
Abstract
MicroRNAs (MiRNAs) have been found to be dysregulated in lung cancer tissues compared to their matched paracancerous tissues. However, the roles of miRNAs in peripheral blood as potential biomarkers for early diagnosis of lung cancer remain poorly understood. Here we found that miR-33a-5p and miR-128-3p were down-regulated in lung cancer tissues and cell lines. The expression levels of miR-33a-5p and miR-128-3p in lung cancer tissues were significantly correlated to TNM stages. MiR-128-3p in lung cancer tissues was also remarkably related to smoking and tumor size. The relative expression levels of miR-33a-5p and miR-128-3p were positively correlated in lung cancer tissues. Notably, miR-33a-5p and miR-128-3p in whole blood of lung cancer patients or early-stage lung cancer patients (TNM stage I-II) were lowly expressed as compared with that in healthy controls. The receiver operating characteristic curve (ROC) analyses revealed higher area under the ROC curve (AUC) values and higher sensitivity/specificity of miR-33a-5p and miR-128-3p alone and in combination were superior to that of traditional tumor markers (CYFR21-1, NSE and CA72-4). Importantly, both miR-33a-5p and miR-128-3p in whole blood were highly stable even under different harsh conditions. The results demonstrate that tumor suppressor miR-33a-5p/miR-128-3p in whole blood can serve as novel biomarkers for the early detection of lung cancer.
Similar content being viewed by others

Introduction
Lung cancer can be divided into non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC) according to different pathological types, and NSCLC accounts for 80–85% of all lung cancers1. Although the current diagnosis and treatment for lung cancer have made great progress in past decades, the mortality rate in lung and bronchus cancers is 26% and 25%, respectively, and the 5-year survival rate of lung cancer is only 5%2. Therefore, early diagnosis for lung cancer is particularly important.
MicroRNAs (miRNAs) are small, conserved, non-coding RNA molecules of approximately 19-25 nucleotides in size that bind to the 3′-untranslated region of a target mRNA resulting in mRNA degradation and/or translation repression3,4. Studies have reported that miRNAs can be involved in lung cancer cell proliferation, migration, invasion and drug resistance5,6,7,8,9. The miRNAs present in the blood are usually called circulating miRNAs10. Circulating miRNAs can be stably present in the blood in the form of Ago2-miRNA protein complexes to protect against RNase degradation and multiple freeze-thaw cycles11. Therefore, the differentially expressed circulating miRNAs in lung cancer patients and healthy humans can be used as novel biomarkers for diagnosis of lung cancer12. MiR-33a-5p is an intronic miRNA located in intronic sequences of the sterol-response-element-binding protein gene 2 (SREBP2), it has been reported that miR-33a-5p acts as a tumor suppressor and inhibits cancer cell proliferation and aggressiveness in lung cancer13,14,15. In addition, miR-128 is significantly down-regulated in NSCLC tissues and cancer cells, in vivo restoration of miR-128 significantly suppresses tumourigenicity of A549 cells in nude mice and inhibits both angiogenesis and lymphangiogenesis of tumor xenografts16. Importantly, antagonism of miR-128-3p potently reverses metastasis and chemoresistance of highly malignant NSCLC cells, which could be completely reversed by restoring Wnt/β-catenin and TGF-β activities, suggesting that miR-128-3p might be a potential target against both metastasis and chemoresistance in NSCLC17.
In our previous studies, we have found that two miRNAs (miR-33a-5p and miR-128-3p) are down-regulated in lung cancer tissues compared to paired normal tissues18,19. However, the clinical significance of these two miRNAs in early diagnosis of lung cancer remains unclear. Compared with tissue samples, blood specimens are easier to collect and miRNA in whole blood can serve as a new type of non-invasive biomarker in the diagnosis of lung cancer. In present study, we detected the expression levels of miR-33a-5p and miR-128-3p in whole blood samples to evaluate the values of these two miRNAs as biomarkers for early diagnosis of lung cancer.
Results
MiR-33a-5p and miR-128-3p were significantly down-regulated in lung cancer tissues and lung cancer cell lines
To confirm the expression levels of miR-33a-5p and miR-128-3p in lung cancer patients, we detected their expression levels in 65 lung cancer tissues and the paired normal adjacent tissues using qRT-PCR. As was expected, the melting curve showed that the amplified product of miR-33a-5p/miR-128-3p generated a single peak (Fig. S1A,B). The qRT-PCR results showed that miR-33a-5p and miR-128-3p were significantly down-regulated in lung cancer tissues compared to adjacent normal tissues (P < 0.001, Fig. 1A,B). Notably, in each pair of cancer and adjacent normal tissue, the fold change of miR-33a-5p was 0.001~0.46 (Fig. 1C), while the fold change of miR-128-3p was 0.001~0.67 (Fig. 1D). Interestingly, the relative expression levels of miR-33a-5p and miR-128-3p were positively correlated in lung cancer tissues (P < 0.001, Fig. 1E). In addition, we further validated the expression levels of miR-33a-5p and miR-128-3p in lung cancer cell lines. Compared with human normal lung epithelial cells (BEAS-2B), both miR-33a-5p of and miR-128-3p were lowly expressed in lung cancer cell lines (NCI-H1299, A549, SPC-A-1 and LTEP-a-2) (P < 0.05, Fig. 1F,G). Together, these two tumor suppressor miRNAs were remarkably down-regulated in lung cancer.

Both miR-33a-5p and miR-128-3p were down-regulated in lung cancer tissues and lung cancer cell lines. MiR-33a-5p (A) and miR-128-3p (B) showed a statistically down-regulated expression in each lung cancer tissues and the matched adjacent normal tissues (n = 65, P < 0.001). The relative expression of miR-33a-5p (C) and miR-128-3p (D) in 65 paired lung cancer tissues and matched adjacent normal tissues. Results were presented as the fold-change in tumor tissues compared to adjacent normal tissues. (E) Pearson correlation coefficient showed that the relative expressions of miR-33a-5p and miR-128-3p were significantly positively correlated in lung cancer tissues (P = 0.0008). Compared with normal lung epithelial cell (BEAS-2B), the relative expressions of miR-33a-5p (F) and miR-128-3p (G) were significantly lower in four lung cancer cell lines (NCI-H1299, A549, SPC-A-1, and LTEP-a-2, P < 0.05). *P < 0.05, **P < 0.01, ***P < 0.001.
MiR-33a-5p was closely correlated to TNM stage, while miR-128-3p was strongly related to smoking, tumor size and TNM stage in lung cancer patients
To investigate the relationship between miR-33a-5p/miR-128-3p expression levels and clinicopathological factors in lung cancer patients, we collected and analyzed the clinical data of 65 proven cases. Based on the constitutive expression levels of miR-33a-5p/miR-128-3p, 65 cases were divided into high expression group (n = 33) and low expression group (n = 32) by the median. We did not find a significant association of miR-33a-5p expression with patients’ sex (P = 0.6942), age (P = 0.3781), smoking (P = 0.2669), pathology classification (P = 0.8191), tumor location (P = 0.8753), differentiated degree (P = 0.5902) and tumor size (P = 0.8208). However, the expression of miR-33a-5p was significantly correlated with tumor node metastasis (TNM) stage (P = 0.0133) (Table 1). Similarly, we also found there was no significant association of miR-128-3p expression with patients’ sex (P = 0.7083), age (P = 0.3843), pathology classification (P = 0.1535), tumor location (P = 0.6854) and differentiated degree (P = 0.11) (Table 2). Whereas miR-128-3p expression was strongly related to tumor size (P = 0.0025) and TNM stage (P = 0.0076). Interestingly, miR-128-3p was also found to be correlated with smoking (P = 0.0178) (Table 2). In general, the expression of miR-33a-5p/miR-128-3p were closely correlated with tumor growth in the early stage.
MiR-33a-5p and miR-128-3p had higher diagnostic value in lung cancer tissues
We further evaluated the diagnostic value of miR-33a-5p and miR-128-3p in lung cancer tissues and corresponding adjacent normal tissues by constructing ROC curves. The ROC analysis showed that the AUC of miR-33a-5p was 0.8644 (95% confidence interval (CI) = 0.8016 to 0.9271, sensitivity = 84.62% and specificity = 76.92%, Fig. 2A,D), and the AUC of miR-128-3p was 0.9391 (95% CI = 0.9022 to 0.9759, sensitivity = 73.85% and specificity = 98.46%, Fig. 2B,D). Moreover, the combination of miR-33a-5p and miR-128-3p yielded a higher AUC value at 0.9517 (95% CI = 0.9199 to 0.9835, sensitivity = 92.31% and specificity = 83.08%, Fig. 2C,D). The results indicated that both miR-33a-5p and miR-128-3p has individual diagnostic value and the combined diagnostic value of these two miRNAs is much higher than that of any single miRNA.

Diagnostic value of miR-33a-5p and miR-128-3p in lung cancer tissues. The ROC analysis for detection of lung cancer tissues and corresponding adjacent normal tissues using miR-33a-5p (A), miR-128-3p (B), and miR-33a-5p + miR-128-3p (C). (D) The comparison of diagnostic values between miR-33a-5p, miR-128-3p and the combination.
MiR-33a-5p and miR-128-3p were lowly expressed in whole blood and served as minimally invasive biomarker to diagnose lung cancer
To reveal the clinical value of these two miRNAs in non-invasive diagnosis for lung cancer, we analyzed the circulating miR-33a-5p/miR-128-3p in whole blood from 90 patients with lung cancer and 90 healthy controls. The qRT-PCR results showed that miR-33a-5p and miR-128-3p expression levels were significantly down-regulated in whole blood from lung cancer patients compared with that from in healthy controls (P < 0.001, Fig. 3A,C). We further evaluated the diagnostic values of miR-33a-5p and miR-128-3p in whole blood with lung cancer and healthy controls. The corresponding AUC value of miR-33a-5p was 0.870 (95% CI = 0.7786 to 0.9614, sensitivity = 86.67% and specificity = 73.33%, Fig. 3B), and the AUC value of miR-128-3p was 0.9278 (95% CI = 0.8616 to 0.9939, sensitivity = 93.33% and specificity = 80%, Fig. 3D). Correspondingly, we used miR-33a-5p and miR-128-3p to create a combined diagnostic model using logistic regression models. The combined diagnostic model showed the AUC of combined two circulating miRNAs was up to 0.9511 (95% CI = 0.8904 to 1.012, sensitivity = 96.67% and specificity = 83.33%, Fig. 3E). These findings indicated that the circulating miR-33a-5p/miR-128-3p were lowly expressed in whole blood of lung cancer patients and had the greater diagnostic value for diagnosis of lung cancer.

Both miR-33a-5p and miR-128-3p were lower expressed in whole blood with lung cancer and had greater diagnostic value. MiR-33a-5p (A) and miR-128-3p (C) were down-regulated in whole blood from lung cancer patients compared to that from healthy controls (n = 90, P < 0.001). The ROC analysis for detection of lung cancer patients from health controls using miR-33a-5p (B), miR-128-3p (D), and miR-33a-5p + miR-128-3p (E). ***P < 0.001.
Whole blood miR-33a-5p and miR-128-3p could be used to distinguish early-stage lung cancer patients from healthy controls
To further verify the diagnostic value of miR-33a-5p and miR-128-3p in early-stage lung cancer, we detected the relative expression of miR-33a-5p in 41 patients with lung cancer at early stage (TNM stage I-II) and 41 healthy controls, and miR-128-3p in 42 patients with lung cancer at early stage (TNM stage I–II) and 42 healthy controls. The results showed that the expression levels of circulating miR-33a-5p and miR-128-3p in healthy controls were significantly higher than that in early-stage lung cancer patients (P < 0.001, Fig. 4A,C). The AUC values of miR-33a-5p and miR-128-3p were 0.8456 (95% confidence interval (CI) = 0.7586 to 0.9327, sensitivity = 85.37% and specificity = 75.61%, Fig. 4B,F) and 0.9246, respectively (95% CI = 0.8677 to 0.9815, sensitivity = 90.48% and specificity = 85.71%, Fig. 4D,F). Interestingly, the combined two-miRNA signature yielded higher values of AUC and specificity (AUC = 0.9554; 95% CI = 0.9144 to 0.9964, sensitivity = 90.24% and specificity = 92.68%, Fig. 4E,F). These results indicated that miR-33a-5p, miR-128-3p, and a two-miRNA signature could be used as novel biomarkers for early diagnosis of lung cancer.

MiR-33a-5p and miR-128-3p could be used to distinguish early-stage lung cancer patients from healthy controls. MiR-33a-5p (A) and miR-128-3p (C) were down-regulated in early lung cancer patients (TNM stage I-II) compared to healthy controls (P < 0.001). The ROC analysis for detection of early lung cancer patients from health controls using miR-33a-5p (B), miR-128-3p (D), and miR-33a-5p + miR-128-3p (E). (F) The comparison of diagnostic values between miR-33a-5p, miR-128-3p and the combination. ***P < 0.001.
MiR-33a-5p and miR-128-3p had higher diagnostic value than traditional tumor markers for lung cancer
We compared the diagnostic values of miR-33a-5p, miR-128-3p and their combination with three commonly used tumor markers (cytokeratin-19-fragment (CYFR21-1), neuron-specific enolase (NSE) and cancer antigen 72-4 (CA72-4)), and obtained the following AUC values: CYFR21-1, 0.5856 (95% CI = 0.4387 to 0.7324, sensitivity = 63.33% and specificity = 63.33%, Fig. 5A,D), NSE, 0.6189 (95% CI = 0.4748 to 0.763, sensitivity = 73.33% and specificity = 56.67%, Fig. 5B,D), CA72-4, 0.5206 (95% CI = 0.3684 to 0.6727, sensitivity = 86.67% and specificity = 36.67%, Fig. 5C,D). In summary, the results showed that the diagnostic values of miR-33a-5p and miR-128-3p were superior to three traditional tumor markers, and the AUC value of the combined diagnosis was not only higher than that of the individual miRNA, but also higher than that of any single traditional biomarker (Fig. 5D), suggesting the highest diagnostic performance.

Diagnostic performance of miR-33a-5p/miR-128-3p and three traditional tumor markers for detection of lung cancer. The ROC analysis for detection of lung cancer using traditional tumor markers CYFR21-1 (A), NSE (B) and CA72-4 (C). (D) The comparison of diagnosis values between miR-33a-5p/miR-128-3p and the combination and three traditional tumor markers.
MiR-33a-5p and miR-128-3p were stably expressed in whole blood under harsh conditions
To test the stability of miR-33a-5p and miR-128-3p in whole blood of lung cancer patients, we collected fresh whole blood from 12 patients with lung cancer, and divided into 3 groups (4 in each group). The first group was incubated at room temperature for different times (0, 2, 6, 12, 24 h), the second group was repeated for different freeze-thaw cycles (0, 2, 4, 6, 8 cyles), and the third group was treated with RNase A digestion for different times (0, 30, 60 min). The results of qRT-PCR showed that the relative expression levels of miR-33a-5p and miR-128-3p did not significantly change under the different incubation time at room temperature (Fig. 6A). Similarly, no significant difference of the miRNA expression was found between 0 to 8 cycles of freeze-thaw treatment (Fig. 6B). Likewise, the RNase A treatment for different time did not markedly affect the raw Ct values of the two circulating miRNAs (Fig. 6C). These results indicated that both miR-33a-5p and miR-128-3p was stably expressed in whole blood under harsh conditions. Therefore, the stability of these two circulating miRNAs in whole blood demonstrates the potential of being diagnostic biomarkers for lung cancer.

Stability test for miR-33a-5p and miR-168-3p. The fresh whole blood samples from 12 patients with lung cancer were exposed to different harsh conditions: incubating at room temperature for 0, 2, 6, 12, 24 h (A), treating with 0, 2, 4, 6, 8 repetitive freeze-thaw cycles (B) and RNase A digestion for 0, 30, 60 min at 37 °C (C). No significant difference was observed in each group. P > 0.05.
Discussion
In our previous studies, we found that miR-33a-5p inhibits NSCLC epithelial-mesenchymal transition (EMT) and serves as a prognostic factor for NSCLC18. Furthermore, we discovered that miR-128-3p directly targets PFK liver type (PFKL) in lung cancer cells and regulates endogenous expression of PFKL at both mRNA and protein levels. Knockdown of miR-128 has been shown to promote lung cancer cell growth and colony formation19. However, the correlation between miR-33a-5p/miR-128-3p and the pathological features of lung cancer patients is still not well known. In current study, we revealed the clinical values of miR-33a-5p and miR-128-3p in peripheral blood for early diagnosis of lung cancer.
In existing studies, miR-33a was found to be decreased in NSCLC tissues compared with the para-carcinoma tissues. Also, miR-33a could inhibit lung cancer cell proliferation, cell cycle progression, and migration by targeting cullin-associated NEDD8-dissociated protein 120. Compared to adjacent non-tumor tissues, miR-128 was down-regulated in lung cancer tissues and miR-128 induced apoptosis in lung cancer cell lines21. These results are consistent with our findings, that miR-33a-5p and miR-128-3p were lowly expressed in lung cancer tissues and lung cancer cell lines. In addition, miR-33a-5p and miR-128-3p exhibited lower expression in colorectal cancer22, osteosarcoma23, breast cancer24 and pancreas cancer25, suggesting that miR-33a-5p and miR-128-3p might act as tumor suppressors in the progression of cancer and have the potential diagnostic value in cancer.
It is particularly important to improve the early diagnosis and early treatment of patients with lung cancer. MiRNAs have been proven to be targets in cancer therapy and to be biomarkers in cancer diagnosis11,26,27. For lung cancer, the hairpin probe-based rolling circle amplification (HP-RCA) technique was developed to directly and accurately distinguish the expression of serum miR-486-5p in NSCLC patients from healthy persons, holding a great potential for further applications in the clinical diagnosis of lung cancers28. Moreover, miRNA-30a was significantly elevated in plasma of NSCLC patients. ROC curve analysis showed that the cut-off points of specificity and sensitivity of NSCLC were 61.0% and 84.3%, respectively29. Generally, targeted therapy for NSCLC requires more accurate tumor classification. It was found that hsa-miR-205 and hsa-miR-21 expressions were appropriate measures allowing a sufficiently accurate discrimination between lung adenocarcinoma (AC) and squamous cell lung carcinoma (SCC) histotype if they were normalized by U6 snRNA and hsa-miR-10330. Other circulating miRNAs could also be used as biomarkers for the diagnosis of colorectal cancer31,32, chronic cardiovascular diseases33 and pulmonary tuberculosis34. In present study, we aimed to verify the expression of miR-33a-5p and miR-128-3p in whole blood and found that the expression levels of miR-33a-5p and miR-128-3p in whole blood of lung cancer patients were significantly lower than those of healthy controls. Compared with plasma and serum, it is more convenient to get whole blood from patients. Also, the stability and abundance of RNA in whole blood is much better than that in plasma or serum. The advantages of minimally invasive and real-time detection of whole blood bring great convenience to clinical diagnosis.
Studies have shown that combined biomarkers can improve the diagnostic accuracy of cancer35,36,37. In the results, the diagnostic values of miR-33a-5p and miR-128-3p in whole blood of lung cancer patients and that of healthy controls showed that the AUC of miR-33a-5p was 0.870, the AUC of miR-128-3p was 0.9278, and the combined AUC of miR-33a-5p and miR-128-3p was 0.951, suggesting a higher combined diagnostic value of miR-33a-5p and miR-128-3p. In addition, the combined sensitivity and specificity of miR-33a-5p and miR-128-3p are better than that of miR-33a-5p and miR-128-3p alone. Compared with a three-miRNA signature (miR-125a-5p, miR-25, and miR-126) as a combined diagnosis of lung cancer12, the values of AUC and sensitivity of the combined diagnosis of our two miRNAs (miR-33a-5p and miR-128-3p) are much higher (AUC, 0.951 vs. 0.936; sensitivity, 96.70% vs. 87.50%), but the combined specificity is slightly lower (83.30% vs. 87.5%). We also compared the diagnostic values of miR-33a-5p and miR-128-3p with traditional diagnostic tumor markers, and found that the diagnostic value of miR-33a-5p and miR-128-3p was higher than that of traditional tumor markers. We analyzed the relationship between the expression of miR-33a-5p and miR-128-3p in lung cancer tissues and clinicopathological factors found that both miR-33a-5p and miR-128-3p were related to TNM staging, and miR-128-3p is also related to smoking and tumor size, suggesting certain mechanism in the future research. Notably, the stability of miR-33a-5p and miR-128-3p in whole blood demonstrates an advantage as a joint biomarker for early diagnosis of lung cancer. Since miR-33a-5p and miR-128-3p are stable in whole blood under different harsh conditions, it is speculated that these two miRNAs may be secreted in exosomes, which requires us to verify in future work. Because the cargo of the exosomes are specific to the parental cells and the conditions in which they are produced, suggesting that circulating miRNAs in the exosomes are likely to be prognostic and predictive biomarkers38,39. As diagnostic tumor markers, higher expressions of plasma exosomal miR-1290 and miR-375 were significantly associated with poor overall survival for castration-resistant prostate cancer (CPRC) patients40. Additionally, circulating exosomal miR-425-3p in NSCLC patients could serve as a biomarker for predicating the clinical responses to platinum-based chemotherapy41.
To clarify the diagnostic values of miR-33a-5p and miR-128-3p in lung cancer, we should also expand the sample number to verify its value in future study. To avoid false positive rate, we should also distinguish the blood miR-33a-5p and miR-128-3p in other benign lung diseases (such as pneumonia, tuberculosis, etc) and their expressions in lung cancer. In addition, we tested serum samples from 27 lung cancer patients who received chemoradiotherapy and found that the expression levels of miR-33a-5p and miR-128-3p from lung cancer patients receiving chemoradiotherapy were much higher than that of whole blood with lung cancer, and was lower than that of healthy serum controls (data not shown). We speculate that miR-33a-5p and miR-128-3p are also related to radiotherapy and chemotherapy, suggesting that a detailed investigation is needed.
In summary, both miR-33a-5p and miR-128-3p has the advantage for diagnosing lung cancer at early stage, and the combined diagnosis value of miR-33a-5p and miR-128-3p is much higher. In addition, the diagnostic values of miR-33a-5p and miR-128-3p are superior to traditional tumor markers. More importantly, the expression of miR-33a-5p and miR-128-3p in whole blood is very stable under different harsh conditions, indicating that the two-miRNA signature (miR-33a-5p and miR-128-3p0 has the potential to serve as novel biomarker to distinguish early-stage lung cancer from healthy controls.
Methods
Clinical specimens
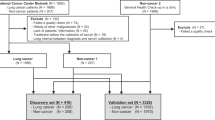
Clinical samples of lung cancer tissues and paired normal tissues were collected from the Affiliated Hospital of Medical School of Ningbo University (Ningbo, China) and Ningbo Medical Center Lihuili Eastern Hospital (Ningbo, China), and the whole blood samples were obtained from the Affiliated Hospital of Medical School of Ningbo University (Ningbo, China) between September 2014 and December 2017. A total of 65 patients with primary lung cancer and their corresponding normal tissues were resected from the operation before treatment. And the adjacent normal tissues were at least 5 cm away from lung cancer tissues. All tissues specimens were placed immediately after resection in the RNAstore (CWBIO, Beijing, China), then stored at −80 °C until use. Peripheral whole blood of 90 patients with lung cancer and 90 healthy controls were obtained using ethylenediaminetetraacetic acid (EDTA) tubes before surgery. Whole blood samples were placed at −80 °C. All specimens were confirmed to be lung cancer according to the International Cancer Control Alliance Version 8 lung cancer standard system. Written informed consent was obtained from all patients and the study protocol was approved by the Clinical Research Ethics Committee of Medical School of Ningbo University. All experiments were performed in accordance with relevant guidelines and regulations.
RNA extraction
Total RNA including miRNA, was isolated from tissue samples using TRIzol reagent (Invitrogen, Carlsbad, CA, USA) according to the manufacturer’s instructions. Total RNA containing miRNA in whole blood was extracted by TRIpure LS Reagent (BioTeKe, Beijing, China). First, added 750 ul of TRIpure LS Reagent to the whole blood of 250 μl of lung cancer patients, mixd by vortexing and placed on ice for 10 min. Thereafter, 200 ul of chloroform was added, mixed by vortexing and placed on ice for 3 min. Subsequently, it was centrifuged at a speed of 12,000 g for 15 min. After centrifugation, the supernatant was pipetted into a clean RNase-free eppendorf (EP) tube, 500 ul of isopropanol was added, gently mixed upside down and placed on ice for 10 min. Then, it was centrifuged at a speed of 12,000 g for 10 min. The liquid in the EP tube was poured out, and 1 ml of 75% ethanol in Diethy pyrocarbonate (DEPC) water was added, and the mixture was centrifuged at 8000 g for 5 min, and the operation was repeated once. Finally, the liquid in the EP tube was poured out, the EP tube was placed in air dry, and then the RNA was dissolved with an appropriate amount of DEPC water. Subsequently, the concentration and purity of RNA were measured by DeNovix DS-11 Spectrophotometer (DeNovix, DE, USA).
Reverse transcription
Using the Hairpin-itTM miR qPCR quantification kit (GenePharma, China). Each reverse transcription was carried out in a volume of 20 μl containing 4 μl 5 × MMLV RT Buffer, 0.75 μl dNTP (10 mM), 1.2 μl miRNA&U6 snRNA RT primer mix (1 μM), 0.25 μl RNasin (40U/μl), 0.2 μl MMLV Reverse Transcriptase, 1 μg total RNA). The reaction mixture was incubated at 25 °C for 30 min, 42 °C for 30 min and 85 °C for 5 min on a Thermal Cycler (MJ research, USA).
Quantitative real-time PCR
To quantitate miR-33a-5p and miR-128-3p levels, the Hairpin-itTM miR qPCR quantification kit (GenePharma, China) was used for the quantitative real-time polymerase chain reaction (qRT-PCR), and the qRT-PCR reaction was carried out on a Mx3005P real-time PCR System (Stratagene, CA, USA). The qRT-PCR reaction volume is 20 μl, including 10 μl of 2 × Real-time PCR Buffer 1, 0.4 μl of miRNA specific primers (0.1 μM), 2 μl of miRNA RT product, 0.2 μl of Taq DNA polymerase (5U/μl) and 7.4 μl of double distilled water. The reaction was performed in an eight-strip (Axygen, USA) tube under the following conditions: 95 °C for 3 min, 40 cycles of 95 °C for 12 s, 62 °C for 40 s. The small nuclear RNA U6 was used to normalize the expression of miR-33a-5p and miR-128-3p. The relative expression levels of miR-33a-5p and miR-128-3p were calculated using the 2−∆CT method All qRT-PCR reactions were performed in triplicate.
Cell culture
Four lung cancer cell lines (NCI-H1299, A549, SPC-A-1, LTEP-a-2), and the human normal lung epithelial cell line (BEAS-2B) were purchased from Chinese Academy of Sciences Cell Bank of Type Culture Collection (Shanghai, China). NCI-H1299, A549, SPC-A-1 and LTEP-a-2 cell lines were cultured in RPMI-1640 (Gibco, USA) medium supplemented with 10% fetal bovine serum (PAN-Biotech, Aidenbach, Germany) with 1% penicillin/streptomycin (Life Technologies, CA, USA). BEAS-2B was cultured in Dulbecco’s modified Eagle’s medium (DMEM) high glucose (HyClone, CT, USA), containing 10% fetal bovine serum only. All of these cells were maintained in 5% CO2 at 37 °C.
Statistical analysis
All data were analyzed by using Statistical Product and Service Solutions software 23.0 (Statistical Product and Service Solutions, IL, USA) and GraphPad Prism 7.0 (GraphPad Software, CA, USA). The Wilcoxon matched-pairs signed rank test was used to compare the expression levels of miR-33a-5p and miR-128-3p between lung tumor tissues and paired adjacent normal tissues. The Student’s t-test was performed to compare the different expression levels of miR-33a-5p and miR-128-3p between lung cancer cell lines and human normal lung epithelial cell line. The Nonparametric Mann-Whitney U test was employed to compare the expression levels of miR-33a-5p and miR-128-3p in whole blood between lung cancer patients and healthy person. The Chi squared test was used to analyze the associations between the expression level of miR-33a-5p and miR-128-3p and the clinicopathological factors. The diagnostic value of miR-33a-5p and miR-128-3p were conducted by the ROC and the AUC. The optimal cut-off thresholds were determined by using the highest Youden index. For correlation, Pearson’s correlations were used. For all analyses, differences were considered statistically significant at P-value less than 0.05.
References
Wood, D. E. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines for Lung Cancer Screening. Thoracic surgery clinics 25, 185–197, https://doi.org/10.1016/j.thorsurg.2014.12.003 (2015).
Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, 2018. CA Cancer J Clin 68, 7–30, https://doi.org/10.3322/caac.21442 (2018).
Bartel, D. P. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell 116, 281–297 (2004).
Lagos-Quintana, M., Rauhut, R., Lendeckel, W. & Tuschl, T. Identification of novel genes coding for small expressed RNAs. Science (New York, N.Y.) 294, 853–858, https://doi.org/10.1126/science.1064921 (2001).
Yoo, J. K. et al. The novel miR-9500 regulates the proliferation and migration of human lung cancer cells by targeting Akt1. Cell death and differentiation 21, 1150–1159, https://doi.org/10.1038/cdd.2014.33 (2014).
Xue, X. et al. miR-342-3p suppresses cell proliferation and migration by targeting AGR2 in non-small cell lung cancer. Cancer letters 412, 170–178, https://doi.org/10.1016/j.canlet.2017.10.024 (2018).
Wei, C. H. et al. MicroRNA-330-3p promotes cell invasion and metastasis in non-small cell lung cancer through GRIA3 by activating MAPK/ERK signaling pathway. Journal of hematology & oncology 10, 125, https://doi.org/10.1186/s13045-017-0493-0 (2017).
Shi, Z. M. et al. Downregulation of miR-218 contributes to epithelial-mesenchymal transition and tumor metastasis in lung cancer by targeting Slug/ZEB2 signaling. Oncogene 36, 2577–2588, https://doi.org/10.1038/onc.2016.414 (2017).
MacDonagh, L. et al. The emerging role of microRNAs in resistance to lung cancer treatments. Cancer treatment reviews 41, 160–169, https://doi.org/10.1016/j.ctrv.2014.12.009 (2015).
Montani, F. et al. miR-Test: a blood test for lung cancer early detection. Journal of the National Cancer Institute 107, djv063, https://doi.org/10.1093/jnci/djv063 (2015).
Mitchell, P. S. et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proceedings of the National Academy of Sciences of the United States of America 105, 10513–10518, https://doi.org/10.1073/pnas.0804549105 (2008).
Wang, P. et al. Early Detection of Lung Cancer in Serum by a Panel of MicroRNA Biomarkers. Clinical lung cancer 16, 313–319.e311, https://doi.org/10.1016/j.cllc.2014.12.006 (2015).
Marquart, T. J., Allen, R. M., Ory, D. S. & Baldan, A. miR-33 links SREBP-2 induction to repression of sterol transporters. Proceedings of the National Academy of Sciences of the United States of America 107, 12228–12232, https://doi.org/10.1073/pnas.1005191107 (2010).
Kang, J. et al. TFAP2C promotes lung tumorigenesis and aggressiveness through miR-183- and miR-33a-mediated cell cycle regulation. Oncogene 36, 1585–1596, https://doi.org/10.1038/onc.2016.328 (2017).
Du, M. et al. MiR-33a suppresses proliferation of NSCLC cells via targeting METTL3 mRNA. Biochemical and biophysical research communications 482, 582–589, https://doi.org/10.1016/j.bbrc.2016.11.077 (2017).
Hu, J. et al. microRNA-128 plays a critical role in human non-small cell lung cancer tumourigenesis, angiogenesis and lymphangiogenesis by directly targeting vascular endothelial growth factor-C. European journal of cancer (Oxford, England: 1990) 50, 2336–2350, https://doi.org/10.1016/j.ejca.2014.06.005 (2014).
Cai, J. et al. Simultaneous overactivation of Wnt/beta-catenin and TGFbeta signalling by miR-128-3p confers chemoresistance-associated metastasis in NSCLC. Nature communications 8, 15870, https://doi.org/10.1038/ncomms15870 (2017).
Yang, L. et al. MircoRNA-33a inhibits epithelial-to-mesenchymal transition and metastasis and could be a prognostic marker in non-small cell lung cancer. Scientific reports 5, 13677, https://doi.org/10.1038/srep13677 (2015).
Yang, J. et al. PFKL/miR-128 axis regulates glycolysis by inhibiting AKT phosphorylation and predicts poor survival in lung cancer. American journal of cancer research 6, 473–485 (2016).
Kang, M., Li, Y., Zhao, Y., He, S. & Shi, J. miR-33a inhibits cell proliferation and invasion by targeting CAND1 in lung cancer. Clinical & translational oncology: official publication of the Federation of Spanish Oncology Societies and of the National Cancer Institute of Mexico 20, 457–466, https://doi.org/10.1007/s12094-017-1730-2 (2018).
Zhao, D., Han, W., Liu, X., Cui, D. & Chen, Y. MicroRNA-128 promotes apoptosis in lung cancer by directly targeting NIMA-related kinase 2. Thoracic cancer 8, 304–311, https://doi.org/10.1111/1759-7714.12442 (2017).
Shan, Y. et al. MicroRNA-33a and let-7e inhibit human colorectal cancer progression by targeting ST8SIA1. The international journal of biochemistry & cell biology 90, 48–58, https://doi.org/10.1016/j.biocel.2017.07.016 (2017).
Jiang, N. et al. lncRNA DANCR promotes tumor progression and cancer stemness features in osteosarcoma by upregulating AXL via miR-33a-5p inhibition. Cancer letters 405, 46–55, https://doi.org/10.1016/j.canlet.2017.06.009 (2017).
Eterno, V. et al. AurkA controls self-renewal of breast cancer-initiating cells promoting wnt3a stabilization through suppression of miR-128. Scientific reports 6, 28436, https://doi.org/10.1038/srep28436 (2016).
Han, H., Wang, L., Xu, J. & Wang, A. miR-128 induces pancreas cancer cell apoptosis by targeting MDM4. Experimental and therapeutic medicine 15, 5017–5022, https://doi.org/10.3892/etm.2018.6047 (2018).
Di Lisio, L. et al. The role of miRNAs in the pathogenesis and diagnosis of B-cell lymphomas. Blood 120, 1782–1790, https://doi.org/10.1182/blood-2012-05-402784 (2012).
Dieckmann, K. P. et al. Serum Levels of MicroRNA miR-371a-3p: A Sensitive and Specific New Biomarker for Germ Cell Tumours. European urology 71, 213–220, https://doi.org/10.1016/j.eururo.2016.07.029 (2017).
Li, Y., Liang, L. & Zhang, C. Y. Isothermally sensitive detection of serum circulating miRNAs for lung cancer diagnosis. Analytical chemistry 85, 11174–11179, https://doi.org/10.1021/ac403462f (2013).
Sun, L. et al. Increased Plasma miRNA-30a as a Biomarker for Non-Small Cell Lung Cancer. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research 22, 647–655 (2016).
Charkiewicz, R. et al. Validation for histology-driven diagnosis in non-small cell lung cancer using hsa-miR-205 and hsa-miR-21 expression by two different normalization strategies. International journal of cancer 138, 689–697, https://doi.org/10.1002/ijc.29816 (2016).
Nonaka, R. et al. Circulating miR-199a-3p as a novel serum biomarker for colorectal cancer. Oncology reports 32, 2354–2358, https://doi.org/10.3892/or.2014.3515 (2014).
Imaoka, H. et al. Circulating microRNA-1290 as a novel diagnostic and prognostic biomarker in human colorectal cancer. Annals of oncology: official journal of the European Society for Medical Oncology 27, 1879–1886, https://doi.org/10.1093/annonc/mdw279 (2016).
Jiang, Y. et al. Peripheral blood miRNAs as a biomarker for chronic cardiovascular diseases. Scientific reports 4, 5026, https://doi.org/10.1038/srep05026 (2014).
Zheng, M. L., Zhou, N. K. & Luo, C. H. MiRNA-155 and miRNA-132 as potential diagnostic biomarkers for pulmonary tuberculosis: A preliminary study. Microbial pathogenesis 100, 78–83, https://doi.org/10.1016/j.micpath.2016.09.005 (2016).
Sun, L. et al. Three-dimensional combined biomarkers assay could improve diagnostic accuracy for gastric cancer. Scientific reports 7, 11621, https://doi.org/10.1038/s41598-017-12022-1 (2017).
Zhang, J. et al. Circulating MiR-16-5p and MiR-19b-3p as Two Novel Potential Biomarkers to Indicate Progression of Gastric Cancer. Theranostics 5, 733–745, https://doi.org/10.7150/thno.10305 (2015).
Zhou, C. et al. Combination of serum miRNAs with Cyfra21-1 for the diagnosis of non-small cell lung cancer. Cancer letters 367, 138–146, https://doi.org/10.1016/j.canlet.2015.07.015 (2015).
Schwarzenbach, H. Clinical Relevance of Circulating, Cell-Free and Exosomal microRNAs in Plasma and Serum of Breast Cancer Patients. Oncology research and treatment 40, 423–429, https://doi.org/10.1159/000478019 (2017).
Sun, Z. et al. Effect of exosomal miRNA on cancer biology and clinical applications. Molecular cancer 17, 147, https://doi.org/10.1186/s12943-018-0897-7 (2018).
Huang, X. et al. Exosomal miR-1290 and miR-375 as prognostic markers in castration-resistant prostate cancer. European urology 67, 33–41, https://doi.org/10.1016/j.eururo.2014.07.035 (2015).
Yuwen, D. et al. Prognostic role of circulating exosomal miR-425-3p for the response of NSCLC to platinum-based chemotherapy. Cancer epidemiology, biomarkers & prevention: a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology, https://doi.org/10.1158/1055-9965.epi-18-0569 (2018).
Acknowledgements
This work was supported in part by research grants from the Non-profit Technology Research Program of Zhejiang (LGF18H160006), the Natural Science Foundation of Zhejiang (LQ18H200001), the Natural Science Foundation of Ningbo (2017A610247, 20171JCGY01009), the Scientific Innovation Team Project of Ningbo (2017C110019) and the K.C. Wong Magna Fund in Ningbo University.
Author information
Authors and Affiliations
Contributions
Z.G., J.P., C.Z. designed the study, wrote and submit the manuscript. J.P. and C.Z. conducted the study. X.Z., J.H., H.T., W.S., Y.H., J.C. collected the clinical samples and performed the clinicopathologic analyses. J.P., C.Z., S.F., X.M., X.J. performed the qRT-PCR and data analyses.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pan, J., Zhou, C., Zhao, X. et al. A two-miRNA signature (miR-33a-5p and miR-128-3p) in whole blood as potential biomarker for early diagnosis of lung cancer. Sci Rep 8, 16699 (2018). https://doi.org/10.1038/s41598-018-35139-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-35139-3
Keywords
This article is cited by
-
microRNA-128-3p inhibits proliferation and accelerates apoptosis of gastric cancer cells via inhibition of TUFT1
World Journal of Surgical Oncology (2023)
-
Using the Precision Lasso for gene selection in diffuse large B cell lymphoma cancer
Journal of the Egyptian National Cancer Institute (2023)
-
Differential early diagnosis of benign versus malignant lung cancer using systematic pathway flux analysis of peripheral blood leukocytes
Scientific Reports (2022)
-
HIV-infection and cocaine use regulate semen extracellular vesicles proteome and miRNAome in a manner that mediates strategic monocyte haptotaxis governed by miR-128 network
Cellular and Molecular Life Sciences (2022)
-
Down-regulation of SNHG16 alleviates the acute lung injury in sepsis rats through miR-128-3p/HMGB3 axis
BMC Pulmonary Medicine (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
