
Abstract
Objectives
To identify distinguishing characteristics of neonates with persistent pulmonary hypertension of the newborn (PPHN) unresponsive to inhaled nitric oxide (iNO) and evaluate the use of milrinone in this cohort.
Study design
Retrospective chart review of 99 neonates with PPHN treated with iNO over a five-year period at a quaternary neonatal intensive care unit.
Results
Neonates with iNO-unresponsive PPHN had an increased number of ventilator days (10 vs 7 days, p = 0.02), greater length of hospital stay (30 vs 22 days, p = 0.02), and increased risk of death or ECMO than iNO-responsive neonates (p = 0.03). Inhaled NO non-responders treated with milrinone had improved oxygenation (p < 0.03) and no change in systemic hemodynamics.
Conclusion
Neonates with iNO-unresponsive PPHN had worse clinical outcomes than iNO responders. Milrinone may be a safe and effective adjuvant therapy, although large-scale studies are lacking. Identifying early predictors of iNO response and novel strategies to enhance iNO responsiveness should be prioritized.
Similar content being viewed by others
Introduction
Persistent pulmonary hypertension of the newborn (PPHN) results when the normal circulatory transition fails to occur at birth, resulting in elevated pulmonary vascular resistance (PVR). The elevated pulmonary vascular pressure leads to right-to-left shunting of blood across the patent ductus arteriosus (PDA) and patent foramen ovale (PFO), resulting in hypoxemia [1,2,3]. PPHN carries mortality rates of up to 10% and is associated with long-term morbidities including high rates of neurodevelopmental impairment [4,5,6]. Inhaled nitric oxide (iNO) remains the only FDA-approved therapy for PPHN/hypoxic respiratory failure (HRF), although a large percentage of neonates do not respond to this treatment [7, 8]. Not surprising, this cohort of iNO non-responders has been a focus of study for additional therapies to prevent morbidity and mortality due to PPHN/HRF. However, studying the iNO-unresponsive group has been a challenge due to lack of a universal criteria to define iNO response in HRF, with significant variability in the literature on the method by which iNO response is defined.
Some evidence exists to support the use of milrinone, a phosphodiesterase 3 (PDE3) inhibitor, in the treatment of PPHN unresponsive to iNO. In the pulmonary vasculature, PDE3 regulates vascular tone via hydrolysis of the cyclic nucleotides, resulting in vasoconstriction [9, 10]. Animal studies demonstrate an increase in PDE3 protein expression and activity in the pulmonary vasculature following treatment with NO, and enhanced relaxation of the pulmonary vasculature with the addition of milrinone [11,12,13,14]. Additionally, case reports in neonates with PPHN show an improvement in oxygenation after the addition of milrinone to iNO, without impacting systemic perfusion [15,16,17,18]. The objective of our present study was to identify distinguishing characteristics and evaluate short-term outcomes of neonates with PPHN who respond to iNO compared to those who fail to respond to iNO at our institution, as well as to evaluate the use of milrinone in this population.
Methods
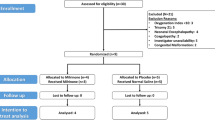
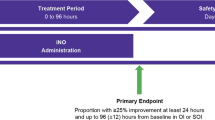
This was a retrospective study conducted at Nationwide Children’s Hospital, an all-referral Level IV neonatal intensive care unit from 2014–2019. This study was reviewed and approved by the local IRB at Nationwide Children’s Hospital. The goal of this study was to identify unique characteristics of neonates with PPHN who were iNO unresponsive. Furthermore, we aimed to determine if milrinone improved oxygenation without compromising systemic perfusion in neonates with iNO-unresponsive PPHN. We included neonates >34 weeks gestational age diagnosed with PPHN who were treated with iNO. All neonates had an oxygenation index (OI) ≥15 prior to initiation of iNO and echocardiographic evidence of PPHN at some point during the treatment period. Neonates were excluded if they had congenital heart defects (except for PDA, PFO, small atrial septal defect, or ventricular septal defect), multiple congenital anomalies, lethal genetic syndrome, pulmonary hypoplasia, or congenital diaphragmatic hernia (CDH). Neonates were also excluded if iNO was started at the birth hospital and records were not available for review. All data were extracted from the electronic medical record for the period of study, up to 48 h following the start of iNO or milrinone as applicable. In addition to demographic data, the time and duration of iNO and milrinone administration, indices of oxygenation (fraction of inspired oxygen (FiO2), partial pressure of oxygen (PaO2), OI, mean airway pressure (MAP)), and indices of systemic perfusion (heart rate, systolic blood pressure, vasopressor need) were documented. Outcome measures included air leak requiring chest tube placement, ventilator days, length of hospital stay, need for extracorporeal membrane oxygenation (ECMO), and death. The use of additional pulmonary vasodilator therapy throughout the study period was documented. Response to iNO was defined as having a 20% or greater reduction in OI and an OI < 40 at four hours after initiation of the drug. OI was calculated using the standard formula: MAP x FiO2 x 100/PaO2.
Descriptive statistics were calculated for demographic data and baseline characteristics. Continuous variables were analyzed using a t-test for parametric data or Mann–Whitney U test for nonparametric data. Categorical variables were analyzed using Chi-square or Fisher’s exact test as appropriate. One- or two-way ANOVA mixed-effects analysis was used to calculate the differences between responders and non-responders and the effects of milrinone on the reported variables. Šídák’s multiple comparisons test or Fisher’s least significant difference test was performed to compare distinct time points. A p value <0.05 was considered statistically significant. GraphPad Prism was used to complete all statistical analyses.
Results
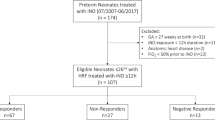
A total of 99 neonates were diagnosed with PPHN and treated with iNO during the study period. Of those 99 neonates, 60 (61%) were classified as responders and 39 (39%) as non-responders based on the study definition. There were no differences in the demographics between the two groups, including gestational age, birth weight, gender, mode of delivery, primary diagnosis, and Apgar scores at one and 5 min (Table 1). There was no difference in the mode of ventilation or percent of patients who received surfactant in the responders vs non-responders (Table 1). There was also no significant difference in the duration of iNO use between groups, with the responders receiving a mean of 110 h and the non-responders receiving a mean of 128 h (Table 1). Interestingly, there was increased use of vasopressors in the non-responder group, which correlated to greater systolic blood pressure in the non-responders vs the responders (65.8 vs 56 mmHg, p = 0.001) (Table 1). The majority of neonates showed no evidence of left or right ventricular dysfunction on the initial echocardiogram, and there was no difference between the responders and non-responders (Table 1). Sixteen of the iNO non-responders received additional pulmonary vasodilator therapy during the study period (12 received milrinone, three received inhaled iloprost, and one received inhaled treprostinil).
We compared several indices of oxygenation, including PaO2, FiO2, MAP, and OI between the two groups (Fig. 1). There were no differences in any of the indices of oxygenation prior to initiation of iNO between the iNO responders vs non-responders (Fig. 1). Compared to the non-responders, the group of iNO responders had a significantly higher PaO2 at 4 h after iNO initiation (p < 0.001). Responders also received a lower FiO2 at 4, 12, and 24 h (p < 0.01), and had a lower MAP at 4, 12, 24, and 48 h following iNO initiation (p ≤ 0.01). As expected, the overall OI was significantly higher in non-responders (32, 23, 17.1) compared to the responders (12, 11.6, 10.2) at 4, 12, and 24 h post-iNO initiation, respectively (p < 0.05).

A PaO2, (B) FiO2, (C) Mean Airway Pressure, and (D) Oxygenation Index. Data presented as means ± SEM. Two-way ANOVA mixed-effects analysis, Šídák’s multiple comparisons test; *p < 0.05, all non-responders different from responders at the specified time point; n = 26–60 for each time point.
Table 1 shows the outcome measures of iNO responders vs non-responders. Among survivors, the non-responders required increased ventilator days (median 10 vs 7, p = 0.02) and a longer length of hospital stay (median 30 vs 22, p = 0.02) compared to responders. While there was no difference between the groups in the use of ECMO or overall survival alone, the composite outcome of death or ECMO was significantly higher in the non-responders (p = 0.03). In the non-responders, the etiologies of death were intracranial hemorrhage (2), sepsis (2), pulmonary hemorrhage (1), and withdrawal of support related to ischemic brain injury (3); whereas in the responders, the cause of death was the withdrawal of support related to ischemic brain injury in all five patients.
Of the 39 non-responders, 12 (31%) received treatment with milrinone in addition to iNO (Table 2). None of the patients treated with milrinone received other pulmonary vasodilators during the study period. These neonates had an average gestational age of 38 weeks and six days, and a mean birth weight of 3549 grams. The primary diagnosis was meconium aspiration syndrome (MAS) in 9/12 (75%) neonates. The average OI was 32.2 ± 14 before starting iNO in this cohort, and 34.1 ± 15 after four hours of iNO use. The average dose and duration of milrinone were 0.36 ± 0.03 mcg/kg/min and 5.75 ± 0.9 days, and no neonates received a loading dose. Three of the neonates went on to require ECMO. Table 2 compares the demographics and clinical characteristics of the non-responders who did not receive milrinone and those who did receive milrinone. There was a difference in the gestational age at birth and birth weight between groups, with those non-responders who did not receive milrinone being younger (37 + 2/7 vs 38 + 6/7, p = 0.02) and smaller (3073 vs 3549 g, p = 0.03) than the milrinone cohort. Interestingly, there were more neonates in the milrinone cohort who were delivered by emergency cesarean section (p = 0.03) compared to those non-responders who did not receive milrinone. The median length of stay was 45 days in the non-responders who received milrinone vs 25 days in those who did not receive milrinone (p = 0.02). There was no difference between groups in the incidence of left or right ventricular dysfunction, need for ECMO, or the composite outcome of ECMO or death.
Inhaled NO non-responders who received milrinone had a statistically significant reduction in the OI at four hours after starting milrinone that persisted throughout the study period, including those who required ECMO (Fig. 2A, B, p < 0.03). They had stable hemodynamics, with no significant differences noted in heart rate or systolic blood pressure at any time during the study period (Fig. 2C, D). Additionally, there was no increased use of the vasopressors dopamine and epinephrine during the study period (Fig. 2E, F).

A Oxygenation Index, (B) Oxygenation Index of individual patients, (C) Heart rate, (D) Systolic blood pressure, (E) Dopamine, (F) Epinephrine. Data are presented as means ± SEM. One-way ANOVA mixed-effects analysis, Fisher’s LSD; *p < 0.05, different from start of milrinone time point; n = 8–12 for each time point.
Discussion
This study had two main aims: (1) To classify neonates who were iNO non-responders and identify clinical characteristics that differed from iNO responders, and (2) To establish the effects of milrinone on oxygenation and systemic perfusion in a subgroup of iNO non-responders. Overall, we found that 40% of neonates with PPHN were not responsive to iNO. There were no differences in demographics or clinical characteristics of the iNO responders vs non-responders. The non-responders had a greater number of ventilator days and length of hospital stay, and an increased risk of the composite outcome of death or ECMO compared to iNO responders. Of those patients who were non-responders, 12 (31%) were treated with milrinone in combination with iNO. Milrinone improved oxygenation without affecting systemic perfusion in these patients.
In neonates with PPHN, iNO remains the gold standard treatment to reduce PVR and improve oxygenation [1, 2, 19]. The early studies that led to the 1999 FDA approval of iNO found that low-dose iNO decreased the need for ECMO in neonates with HRF [7, 8, 19]. A 2017 meta-analysis of 17 randomized clinical trials evaluating the use of iNO in this population confirmed these findings, concluding that iNO is a safe and effective treatment for the term and near-term neonates with HRF [19]. However, these studies did not show a reduction in mortality. Despite the widespread use of iNO in neonates with HRF in recent years, mortality remains approximately 11% [19]. In previous studies, iNO did not reduce hospital length of stay [8] or improve neurodevelopmental outcomes of survivors [5, 6, 20]. Moreover, up to 50% of neonates are considered iNO non-responders and fail to show improvement in oxygenation following iNO administration [7, 8, 19]. Our findings are consistent with previous reports, with 40% of our study population meeting the criteria for iNO non-response. However, in the present study, we observed longer lengths of stay for the iNO non-responders compared to iNO responders. Our knowledge of the underlying mechanism of iNO non-response remains unclear and consequently, there are no well-studied alternative therapies for this subgroup of patients.
A major barrier in studying iNO responsiveness in neonates with HRF is a lack of universal criteria to distinguish non-responders from responders. In fact, marked differences exist in the oxygenation indices and time frames that have been used as criteria to determine iNO responsiveness in various studies (Table 3) [7, 8, 16, 17, 21,22,23,24,25,26,27]. Measures of PaO2, oxygen saturations, OI, and the need for ECMO are amongst the different indices of oxygenation used. Even more varied is the time frame following iNO administration that has been used to define responsiveness, ranging from 20 min to 24 h (Table 3). Considering this significant variability, it is plausible that neonates labeled as iNO responders in one study may be labeled iNO non-responders in another study based upon the different definitions. This is problematic as it limits our ability to further study the group of patients who do not respond to iNO. In this study, we chose to use the oxygenation index, as it is an accepted marker of HRF severity and a better indicator of lung disease as compared to PaO2 or FiO2 alone [28, 29]. We chose a time point at four hours to assess responsiveness to iNO. While many of the initial studies used shorter time points given the fast onset of action of iNO, more recent evidence suggests that some neonates may respond later [27, 30]. A recent post hoc analysis of data from the CINRGI trial showed that 12% of patients who did not respond within the defined 60 min, had a late response between 1–24 h [27]. Overall, there remains a critical need to develop a consistent and accurate definition of iNO responsiveness, taking into account indicators of oxygenation, and an appropriate time point, which remains unknown.
It is critical to develop tools that will predict iNO responsiveness given the large percentage of neonates who do not respond to iNO, the cost of iNO, as well as the invasiveness, morbidities, and healthcare-related costs associated with ECMO. To date, no studies have identified consistent variables that correlate with iNO response [7, 22, 31, 32]. Several studies have found that lower OI is associated with a better response to iNO [7, 31]. However, Roberts et al. [22] found that amongst the iNO responders, those with the highest baseline OI had the greatest reduction in OI after starting iNO. In a retrospective study designed to evaluate predictors of iNO response in neonates with HRF, Truog et al. [32] found that more iNO responders were >24 h-old at the time of iNO initiation and had a primary diagnosis of PPHN compared to non-responders. However, they found no difference in demographic factors or baseline PaO2 between the two groups [32]. Conversely, in a retrospective study of 51 neonates with PPHN, Hwang et al. [31] reported significantly higher birth weight and one-minute Apgar scores in the responder group compared to the non-responders. Non-responders also had significantly higher initial FiO2, MAP, and OI than did responders. However, a significant number of the non-responders carried a diagnosis of CDH (nine non-responders vs one responder) which likely impacted these results [31]. We found no difference in the demographics and most clinical characteristics of those neonates who responded to iNO, including mode of ventilation pre-iNO initiation, age at the time of iNO initiation (data not shown), baseline FiO2, MAP, PaO2, OI, or echocardiographic evidence of left or right ventricular dysfunction (Table 1). While there was increased use of vasopressors in the non-responder group, this was associated with a greater systolic blood pressure compared to the responders. We speculate that this increased use of vasopressors and increased systolic blood pressure may have been an attempt to overcome the intracardiac right-to-left shunting of blood seen in HRF.
As expected, by four hours after iNO initiation, there were significant differences in oxygenation indices between the two groups, with the responders having a significantly lower OI at 4, 12, and 24 h after iNO initiation compared to non-responders (Fig. 1D). Importantly, non-responders required significantly higher ventilatory support in the form of FiO2 and MAP compared to responders in the 24 h after iNO was initiated (Fig. 1B, C). At that time point, the mean PaO2 in the non-responder group was >100 mmHg, which may have reflected a failure to wean support. Furthermore, despite a lack of iNO response, this cohort received a similar, and perhaps on average a longer duration of iNO (128 vs 110 h), although not statistically significant (Table 1). We suspect that the persistent use of iNO as part of maximal medical management may reflect attempts to avoid ECMO, although it is possible that attempts to discontinue iNO resulted in worsening oxygenation. Additionally, the prolonged use of iNO despite a lack of response contributes to the increased healthcare costs and utilization, which may be reduced if those iNO non-responsive neonates could be identified prior to iNO initiation.
In contrast to previous reports, in our study iNO non-responders had an increased number of ventilator days and overall length of stay compared to the iNO responders (Table 1). Additionally, there was an increased risk of the composite outcome of death or ECMO, but not either alone (Table 1). This is an important finding as ventilator days, length of initial hospital admission, and ECMO increase resource utilization and healthcare costs and may lead to worse health outcomes. Although our data did not include long-term outcomes, based on these findings iNO non-responders are likely to be at higher risk for impaired neurodevelopment, and this should be evaluated in future studies. We speculate the difference in our findings may be related to the definition we chose for the iNO non-responder group. Nelin et al. [27] found that a moderate percentage of neonates (12%) demonstrated a late response between one to 24 h after starting iNO. Thus, some of the neonates who were labeled as non-responders in our study may have had a late response to iNO. Alternatively, it is documented that some neonates who have an initial response to iNO fail to sustain that response over time [27, 33, 34], and this may have been the case in some of our patients who were labeled as responders. Some studies classified any neonate who required ECMO during the hospitalization as iNO non-responsive [8]. Given that we were attempting to identify clinical characteristics that may predict early response to iNO to guide the use of alternative therapies, we chose to use four hours as the time point to define iNO responsiveness, regardless of the eventual need for ECMO. Furthermore, ECMO may be indicated for reasons other than pulmonary hypertension, such as refractory hypotension or cardiac dysfunction. In conclusion, there remains a critical need to identify clinical, biochemical, and genetic factors that may predict iNO responsiveness. This will aid in the development of alternative treatment strategies for iNO non-responders and for more personalized therapies to improve outcomes.
Given the large percentage of neonates with PPHN who do not respond or fail to sustain a response to iNO, there remains a need to investigate alternative treatment strategies for these groups of patients. There is emerging evidence to suggest that the PDE3 inhibitor, milrinone improves oxygenation and exhibits synergism with iNO [11, 18, 35, 36]. PDE3 regulates vascular tone via hydrolysis of both cyclic adenosine monophosphate (cAMP) and cyclic guanosine monophosphate (cGMP), leading to vasoconstriction [9, 10]. Animal studies have demonstrated increased PDE3 protein expression and/or activity following treatment with NO, implicating a role for PDE3 in the poor response to NO [11, 13, 14]. For example, increased PDE3 activity and protein expression were observed in a study of rat pulmonary artery smooth muscle cells (PASMC) exposed to an NO donor [14]. Similarly, pulmonary arteries from one-day-old lambs ventilated with 100% oxygen and iNO had the highest PDE3 activity and the greatest relaxation response to milrinone compared to ventilation with oxygen alone [11]. Interestingly, in the same study PDE3 activity was shown to be significantly higher in one-day-old spontaneously breathing healthy lambs compared to fetal lambs, thus indicating a developmental regulation of PDE3 in the pulmonary vasculature [11]. The higher levels of PDE3 expression after birth could potentially be the reason for the failure of a neonate to sustain a response to iNO following an initial relaxation response when PDE3 levels are low. We recently demonstrated that human neonatal PASMC had increased PDE3A protein expression and increased PDE3 activity, with a concomitant decrease in cAMP levels after treatment with an NO donor [37]. Furthermore, there are several small studies of neonates with PPHN that demonstrate improved oxygenation with the addition of milrinone to iNO in those who were unresponsive to iNO alone [15,16,17, 33, 38]. In a prospective case series, McNamara et al. [17] showed that the addition of milrinone to iNO improved pulmonary arterial pressure and PVR, and increased cardiac output. Consistent with these reports, in our present study iNO non-responders who were treated with milrinone had improved oxygenation, with a significant reduction in the OI at 4, 12, 24, and 48 h after starting milrinone (Fig. 2). Cumulatively, this evidence suggests that milrinone may be of benefit in those who fail to respond to iNO, although further prospective, large-scale studies are needed to confirm these findings. Unfortunately, attempts at large-scale randomized-controlled studies to evaluate the use of milrinone in PPHN have been unsuccessful with early termination due to low enrollment numbers [39].
Interestingly, the group of patients treated with milrinone in the present study were of later GA, higher birth weight, and more often delivered by emergency cesarean section compared to those non-responders who did not receive milrinone. Additionally, the median length of stay was 45 days for the milrinone cohort, which was much longer than that of the non-responders as a whole. It is not clear the reason for these differences given the small sample size, but it may be reflective of a sicker group of patients (Table 2). As shown in Fig. 1D, the non-responders who received milrinone also had a higher overall OI compared to those who did not receive milrinone, although this was not statistically significant in this small sample size. As there was no protocol during the study period in our neonatal intensive care unit to guide the use of milrinone in neonates with HRF, we speculate that it was administered after other measures were exhausted, in an effort to avoid ECMO. If we exclude the patients who required ECMO, the median length of stay was not different between the non-responders who received milrinone and the non-responders who did not receive milrinone (38 vs 30 days, p = 0.28). Furthermore, while eight patients in the non-responder cohort died, no patients who received milrinone died, which may confound length of stay data. Nonetheless, this should be evaluated in future studies. Additionally, the time between starting iNO and adding milrinone was 34 ± 9 h, longer than reported in other studies, which further points to its use as rescue therapy during the study time period. The average dose of milrinone used was 0.36 ± 0.03 mcg/kg/minute, which was lower compared to previous reports (Table 2). During the study period, there was no standard dosing regimen for milrinone in PPHN at our institution. The starting dose of milrinone in this cohort was 0.25–0.35 mcg/kg/minute, with a maximum dose of 0.5 mcg/kg/minute. Follow-up echocardiograms to assess PPHN were not routinely performed after starting milrinone. We speculate that the lack of a bolus and low dose of milrinone used may be related to concerns for the possibility of systemic hypotension related to milrinone administration.
Concerns remain regarding the effects of milrinone on systemic perfusion. It is known that milrinone decreases systemic vascular resistance. Theoretically, a decrease in systemic vascular resistance may result in a greater degree of right-to-left shunting, ultimately worsening hypoxemia. McNamara et al. [16] reported a significant improvement in heart rate and no change in blood pressure or inotropic support after the addition of milrinone in neonates with PPHN. However, in a retrospective study, James et al. [33] reported a significant decrease in the mean blood pressure six hours after initiating a milrinone infusion. Importantly, this reduction in blood pressure was associated with an increase in vasopressor use at six and 12 h after the initiation of milrinone [33]. Although a loading dose was not administered, they used higher overall doses of milrinone (0.5–0.75 mcg/kg/minute), which may account for this difference. In our study, there were no significant changes in heart rate, systolic blood pressure, or the use of dopamine and epinephrine for 48 h after initiation of milrinone (Fig. 2C-F). Conversely, there was a non-significant trend toward lower heart rate and increased systolic blood pressure at the four-hour time point. These findings may be related to a lower dose of milrinone used in our study.
There are several limitations to our study. As a quaternary referral hospital, it is likely that our population of neonates with PPHN represents a sicker group than the general population, as some neonates were transferred for ECMO evaluation after failing iNO at the referring facility. Furthermore, we excluded those neonates who were started on iNO at a referring facility if records were not available for review. During the study period, there was no set protocol for the management of neonates who were iNO non-responsive, which may have resulted in significant practice variability. However, we did record the use of all pulmonary vasodilators, vasopressors, ventilator mode (high-frequency oscillatory ventilation, conventional ventilation), and MAP to assess for these differences. This was a retrospective study and therefore no causal inference can be made. Additionally, given the small sample size, comparisons between groups, specifically amongst the non-responders who did and did not receive milrinone may fail to identify important differences that exist or may find differences that are not true due to significant outliers. It is possible that time alone, or some other factor is responsible for the improvement in oxygenation in iNO non-responders who were administered milrinone. Additionally, as no universally accepted definition of iNO-response exists, we used a definition that we felt was most appropriate and took into account oxygenation and time. However, we accept that it remains unknown as to the best definition for iNO responsiveness, and this may have impacted our results. Finally, additional maternal characteristics such as age, ethnicity, comorbid conditions, and medications may have an impact on iNO response and should be investigated in future studies, along with long-term outcomes.
In conclusion, our present study found that neonates with PPHN who did not respond to iNO had an increased number of ventilator days, a greater length of hospital stay, and an increased risk of death or ECMO than neonates who responded to iNO. Furthermore, the addition of milrinone in iNO non-responders resulted in improvement in oxygenation without impacting systemic hemodynamics. Studies are needed to further characterize iNO responders and non-responders in an effort to decrease the need for ECMO and improve mortality in the non-responders. Specifically, there is a need to identify clinical, biochemical, and genetic factors that may predict iNO responsiveness resulting in more personalized care for neonates with PPHN. Furthermore, it is apparent that large-scale, prospective studies to evaluate the efficacy of milrinone as an adjuvant pulmonary vasodilator in this population, including long-term outcomes, are needed. However, given the lack of success to date in obtaining these data, perhaps future studies should focus on identifying therapies that could be initiated early to improve iNO responsiveness, in addition to identifying rescue therapies for the iNO-unresponsive neonate. A question that remains to be determined is whether milrinone or other pharmacotherapies can be used to enhance the responsiveness to iNO in neonates with PPHN.
References
Nair J, Lakshminrusimha S. Update on PPHN: mechanisms and treatment. Semin Perinatol. 2014;38:78–91.
Lakshminrusimha S, Mathew B, Leach CL. Pharmacologic strategies in neonatal pulmonary hypertension other than nitric oxide. Semin Perinatol. 2016;40:160–73.
Steinhorn RH. Neonatal pulmonary hypertension. Pediatr Crit Care Med. 2010;11:S79–84. 2 Suppl
Clark RH, Huckaby JL, Kueser TJ, Walker MW, Southgate WM, Perez JA, et al. Low-dose nitric oxide therapy for persistent pulmonary hypertension: 1-year follow-up. J Perinatol. 2003;23:300–3.
Inhaled nitric oxide in term and near-term infants: neurodevelopmental follow-up of the neonatal inhaled nitric oxide study group (NINOS). J Pediatr. 2000;136:611–7.
Konduri GG, Vohr B, Robertson C, Sokol GM, Solimano A, Singer J, et al. Early inhaled nitric oxide therapy for term and near-term newborn infants with hypoxic respiratory failure: neurodevelopmental follow-up. J Pediatr. 2007;150:235–40. 40.e1
Group NINOS. Inhaled nitric oxide in full-term and nearly full-term infants with hypoxic respiratory failure. N Engl J Med. 1997;336:597–604.
Clark RH, Kueser TJ, Walker MW, Southgate WM, Huckaby JL, Perez JA, et al. Low-dose nitric oxide therapy for persistent pulmonary hypertension of the newborn. Clinical inhaled nitric oxide research group. N Engl J Med. 2000;342:469–74.
Rose RJ, Liu H, Palmer D, Maurice DH. Cyclic AMP-mediated regulation of vascular smooth muscle cell cyclic AMP phosphodiesterase activity. Br J Pharm. 1997;122:233–40.
Rybalkin SD, Yan C, Bornfeldt KE, Beavo JA. Cyclic GMP phosphodiesterases and regulation of smooth muscle function. Circ Res. 2003;93:280–91.
Chen B, Lakshminrusimha S, Czech L, Groh BS, Gugino SF, Russell JA, et al. Regulation of phosphodiesterase 3 in the pulmonary arteries during the perinatal period in sheep. Pediatr Res. 2009;66:682–7.
Lakshminrusimha S, Porta NF, Farrow KN, Chen B, Gugino SF, Kumar VH, et al. Milrinone enhances relaxation to prostacyclin and iloprost in pulmonary arteries isolated from lambs with persistent pulmonary hypertension of the newborn. Pediatr Crit Care Med. 2009;10:106–12.
Murray F, MacLean MR, Pyne NJ. Increased expression of the cGMP-inhibited cAMP-specific (PDE3) and cGMP binding cGMP-specific (PDE5) phosphodiesterases in models of pulmonary hypertension. Br J Pharm. 2002;137:1187–94.
Busch CJ, Graveline AR, Jiramongkolchai K, Liu H, Sanchez LS, Bloch KD. Phosphodiesterase 3 A expression is modulated by nitric oxide in rat pulmonary artery smooth muscle cells. J Physiol Pharm. 2010;61:663–9.
Bassler D, Choong K, McNamara P, Kirpalani H. Neonatal persistent pulmonary hypertension treated with milrinone: four case reports. Biol Neonate. 2006;89:1–5.
McNamara PJ, Laique F, Muang-In S, Whyte HE. Milrinone improves oxygenation in neonates with severe persistent pulmonary hypertension of the newborn. J Crit Care. 2006;21:217–22.
McNamara PJ, Shivananda SP, Sahni M, Freeman D, Taddio A. Pharmacology of milrinone in neonates with persistent pulmonary hypertension of the newborn and suboptimal response to inhaled nitric oxide. Pediatr Crit Care Med. 2013;14:74–84.
Qasim A, Jain SK. Milrinone Use in Persistent Pulmonary Hypertension of the Newborn. Neoreviews. 2020;21:e165–e78.
Barrington KJ, Finer N, Pennaforte T, Altit G. Nitric oxide for respiratory failure in infants born at or near term. Cochrane Database Syst Rev. 2017;1:CD000399.
Lipkin PH, Davidson D, Spivak L, Straube R, Rhines J, Chang CT. Neurodevelopmental and medical outcomes of persistent pulmonary hypertension in term newborns treated with nitric oxide. J Pediatr. 2002;140:306–10.
Kinsella JP, Truog WE, Walsh WF, Goldberg RN, Bancalari E, Mayock DE, et al. Randomized, multicenter trial of inhaled nitric oxide and high-frequency oscillatory ventilation in severe, persistent pulmonary hypertension of the newborn. J Pediatr. 1997;131:55–62. 1 Pt 1
Roberts JD, Fineman JR, Morin FC, Shaul PW, Rimar S, Schreiber MD, et al. Inhaled nitric oxide and persistent pulmonary hypertension of the newborn. The Inhaled Nitric Oxide Study Group. N Engl J Med. 1997;336:605–10.
Konduri GG, Solimano A, Sokol GM, Singer J, Ehrenkranz RA, Singhal N, et al. A randomized trial of early versus standard inhaled nitric oxide therapy in term and near-term newborn infants with hypoxic respiratory failure. Pediatrics 2004;113:559–64. 3 Pt 1
Field D, Elbourne D, Hardy P, Fenton AC, Ahluwalia J, Halliday HL, et al. Neonatal ventilation with inhaled nitric oxide vs. ventilatory support without inhaled nitric oxide for infants with severe respiratory failure born at or near term: the INNOVO multicentre randomised controlled trial. Neonatology 2007;91:73–82.
Liu CQ, Ma L, Tang LM, He XJ, Wei SF, Wang SX, et al. [A randomized controlled study on the efficacy of inhaled nitric oxide in treatment of neonates with meconium aspiration syndrome]. Zhonghua Er Ke Za Zhi. 2008;46:224–8.
González A, Fabres J, D’Apremont I, Urcelay G, Avaca M, Gandolfi C, et al. Randomized controlled trial of early compared with delayed use of inhaled nitric oxide in newborns with a moderate respiratory failure and pulmonary hypertension. J Perinatol. 2010;30:420–4.
Nelin LD, Potenziano JL. Inhaled nitric oxide for neonates with persistent pulmonary hypertension of the newborn in the CINRGI study: time to treatment response. BMC Pediatr. 2019;19:17.
Kumar D, Super DM, Fajardo RA, Stork EE, Moore JJ, Saker FA. Predicting outcome in neonatal hypoxic respiratory failure with the score for neonatal acute physiology (SNAP) and highest oxygen index (OI) in the first 24 h of admission. J Perinatol. 2004;24:376–81.
Rawat M, Chandrasekharan PK, Williams A, Gugino S, Koenigsknecht C, Swartz D, et al. Oxygen saturation index and severity of hypoxic respiratory failure. Neonatology 2015;107:161–6.
DiBlasi RM, Myers TR, Hess DR. Evidence-based clinical practice guideline: inhaled nitric oxide for neonates with acute hypoxic respiratory failure. Respir Care. 2010;55:1717–45.
Hwang SJ, Lee KH, Hwang JH, Choi CW, Shim JW, Chang YS, et al. Factors affecting the response to inhaled nitric oxide therapy in persistent pulmonary hypertension of the newborn infants. Yonsei Med J. 2004;45:49–55.
Truog WE, Castor CA, Sheffield MJ. Neonatal nitric oxide use: predictors of response and financial implications. J Perinatol. 2003;23:128–32.
James AT, Corcoran JD, McNamara PJ, Franklin O, El-Khuffash AF. The effect of milrinone on right and left ventricular function when used as a rescue therapy for term infants with pulmonary hypertension. Cardiol Young-. 2016;26:90–9.
Goldman AP, Tasker RC, Haworth SG, Sigston PE, Macrae DJ. Four patterns of response to inhaled nitric oxide for persistent pulmonary hypertension of the newborn. Pediatrics 1996;98:706–13. 4 Pt 1
Deb B, Bradford K, Pearl RG. Additive effects of inhaled nitric oxide and intravenous milrinone in experimental pulmonary hypertension. Crit Care Med. 2000;28:795–9.
Dillard J, Perez M, Chen B. Therapies that enhance pulmonary vascular NO-signaling in the neonate. Nitric Oxide. 2020;95:45–54.
Dillard J, Meng X, Nelin L, Liu Y, Chen B. Nitric oxide activates AMPK by modulating PDE3A in human pulmonary artery smooth muscle cells. Physiol Rep. 2020;8:e14559.
El-Khuffash A, McNamara PJ, Breatnach C, Bussmann N, Smith A, Feeney O, et al. The use of milrinone in neonates with persistent pulmonary hypertension of the newborn - a randomised controlled trial pilot study (MINT 1): study protocol and review of literature. Matern Health Neonatol Perinatol. 2018;4:24.
Giaccone A, Zuppa AF, Sood B, Cohen MS, O’Byrne ML, Moorthy G, et al. Milrinone pharmacokinetics and pharmacodynamics in neonates with persistent pulmonary hypertension of the newborn. Am J Perinatol. 2017;34:749–58.
Acknowledgements
We thank Jonathan Slaughter MD, MPH, Nationwide Children’s Hospital, for providing statistical support. This work was supported by the grant 5R01HL13693 (BC) from the National Heart Lung and Blood Institute of the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
JD, LRP, and BC conceived and designed this research; JD, LRP, and SK collected and analyzed data, BC analyzed data, JD drafted the manuscript. All authors edited and revised the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
This study was approved by the local IRB at Nationwide Children’s Hospital, with a risk level of posing no greater than minimal risk.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dillard, J., Pavlek, L.R., Korada, S. et al. Worsened short-term clinical outcomes in a cohort of patients with iNO-unresponsive PPHN: a case for improving iNO responsiveness. J Perinatol 42, 37–44 (2022). https://doi.org/10.1038/s41372-021-01228-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-021-01228-x
