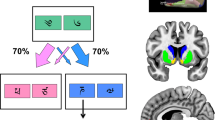
Probabilistic reversal-learning task (PRLT). During each trial two stimuli, ie a picture of a bus and a tie, were presented simultaneously at either side of a screen with randomized locations until the subject responded (3 s maximum). Subjects selected either stimulus by pressing the left or right button on a button box. Upon a correct response, either positive or negative feedback was given based on an 80 : 20 ratio, resulting in a gain or a loss of a random amount of 80–250 points. Each trial ended with a 2 s display of both the number of points won or lost in that trial and the amount of accumulated points in the task up to that trial, followed by a fixation cross for 1 s, which indicated the start of the next trial. An affectively neutral baseline task consisting of two different, equivalent stimuli in terms of visual complexity and semantic category (the picture of a car and a pair of trousers) was randomly intermixed with experimental trials, and responses in this task were given neutral feedback (‘response made’). Subjects were instructed in advance which of the two baseline stimuli to select. The task ended after 400 trials (including the baseline task) and lasted approximately 25 min. The main task instruction was to strive to obtain a maximum number of points; subjects were not encouraged to respond as quickly as possible. Subjects were informed beforehand that they could earn real money with the task. The task started with a five Euro credit. After the scanning session, participants received the total amount of accumulated points during the task divided by 1000 in Euros. To familiarize participants with the concept of probabilistic errors, before scanning subjects performed a brief version of the PRLT that did not contain reversal stages. Subjects were not informed that the actual task contained reversal stages. CR, correct response; BL, baseline trial; PENS, probabilistic error, no shift; PRE, preceding reversal error; FRE, final reversal error.

Tower of London (ToL). This version consisted of six conditions, including a baseline condition and five planning conditions of increasing difficulty, requiring planning of 1–5 moves. During the planning conditions, subjects saw a starting configuration together with a target configuration, with the instruction to ‘count the number of steps’ required to achieve the target configuration. In both configurations, three colored beads were placed on three vertical rods, which could accommodate one, two, and three beads each. One bead could be moved at a time and only when there was no other bead on top. Subjects were required to determine the minimum number of moves necessary to reach the target configuration. Two possible answers were shown. Subjects had to press the button corresponding to the side (left or right) of the screen where the correct answer was presented. In the baseline condition, subjects simply had to count the total number of yellow and blue beads. No feedback regarding the answers was provided during the task. The task was self-paced with a maximum response time for each trial of 30 s and lasted 15 min. To ensure that participants were familiar with the task, it was explained and practiced outside the scanner.
Imaging Acquisition and Preprocessing
Imaging data were obtained using a 3.0 T Intera full-body fMRI scanner (Philips Medical Systems, Best, the Netherlands) with a phased array SENSE RF six-channel receiver head coil. A total of 35 axial slices (voxel size 3 × 3 × 3 mm, interslice gap 0.3 mm, matrix size 64 × 64 mm, PRLT: TR/TE=2.50 s/30 ms, ToL: TR/TE=2.28 s/35 ms, bandwidth 90 kHz) of T2*-weighted echo planar images (EPIs), sensitive to blood oxygenation level-dependent (BOLD) contrast, were obtained, covering the entire brain except for the inferior regions of the cerebellum. Also a structural scan of 170 sagittal T1-weighed slices of the entire brain was made to co-register it with the fMRI data (voxel size 1 × 1 × 1 mm). Imaging analysis was done using SPM2 (Statistical Parametric Mapping; Wellcome Department of Cognitive Neurology, London, UK). Images were slice-timed, reoriented, and realigned to the first volume. Next, T1-co-registered volumes were normalized to an SPM T1 template and spatially smoothed using an 8 mm FWHM Gaussian kernel.
Statistical Analysis
Demographic and clinical data were analyzed using univariate analysis of variance (ANOVA) in SPSS 13.0 (SPSS Inc., Chicago, Illinois). FMRI data were analyzed in the context of the general linear model, using δ functions convolved with a canonical hemodynamic response function to model responses to each type of stimulus. Contrast images containing parameter estimates were entered into a second-level (random effects) analysis. Main effects across groups for each contrast were analyzed with one-way ANOVA implemented in SPM2 and are reported with a cluster size restriction of 10 voxels at a p<0.05 corrected for multiple comparisons according to the false discovery rate (FDR) method (Genovese et al, 2002; Remijnse et al, 2005). Group interactions are reported at p<0.001, masked with the appropriate main effect at p<0.05.
PRLT
FMRI data for one smoker were corrupt for the PRLT due to scanner failure. Therefore, 18 instead of 19 smokers were used for analysis of this task. To ensure adequate power, for each subject a minimum of 10 trials per condition were required for fMRI analyses. As a result, for calculation of the reward–baseline contrast, 5 problem gamblers had to be excluded, leaving 14 problem gamblers for analysis. For calculation of the reversal–baseline contrast, 2 smokers and 8 gamblers had to be excluded, leaving 16 smokers and 11 gamblers for analysis. ANOVA was used to analyze behavioral data (amount of money won and mean reaction time (MRT) with Group (problem gamblers, smokers, and healthy controls) as between-subject factor. For fMRI analyses, the following events were modeled to feedback onset: neutral feedback, monetary gain, monetary loss (not followed by reversal), monetary loss followed by reversal, and monetary gain followed by a reversal (regressor of no interest). The following contrasts were computed: monetary gain vs baseline, monetary loss vs baseline, and monetary loss followed by a reversal vs baseline.
ToL
For the ToL, one smoker failed to comply with task instructions and fMRI data from one smoker were corrupt due to scanner failure. Therefore, 17 smokers were used for analysis of this task. A mixed model ANOVA was used to investigate performance differences (number of correct responses and MRT) between the three groups, with Group as a between-subject factor (three levels) and Difficulty as a within-subject factor (five levels). For the fMRI analyses, the following six events were modeled to stimulus onset: baseline, one step, two steps, three steps, four and five steps, erroneous response (regressor of no interest). For each subject, two contrasts were computed: all steps vs baseline and a parametric contrast for increasing task difficulty, not taking into account the baseline trials.
RESULTS
Demographic and Clinical Results
Table 1 summarizes demographic and clinical characteristics for the problem gamblers, smokers, and healthy controls. The three groups did not differ with regard to age and educational level. Of the 19, 15 (79%) problem gamblers were diagnosed with lifetime PG; 12 of them (63%) also met the criteria for this disorder in the past 12 months. Fagerström scores indicated medium ND for the smokers, as well as for the two problem gamblers who smoked. It should be noted, however, that all smokers smoked more than 15 cigarettes per day, whereas the two smoking problem gamblers smoked less than 5 cigarettes per day. Seven problem gamblers (37%) suffered from comorbid anxiety and depression disorders in the past 12 months. Problem gamblers obtained significantly higher scores on the CAARS and BDI compared to both smokers and healthy controls. Smokers and healthy controls did not differ on the CAARS and the BDI.
PRLT
In the PRLT, the three groups differed significantly with regard to the amount of money won (F(2, 53)=10.00, p<0.0005; Figure 3). Post hoc tests showed that problem gamblers won less money than smokers (t(19.31)=2.86, p=0.01), and smokers won less money than healthy controls (t(33.60)=2.42, p<0.05). No differences in MRT were found between the groups. Performance was significantly negatively correlated with the score on the CAARS G scale (r=−0.31, p<0.05) and the BDI (r=−0.39, p<0.005). Group differences in the amount of money earned, however, remained significant after adjusting for differences between groups in CAARS (F(2, 52)=7.22, p<0.005) and BDI scores (F(2, 52)=5.76, p<0.005). This effect also remained significant when only considering problem gamblers fulfilling a PG diagnosis for the last 12 months (n=12; F(2, 46)=5.76, p<0.005) or when analyzing only problem gamblers without comorbid anxiety or depression (n=12; F(2, 46)=4.38, p<0.05).

Amount of money earned in probabilistic reversal-learning task (PRLT). Error bars show SEM.
Monetary gain was associated with activation of right ventrolateral prefrontal cortex (VLPFC) and frontal operculum, right parietal and occipital cortex, as well as bilateral caudate nucleus and subthalamic region (Figure 4 ; Table 2). Interaction analyses revealed significantly lower VLPFC activation in problem gamblers relative to healthy controls (Figures 4 and 5). In addition, in smokers we found significantly increased activation relative to healthy controls in right insula (Figure 4), right (pre)frontal areas, and bilateral parietal regions.

Probabilistic reversal-learning task. BOLD activations (main effects) for the contrasts monetary gain–baseline and monetary loss–baseline. Activations are shown at p<0.05 uncorrected to show the extent of activity. Circle indicates hypoactive right ventrolateral prefrontal cortex (VLPFC) to monetary gain in problem gamblers compared to healthy controls, and hypoactivation of right VLPFC to monetary loss in both problem gamblers and smokers, compared to healthy controls. Square indicates hyperactivation of right anterior insula to monetary gain in smokers relative to healthy controls.

Probabilistic reversal-learning task. BOLD activations (group interactions) showing hypoactivation for problem gamblers compared to healthy controls in right ventrolateral prefrontal cortex (VLPFC) during monetary gain (left panel), and hypoactivation for both problem gamblers and smokers compared to healthy controls in right VLPFC during monetary loss (middle and right panels, respectively). Activations are shown at p<0.05 uncorrected to show the extent of activity. Lighter color indicates higher t-score.
Monetary loss was associated with activation of right frontal operculum and insular cortex, as well as subthalamic region. Problem gamblers and smokers showed significantly less VLPFC activation than healthy controls (Figures 4 and 5). Monetary loss followed by a reversal was associated with activation of right frontal operculum and right insular cortex, as well as in the subthalamic region. In addition, we observed activation of right DLPFC, right supplementary motor area (SMA), right dorsal anterior cingulate, and bilateral parietal cortex. Significant group differences were observed in controls relative to problem gamblers (cerebellum) and smokers (VLPFC), and in smokers relative to healthy controls (right frontal operculum and right insula).
ToL
A significant main effect of Difficulty (F(4, 49)=26.88, p<0.0001) showed that error rates increased with increasing planning demands. The three groups did not differ with regard to the proportion of correct responses (F(2, 52)=1.73, NS). The Difficulty by Group interaction was not significant either (F<1, NS). A significant main effect of Difficulty was found for MRT (F(4, 49)=82.17, p<0.0001), indicating longer reaction times with increasing task load. MRT was similar for the three groups (F(2, 52)=1.07, NS) and the Difficulty by Group interaction was also not significant (F<1, NS). After restricting problem gamblers to those meeting a formal PG diagnosis in the last 12 months (n=12), no significant group effects were observed either.
Imaging results showed robust activations in bilateral dorsolateral prefrontal and parietal cortex, dorsal medial prefrontal cortex, and bilateral striatum, both when comparing task vs baseline and for task load (Figure 6; Table 3). However, group comparisons failed to reveal significant interaction effects between groups with the exception of small parietal and cerebellar foci in controls relative to problem gamblers and smokers, respectively.

Tower of London BOLD activations (main effects) for the contrasts planning–baseline and parametric. Activations are shown at p<0.05, FDR corrected. Upper panel shows activation of dorsal striatum for the planning–Baseline contrast. Lower panel shows activation of dorsolateral prefrontal cortex for the parametric contrast, modeling increasing task difficulty.
Correlation Between PRLT and ToL
Amount of money won on the PRLT was not correlated with proportion of correct answers on the ToL (r=0.026, NS).
DISCUSSION
The present study aimed at investigating abnormalities in behavioral performance and in the neural circuitry underlying reward and punishment sensitivity and planning in problem gamblers, compared to smokers and healthy controls. The main finding of the present study was a failure of the problem gamblers to adequately perform the reversal task, associated with response perseveration and lower responsiveness of the right VLPFC during winning and losing money. In contrast, planning in the problem gamblers was intact as indicated by normal performance on the ToL and normal responsiveness of the dorsal frontostriatal circuitry.
Decreased Reward Responsiveness in Problem Gamblers
The brain areas activated during the PRLT have also been reported in previous studies employing reversal-learning paradigms (Cools et al, 2002; O’Doherty et al, 2001, 2003; Remijnse et al, 2005, 2006). The most relevant areas activated by monetary gain were the right VLPFC, right frontal operculum, bilateral caudate nucleus, and subthalamic region. Compared to healthy controls, problem gamblers showed decreased responsiveness of VLPFC to monetary gain. Our findings are consistent with those of Reuter et al (2005), showing hypoactivation of the ventral prefrontal cortex in pathological gamblers in response to monetary gain. Moreover, in a recent study employing a decision-making task that was similarly developed to assess responses to monetary gain and loss (the Iowa Gambling Task), decreased responsiveness of the ventral prefrontal cortex in gambling and nongambling substance-dependent subjects during decision-making was found, compared to a task in which no decision-making was required (Tanabe et al, 2007). It should be noted, however, that in these studies group differences were observed in the medial instead of lateral ventral prefrontal cortex, a brain region that was incompletely covered in our study due to signal dropout. Moreover, prefrontal hyporesponsiveness to monetary rewards has also been reported in two studies in cocaine abusers (Goldstein et al, 2007; Goldstein and Volkow, 2002).
It has been suggested that decreased dopamine function in the ventral striatum in addicted individuals results in a diminished sensitivity for drug-related as well as other rewarding stimuli. This ventrostriatal hypoactivity has been linked to increased reward-seeking behavior as a compensatory mechanism for existing reward deficiency (Blum et al, 2000). In PG this may relate to the high amounts of money spent in gambling episodes. Decreased ventrostriatal activity in turn has been found to be related to hypoactivity of the ventral prefrontal cortex (Volkow et al, 2004), which contains extensive ventrostriatal dopaminergic projections. Therefore, the current findings are consistent with the view of PG as a behavioral or nonchemical addiction. Interestingly, decreased responsiveness of the VLPFC has also been observed in patients with OCD in a study by our group, using an identical version of the PRLT (Remijnse et al, 2006). Hyporesponsiveness of the ventral prefrontal cortex to reward, therefore, seems to be a common phenomenon in both chemical and behavioral addictions on the one hand and OCD on the other hand, supporting the view that addictive behaviors and OCD may be part of an obsessive-compulsive spectrum (Hollander et al, 2007). This might be related to the maladaptive perseverative behavior that these disorders have in common.
Interestingly, the smokers were characterized by hyperresponsiveness rather than hyporesponsiveness of the insular cortex to monetary gain compared to both healthy controls and problem gamblers. In addition, in smokers we found increased activity in DLPFC, and posterior parietal cortex during rewarding feedback, indicating recruitment of higher-order cognitive functions similar to those activated during the ToL (Mitchell and Cusack, 2008; van den Heuvel et al, 2003). In this respect, smokers demonstrated an activation pattern that is atypical for addiction. A possible explanation may be that ND constitutes an atypical addiction: the percentage of individuals that develops addictive behaviors is quite low in gambling as well as in most drugs of abuse (around 15%), but the percentage of individuals that develop a dependence to nicotine is very high (Grant et al, 2004; Kessler et al, 1994). Finally, it should also be noted that the smokers had been abstinent for more than 10 h, which may also have influenced the results (Xu et al, 2006).
Decreased Punishment Sensitivity in Problem Gamblers
Punishment, ie monetary loss, was associated with activation of right insula, right frontal operculum, and subthalamic region, areas that have been reported before in studies examining the effects of abstract punishments (O’Doherty et al, 2001). In healthy controls, but not in smokers and problem gamblers, we additionally found right VLPFC activation, an area very close to the region that was hypoactive in response to reward reception in problem gamblers. The problem gamblers failed to activate right VLPFC to rewarding as well as punishing stimuli, which was coupled with a very poor performance. In contrast, smokers only failed to activate right VLPFC to punishing stimuli, associated with an intermediate performance.
Consistent with earlier reports (O’Doherty et al, 2003; Remijnse et al, 2005, 2006), punishment trials that resulted in a reversal activated a large neural network, including dorsal prefrontal areas, compared to punishing trials not resulting in a behavioral shift. When comparing problem gamblers to healthy controls only decreased activation in the left cerebellum was observed. It should be noted, however, that the worst performing problem gamblers had to be excluded from this analysis as poor performance on this learning task inherently results in too few reversal trials to allow meaningful comparisons. Although our findings in this respect thus need to be interpreted with caution, it is interesting to note that cerebellar pathology has been associated with ‘frontal-like’ impairments, for example, impaired set-shifting and planning (Bellebaum and Daum, 2007; Gottwald et al, 2004). In line with our expectations, we observed VLPFC hyporesponsiveness in smokers relative to healthy controls during reversal trials. In addition, this group also showed hyperresponsiveness of right insula and frontal operculum during reversals, compared to healthy controls. This hyperresponsiveness was also observed in response to rewarding stimuli. In the present study, ND thus seems to be characterized by a hyperresponsive right insular cortex in response to motivational feedback. Interestingly, it was recently reported that smokers who acquired brain damage in the insula find it easy to quit smoking (Naqvi et al, 2007). The present findings indicate that the insula may not only be related to the rewarding effects of smoking, but also to a general hyperresponsiveness to reward in smokers.
Intact Planning
The three groups showed a similar performance on the planning task (ToL), and a dorsal frontostriatal and parietal network was activated with increasing task difficulty in all three groups. Apparently, in the present study, problem gamblers and smokers were characterized by normal EF as shown by normal performance and intact neural responsiveness of the dorsal frontostriatal network during a planning task. Problem gamblers showed less posterior parietal activation during increasing planning difficulty with intact performance. This may indicate that less attention-related processing was involved during planning for problem gamblers than for healthy controls, pointing to mild attention deficits that are too subtle to be detected by our present performance measures. Post hoc tests on the behavioral data (not shown), however, indicated that problem gamblers performed better during the more difficult conditions of the ToL than the other groups, which makes this a less probable explanation. Alternatively, these results may thus indicate that problem gamblers are actually better at planning and therefore need to recruit the posterior parietal cortex to a lesser extent.
Smokers showed less cerebellar activation than healthy controls during overall planning. Although executive dysfunction has been linked to cerebellar pathology, as noted earlier, in the present study such an interpretation remains speculative in the absence of impaired planning abilities in smokers.
Impaired EFs have been reported in a wide range of substance use disorders (Lundqvist, 2005; Montgomery et al, 2005; Noel et al, 2001; Verdejo-Garcia and Perez-Garcia, 2007; Verdejo-Garcia et al, 2005). This may indicate that in these substance use disorders, EF impairment is the result of neurotoxicity of the drugs of abuse. In the present study, the group with the ‘behavioral addiction’ of PG did not suffer from neurotoxic damage due to substance abuse, whereas the smokers were intentionally selected because of the negligible neurotoxicity of tobacco compared to most other substance use disorders drugs of abuse (including alcohol; Mudo et al, 2007). Moreover, nicotine apparently does not interfere with BOLD signal response (Jacobsen et al, 2002). However, several other studies have reported EF impairments in PG (Goudriaan et al, 2006; Kertzman et al, 2006; Rugle and Melamed, 1993). For example, Goudriaan et al employed a ToL task and reported performance impairments in their group of pathological gamblers. Three explanations can be put forward to account for this discrepancy. First, although all problem gamblers in our study were treated for PG in an outpatient clinic, not all of them met the criteria for a formal DSM-IV PG diagnosis, whereas all gamblers in the Goudriaan et al study did. This is also reflected in higher SOGS scores in the Goudriaan et al study. Exclusion of problem gamblers that did not fulfill a 12-month PG diagnosis, however, did not change our results. Second, in the present study, a computerized ToL was used, requiring the identification of the number of correct moves, which may be less affected by impulsivity. PG is associated with behavioral impulsivity and may predispose for impulsive responding in the original ToL during the first moves (Goudriaan et al, 2006). Third, smoking status was not an exclusion criterion for the PG group in the Goudriaan et al study. Smoking is also related with impulsivity (Mitchell, 1999; Reynolds et al, 2007). The combination of smoking and problem gambling may have led to decreased performance on the ToL on the Goudriaan et al study. Therefore, in future studies it would be highly informative to also include a group of smoking problem gamblers.
Strengths and Limitations
The main strengths of the study are the relatively large sample sizes of the group, the inclusion of a control and a comparison (smokers) group, and the inclusion of a ventral and a dorsal prefrontal task in one study.
However, also some limitations of the present study should be noted. The current sample consisted of problem gamblers who were in treatment at the time of data collection, whereas the smokers were not actively seeking treatment. This may partially explain the more severe impairments in reversal learning in problem gamblers compared to smokers. Moreover, it can be argued that the higher prevalence of comorbid anxiety and/or depression in problem gamblers may have biased our results. However, omitting problem gamblers with comorbidity from the analyses did not change the pattern of results with regard to impaired reversal learning. In addition, group differences remained significant after controlling for ADHD and depression scores in the analyses.
We did not assess lifetime smoking behavior of our participants. Therefore, smoking history of the currently nonsmoking healthy controls and problem gamblers may have influenced the results. The 10 h abstinence that was required for the smokers may potentially have negatively influenced performance of this group due to withdrawal effects. The intact planning performance of the smokers argues against this explanation, however.
Inherent to the task design, in participants that performed poorly on the reversal learning task not enough reversal trials were available for reliable assessment of reversal-related BOLD activity. Therefore, whereas the reversal learning task used in the present study may be a powerful tool to detect decision-making deficits in chemical and nonchemical addictions, inability to perform the task adequately may also hamper identification of the neural substrate underlying this deficiency.
CONCLUSIONS
In the present study problem gamblers were characterized by response perseveration and hyporesponsiveness of right VLPFC to both monetary loss and gain. This aberrant functioning could not be explained by impaired EFs and concomitant abnormal activation patterns in the dorsal frontostriatal circuit. Although prospective study designs are necessary to further explore this issue, it may be speculated that ventral prefrontal hyporesponsiveness to rewarding stimuli, as exemplified by problem gamblers in this study, may be a neurocognitive marker for the development of addictive behaviors. Ventral prefrontal hyporesponsiveness to punishment, as exemplified by both problem gamblers and smokers, may be crucial in the continuation of addictive behaviors despite serious adverse consequences.
References
American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorders. American Psychiatric Association: Washington, DC.
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961). An inventory for measuring depression. Arch Gen Psychiatry 4: 561–571.
Bellebaum C, Daum I (2007). Cerebellar involvement in executive control. Cerebellum 6: 184–192.
Blum K, Braverman ER, Holder JM, Lubar JF, Monastra VJ, Miller D et al (2000). Reward deficiency syndrome: a biogenetic model for the diagnosis and treatment of impulsive, addictive, and compulsive behaviors. J Psychoactive Drugs 32 (Suppl): 1–112.
Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA (1998). The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Intern Med 158: 1789–1795.
Clark L, Cools R, Robbins TW (2004). The neuropsychology of ventral prefrontal cortex: decision-making and reversal learning. Brain Cogn 55: 41–53.
Conners CK, Erhart D, Sparrow E (1999). Conners' Adult ADHD Rating Scales, technical manual. Multi-Health Systems: New York, NY.
Cools R, Clark L, Owen AM, Robbins TW (2002). Defining the neural mechanisms of probabilistic reversal learning using event-related functional magnetic resonance imaging. J Neurosci 22: 4563–4567.
Crockford DN, Goodyear B, Edwards J, Quickfall J, el-Guebaly N (2005). Cue-induced brain activity in pathological gamblers. Biol Psychiatry 58: 787–795.
Dias R, Robbins TW, Roberts AC (1996). Dissociation in prefrontal cortex of affective and attentional shifts. Nature 380: 69–72.
Eisen SA, Slutske WS, Lyons MJ, Lassman J, Xian H, Toomey R et al (2001). The genetics of pathological gambling. Semin Clin Neuropsychiatry 6: 195–204.
Forman SD, Dougherty GG, Casey BJ, Siegle GJ, Braver TS, Barch DM et al (2004). Opiate addicts lack error-dependent activation of rostral anterior cingulate. Biol Psychiatry 55: 531–537.
Genovese CR, Lazar NA, Nichols T (2002). Thresholding of statistical maps in functional neuroimaging using the false discovery rate. Neuroimage 15: 870–878.
Goldstein RZ, Alia-Klein N, Tomasi D, Zhang L, Cottone LA, Maloney T et al (2007). Is decreased prefrontal cortical sensitivity to monetary reward associated with impaired motivation and self-control in cocaine addiction? Am J Psychiatry 164: 43–51.
Goldstein RZ, Volkow ND (2002). Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. Am J Psychiatry 159: 1642–1652.
Gottwald B, Wilde B, Mihajlovic Z, Mehdorn HM (2004). Evidence for distinct cognitive deficits after focal cerebellar lesions. J Neurol Neurosurg Psychiatry 75: 1524–1531.
Goudriaan AE, Oosterlaan J, de Beurs E, van den Brink W (2006). Neurocognitive functions in pathological gambling: a comparison with alcohol dependence, Tourette syndrome and normal controls. Addiction 101: 534–547.
Grant BF, Hasin DS, Chou SP, Stinson FS, Dawson DA (2004). Nicotine dependence and psychiatric disorders in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry 61: 1107–1115.
Grant JE, Kim SW (2006). Medication management of pathological gambling. Minn Med 89: 44–48.
Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO (1991). The Fagerstrom test for nicotine dependence: a revision of the Fagerstrom Tolerance Questionnaire. Br J Addict 86: 1119.
Hester R, Garavan H (2004). Executive dysfunction in cocaine addiction: evidence for discordant frontal, cingulate, and cerebellar activity. J Neurosci 24: 11017–11022.
Hollander E, Kim S, Khanna S, Pallanti S (2007). Obsessive-compulsive disorder and obsessive-compulsive spectrum disorders: diagnostic and dimensional issues. CNS Spectr 12: 5–13.
Hollander E, Pallanti S, Baldini RN, Sood E, Baker BR, Buchsbaum MS (2005a). Imaging monetary reward in pathological gamblers. World J Biol Psychiatry 6: 113–120.
Hollander E, Sood E, Pallanti S, Baldini-Rossi N, Baker B (2005b). Pharmacological treatments of pathological gambling. J Gambl Stud 21: 99–110.
Ibanez A, Blanco C, Perez de Castro I, Fernandez-Piqueras J, Saiz-Ruiz J (2003). Genetics of pathological gambling. J Gambl Stud 19: 11–22.
Jacobsen LK, Gore JC, Skudlarski P, Lacadie CM, Jatlow P, Krystal JH (2002). Impact of intravenous nicotine on BOLD signal response to photic stimulation. Magn Reson Imaging 20: 141–145.
Kaufman JN, Ross TJ, Stein EA, Garavan H (2003). Cingulate hypoactivity in cocaine users during a GO-NOGO task as revealed by event-related functional magnetic resonance imaging. J Neurosci 23: 7839–7843.
Kertzman S, Lowengrub K, Aizer A, Nahum ZB, Kotler M, Dannon PN (2006). Stroop performance in pathological gamblers. Psychiatry Res 142: 1–10.
Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S et al (1994). Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry 51: 8–19.
Lejoyeux M, Arbaretaz M, McLoughlin M, Ades J (2002). Impulse control disorders and depression. J Nerv Ment Dis 190: 310–314.
Lesieur H, Blume SB (1987). The South Oaks Gambling Screen (SOGS): a new instrument for the identification of pathological gamblers. Am J Psychiatry 144: 1184–1188.
Lundqvist T (2005). Cognitive consequences of cannabis use: comparison with abuse of stimulants and heroin with regard to attention, memory and executive functions. Pharmacol Biochem Behav 81: 319–330.
Mitchell DJ, Cusack R (2008). Flexible, capacity-limited activity of posterior parietal cortex in perceptual as well as visual short-term memory tasks. Cereb Cortex 18: 1788–1798.
Mitchell SH (1999). Measures of impulsivity in cigarette smokers and non-smokers. Psychopharmacology (Berl) 146: 455–464.
Montgomery C, Fisk JE, Newcombe R, Murphy PN (2005). The differential effects of ecstasy/polydrug use on executive components: shifting, inhibition, updating and access to semantic memory. Psychopharmacology (Berl) 182: 262–276.
Mudo G, Belluardo N, Fuxe K (2007). Nicotinic receptor agonists as neuroprotective/neurotrophic drugs. Progress in molecular mechanisms. J Neural Transm 114: 135–147.
Naqvi NH, Rudrauf D, Damasio H, Bechara A (2007). Damage to the insula disrupts addiction to cigarette smoking. Science 315: 531–534.
Noel X, Van der LM, Schmidt N, Sferrazza R, Hanak C, Le Bon et al (2001). Supervisory attentional system in nonamnesic alcoholic men. Arch Gen Psychiatry 58: 1152–1158.
O’Doherty J, Critchley H, Deichmann R, Dolan RJ (2003). Dissociating valence of outcome from behavioral control in human orbital and ventral prefrontal cortices. J Neurosci 23: 7931–7939.
O’Doherty J, Kringelbach ML, Rolls ET, Hornak J, Andrews C (2001). Abstract reward and punishment representations in the human orbitofrontal cortex. Nat Neurosci 4: 95–102.
Owen AM, Evans AC, Petrides M (1996). Evidence for a two-stage model of spatial working memory processing within the lateral frontal cortex: a positron emission tomography study. Cereb Cortex 6: 31–38.
Patterson JC, Holland J, Middleton R (2006). Neuropsychological performance, impulsivity, and comorbid psychiatric illness in patients with pathological gambling undergoing treatment at the CORE Inpatient Treatment Center. South Med J 99: 36–43.
Petry NM (2006). Should the scope of addictive behaviors be broadened to include pathological gambling? Addiction 101 (Suppl 1): 152–160.
Petry NM, Kiluk BD (2002). Suicidal ideation and suicide attempts in treatment-seeking pathological gamblers. J Nerv Ment Dis 190: 462–469.
Petry NM, Stinson FS, Grant BF (2005). Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry 66: 564–574.
Potenza MN (2006). Should addictive disorders include non-substance-related conditions? Addiction 101 (Suppl 1): 142–151.
Potenza MN, Leung HC, Blumberg HP, Peterson BS, Fulbright RK, Lacadie CM et al (2003a). An FMRI Stroop task study of ventromedial prefrontal cortical function in pathological gamblers. Am J Psychiatry 160: 1990–1994.
Potenza MN, Steinberg MA, Skudlarski P, Fulbright RK, Lacadie CM, Wilber MK et al (2003b). Gambling urges in pathological gambling: a functional magnetic resonance imaging study. Arch Gen Psychiatry 60: 828.
Remijnse PL, Nielen MM, Uylings HB, Veltman DJ (2005). Neural correlates of a reversal learning task with an affectively neutral baseline: an event-related fMRI study. Neuroimage 26: 609–618.
Remijnse PL, Nielen MM, van Balkom AJ, Cath DC, van Oppen P, Uylings HB et al (2006). Reduced orbitofrontal-striatal activity on a reversal learning task in obsessive-compulsive disorder. Arch Gen Psychiatry 63: 1225–1236.
Reuter J, Raedler T, Rose M, Hand I, Glascher J, Buchel C (2005). Pathological gambling is linked to reduced activation of the mesolimbic reward system. Nat Neurosci 8: 147–148.
Reynolds B, Patak M, Shroff P, Penfold RB, Melanko S, Duhig AM (2007). Laboratory and self-report assessments of impulsive behavior in adolescent daily smokers and nonsmokers. Exp Clin Psychopharmacol 15: 264–271.
Robins L, Cottler L, Bucholz K, Compton W (1998). Diagnostic Interview Schedule for DSM-IV (DIS-IV—Revision 11 Sept 1998). Washington University, School of Medicine, Department of Psychiatry: St Louis.
Rosenthal RJ, Lorenz VC (1992). The pathological gambler as criminal offender. Comments on evaluation and treatment. Psychiatr Clin North Am 15: 647–660.
Rugle L, Melamed L (1993). Neuropsychological assessment of attention problems in pathological gamblers. J Nerv Ment Dis 181: 107–112.
Shallice T (1982). Specific impairments of planning. Philos Trans R Soc Lond B Biol Sci 298: 199–209.
Slutske WS (2006). Natural recovery and treatment-seeking in pathological gambling: results of two US national surveys. Am J Psychiatry 163: 297–302.
Strong DR, Breen RB, Lesieur HR, Lejuez CW (2003). Using the Rasch model to evaluate the South Oaks Gambling Screen for use with nonpathological gamblers. Addict Behav 28: 1465–1472.
Tamminga CA, Nestler EJ (2006). Pathological gambling: focusing on the addiction, not the activity. Am J Psychiatry 163: 180–181.
Tanabe J, Thompson L, Claus E, Dalwani M, Hutchison K, Banich MT (2007). Prefrontal cortex activity is reduced in gambling and nongambling substance users during decision-making. Hum Brain Mapp 28: 1276–1286.
van den Heuvel OA, Groenewegen HJ, Barkhof F, Lazeron RH, van Dyck R, Veltman DJ (2003). Frontostriatal system in planning complexity: a parametric functional magnetic resonance version of Tower of London task. Neuroimage 18: 367–374.
Verdejo-Garcia A, Perez-Garcia M (2007). Profile of executive deficits in cocaine and heroin polysubstance users: common and differential effects on separate executive components. Psychopharmacology (Berl) 190: 517–530.
Verdejo-Garcia AJ, Lopez-Torrecillas F, guilar de AF, Perez-Garcia M (2005). Differential effects of MDMA, cocaine, and cannabis use severity on distinctive components of the executive functions in polysubstance users: a multiple regression analysis. Addict Behav 30: 89–101.
Volkow ND, Fowler JS, Wang GJ (2004). The addicted human brain viewed in the light of imaging studies: brain circuits and treatment strategies. Neuropharmacology 47 (Suppl 1): 3–13.
World Health Organization (1997). Composite International Diagnostic Interview—Version 2.1. World Health Organization: Geneva.
Xu J, Mendrek A, Cohen MS, Monterosso J, Simon S, Brody AL et al (2006). Effects of acute smoking on brain activity vary with abstinence in smokers performing the N-Back task: a preliminary study. Psychiatry Res 148: 103–109.
Acknowledgements
This study was supported by a grant from the Netherlands Organization for Health Research and Development (no. 31000056) of the Netherlands Organization for Scientific Research (NWO) and an additional grant from the Amsterdam Brain Imaging Platform (no. 2005-12). We thank Bouman GGZ Rotterdam and Jellinek Amsterdam for the recruitment of problem gamblers. We also thank Annemieke Bakker Arkema, Joost van der Meer, Caspar Müller, Cécile Overman, and Qiluan Schaafsma-Zhao for their assistance in data collection and analysis.
Author information
Authors and Affiliations
Corresponding author
Additional information
DISCLOSURE/CONFLICTS OF INTEREST
None of the authors report potential conflicts of interest.
Rights and permissions
About this article
Cite this article
de Ruiter, M., Veltman, D., Goudriaan, A. et al. Response Perseveration and Ventral Prefrontal Sensitivity to Reward and Punishment in Male Problem Gamblers and Smokers. Neuropsychopharmacol 34, 1027–1038 (2009). https://doi.org/10.1038/npp.2008.175
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/npp.2008.175
Keywords
This article is cited by
-
The protective effects of cognitive empathy and emotional empathy on gambling disorder are mediated by risk aversion and responsible gambling attitude
BMC Psychiatry (2024)
-
Assessing the mediating role of impulsivity between methamphetamine-induced psychotic disorders and increased gambling severity in methamphetamine-dependent individuals
European Archives of Psychiatry and Clinical Neuroscience (2022)
-
Decision-making inflexibility in a reversal learning task is associated with severity of problem gambling symptoms but not with a diagnosis of substance use disorder
BMC Psychology (2020)
-
Neural and neurocognitive markers of vulnerability to gambling disorder: a study of unaffected siblings
Neuropsychopharmacology (2020)
-
Reduced model-based decision-making in gambling disorder
Scientific Reports (2019)
