
Abstract
To explore the individual effect and interaction of diabetes and family history and other risk factors on hypertension in Han in Shanghai China. The method of case–control study with l:l matched pairs was used, 342 cases of hypertension and 342 controls were selected and investigate their exposed factors with face-to-face. The method of epidemiology research was used to explore the individual effect and interaction of diabetes and family history and other risk factors on hypertension. The individual effect of family history (OR = 4.103, 95%CI 2.660–6.330), diabetes (OR = 4.219, 95%CI 2.926–6.083), personal taste (OR = 1.256, 95%CI 1.091–1.593), drinking behavior (OR = 1.391, 95%CI 1.010–1.914) and smoking behavior (OR = 1.057, 95%CI 1.00–1.117) were significant (p < 0.05). But individual effect of sex, education, occupation, work/life pressure, environmental noise, sleeping time and sports habit were not significant (p > 0.05). The OR of interaction between FH and DM to hypertension was 16.537 (95%CI 10.070–21.157), between FH and drinking behavior was 4.0 (95%CI 2.461–6.502), FH and sport habit was 7.668 (95%CI 3.598–16.344), FH and personal taste was 6.521 (95%CI 3.858–11.024), FH and smoking behavior was 5.526 (95%CI 3.404–8.972), FH and work/life pressure was 4.087 (95%CI 2.144–7.788). The SI of FH and DM was 2.27, RERI was 8.68, AP was 52.48% and PAP was 55.86%. FH and DM, personal taste, smoking behavior had positive interaction on hypertension, but FH and sport habits, drinking behavior, work/life pressure had reverse interaction on hypertension. FH and diabetes were very important risk factors with significant effect for hypertension. FH and diabetes, personal taste, smoking behavior had positive interaction on hypertension, but FH and sport habits, drinking behavior, work/life pressure had reverse interaction on hypertension.
Similar content being viewed by others

Introduction
Hypertension is a multifactorial disease caused by genetic and acquired environmental factors, the role of gene and gene, as well as between gene and acquired environmental factors, including among acquired risk factors, leads to increased risk of hypertension and disease among different populations. Unhealthy lifestyle including obesity and lack of exercise can significantly increase hypertension incidence1,2,3,4. The study result from familial aggregation showed that the prevalence rate of brothers and sisters in offspring was from 20 to 66% in positive population of parents, the estimated possibility of hereditary was over 50% in a plurality of twin studies5,6. It showed that more than half of the blood pressure changed could be attributed to the accumulation of genetic effects.
In fact, the individual effect of single factor on the result could not truly reflect the actual effect of factors, because there was interaction between risk factors, which might weaken the role of single factor, or enhance the role of single factor. Therefore, the interaction between factors may be more able to reflect the real relationship between factors and results. There were many studies on the influencing factors of hypertension at home and abroad, but there were few reports on the interaction between the influencing factors of hypertension.
There were two models to analyze biological interaction: addition and multiplication. To explore the risk factors and etiological factors of hypertension from the perspective of environment and genetics, and to carry out effective etiological prevention are the fundamental countermeasures and measures to reduce the incidence of hypertension. It might be of public health significance to explore the interaction with additive model. Therefore, this study selected additive model to analyze the interaction between family history of hypertension and diabetes and other exposed factors on the incidence of hypertension.
Methods
Source of cases and controls
All cases were randomly selected from hypertension registry and follow-up management system in Jiading district in Shanghai, and all controls were randomly selected from the community population. The cases of this study were patients with hypertension who have been definitely diagnosed in the hospital and had been using antihypertensive drugs (SBP ≥ 140 mmHg or DBP ≥ 90 mmHg without using antihypertensive drugs). The controls of this study was non hypertensive patients, their blood pressure were SBP < 140 mmHg and DBP < 100 mmHg and unused antihypertensive drugs. According to l:l matched pairs design, all controls had no hypertension, and controls were required the same sex, same race, living in the same community as cases, and the difference of age was not more than 5 years old and at the same age group. Every case or control gave informed consent to participate in the study which was approved by the local ethics committee (JD-2016-KY-18). They were able to correctly respond to the investigators for the health information of themselves and their nuclear family members.
Investigation method and content
Investigation was conducted by trained public health investigators, using a unified questionnaire. Using direct survey method, the contents of the questionnaire mainly include: age, sex, age of onset, diagnosis time, hospital name, diabetes history and so on. The criteria for judging whether all the respondents had essential hypertension and diabetes (all relatives of cases and controls): whether they had been diagnosed with essential hypertension or diabetes in the hospital before this investigation. If they had been diagnosed with essential hypertension in the hospital, it is “Yes”; if they had not been diagnosed, it is “No”.
Statistical analysis
Statistical analyses were performed using the statistical software package (IBM SPSS statistics version 21). When P values < 0.05, the difference was considered statistically significant. Mean and standard deviation (SD) were used to compute for quantitative variables (age and so on), and comparisons between groups were performed by t-test. Number (n) and percentage (%)) were computed for the categorical data, comparisons between groups were performed by the chi-square (χ2) test. Multivariate logistic regression analyses were conducted for investigated risk factors, odds ratios (OR) and 95% confidence intervals (CI) were calculated. In multivariate analysis, OR were adjusted by sex. The additive model was used by cross analysis to calculate the additive interaction effect1. The calculated indicators were SI (synergistic effect index), RERI (relative excess risk due to interaction), AP (attributable proportion due to interaction) and PAP (the percentage of the interaction between the pure factors).
Statement
All methods were carried out in accordance with relevant guidelines and regulations. The investigated object, content and methods of study were implemented according to the design scheme and technical route.
Ethics approval and consent to participate
Ethical approval was granted by Jiading district center for disease control and prevention research ethics committee. All subjects gave informed consent to participate in the study, they would like to participate in investigation and answer all the related questions in the questionnaire.
Results
Individual effect analysis
Among 684 investigated participants (342 hypertension cases and 342 controls) aged 28–87 years old in this study, male was 50.73%, female was 49.27%. 76.17% participants had family history of hypertension, 23.83% had not. Between case group and control group, the statistical test results showed that the difference of sex, education level, work and life pressure, living environmental noise, person's taste, sleeping time, sports habit, drinking behavior and smoking behavior was no significant (p > 0.05). But the difference of family history (FH) and occupation between case group and control group was significant (p < 0.05). The difference of mean age between case group and control group was no significant (t = 0.894, p = 0.372).
The result of logistic regression analysis showed that individual effect of family history of hypertension, diabetes history, personal taste, drinking behavior and smoking behavior were significant (p < 0.05). But individual effect of sex, education, occupation, work/life pressure, environmental noise, sleeping time and sports habit were not significant (p > 0.05). See Table 1.
The OR result showed that family history of hypertension, diabetes history, drinking behavior and smoking behavior were important risk factors to hypertension. The OR between family history and hypertension was 4.103 (95%CI 2.660–6.330); the OR between diabetes history and hypertension was 4.219 (95%CI 2.926–6.083); the OR between drinking behavior and hypertension was 1.391 (95%CI 1.010–1.914); the OR between smoking behavior and hypertension was 1.057 (95%CI 1.000–1.117). The OR between personal taste and hypertension was 1.256 (95%CI 1.091–1.593). See Table 1.
Interaction analysis
Interaction of family history and diabetes
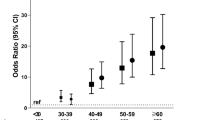
The effect of risk factors on the occurrence of hypertension was often not independent; they often interacted with each other and promoted the occurrence of hypertension through interaction. In order to explore the interaction between family history and diabetes, the methods of interactive effects analysis was used. Table 2 shows the result of interactive effects between family history and diabetes. The OR of interaction between family history and diabetes to hypertension was 16.537, the OR of family history and diabetes to hypertension were respectively 4.505 and 4.354. OR(FH+DM) > ORFH + ORDM. It was showed that family history and diabetes have positive interaction with hypertension.
According the result of Table 3, additive model was used to calculate the additive interaction effect: the synergistic effect index (SI) of family history and diabetes to hypertension was 2.27; relative excess risk due to interaction (RERI) was 8.68; Attributable proportion due to interaction (AP) was 52.48%; and the percentage of the interaction between the pure factors (PAP) was 55.86%. The result of PAP indicated that 55.86% of hypertension was attributable to the interaction of them, when exposed to both family history and diabetes risk factors.
Interaction of FH and other risk factors
In order to better observe the interaction between family history (FH) and other risk factors (drinking behavior, sport habits, personal taste, smoking behavior and work/life pressure), we changed behavior from three categories (no, occasionally and regular) to two categories (yes or no), the combination of occasionally drinking and regular drinking was yes (have drink behavior); occasionally sport and regular sport was yes (have sport habits). The same as, balance taste and light taste was no salty; occasionally and regular smoking behavior was yes (smoking), little and more work/life pressure was have pressure.
The result showed OR of interaction between FH and drinking behavior to hypertension was 4.0, the OR of family history and smoking behavior to hypertension were respectively 4.942 and 0.741. OR(FH+Dr) < ORFH + ORDr. It was showed that FH and drinking behavior have reverse interaction on hypertension. See Table 3.
The result showed OR of interaction between FH and sport habits to hypertension was 7.668, the OR of family history and sport habits to hypertension were respectively 8.571 and 1.773. OR(FH+S) < ORFH + ORS. It was showed that FH and sport habits have reverse interaction on hypertension. See Table 4.
The result showed OR of interaction between FH and taste preference to hypertension was 6.521, the OR of family history and taste preference to hypertension were respectively 4.840 and 1.386. OR(FH+T) > ORFH + ORT. It was showed that FH and taste preference (salty) have positive interaction on hypertension. See Table 5.
The result showed OR of interaction between FH and smoking behavior to hypertension was 5.526, the OR of family history and smoking behavior to hypertension were respectively 4.359 and 0.871. OR(FH+Sm) > ORFH + ORSm. It was showed that FH and smoking behavior have positive interaction on hypertension. See Table 6.
The result showed OR of interaction between FH and work/life pressure to hypertension was 4.087, the OR of family history and work/life pressure to hypertension were respectively 5.217 and 2.229. OR(FH+P) < ORFH + ORP. It was showed that FH and work/life pressure have reverse interaction on hypertension. See Table 7.
Discussion
The factors influencing the occurrence of hypertension include congenital factors and natural factors, congenital factors refer to hereditary factors such as genes or family history, acquired factors mainly include bad living habits, overweight / obesity, etc. Body mass index was a comprehensive indicator of the outcome of acquired lifestyle, and closely related to the occurrence of hypertension7,8,9,10,11,12. Family history of hypertension was an important marker of genetic factors, it was often used as an alternative indicator to study the relationship between genetic factors and diseases13,14,15,16. Previous studies had not been considered the interaction between genetic and environmental factors. More attention needed to pay to the related research, to evaluate the relationship between polymorphic gene and exposed factors. Hypertension and diabetes usually occurred successively, due to the hardening of blood vessels diabetes could induce hypertension17,18,19.
There were many risk factors for hypertension, such as smoking, drinking, mental tension, lack of exercise, family genetics and so on20,21. In this study, the result showed that effect of family history of hypertension, diabetes history, personal taste, drinking behavior and smoking behavior were significant (p < 0.05). But effect of education, occupation, work/ life pressure, environmental noise, sleeping time and sports habit were not significant (p > 0.05). The OR result showed that family history of hypertension, diabetes history and drinking behavior were important risk factors to hypertension. The OR of family history of hypertension was 4.103, diabetes history was 4.219, drinking behavior was 1.391, smoking behavior was 1.057. This result showed that family history of hypertension, diabetes history, drinking behavior and smoking behavior were important factors of hypertension, especially family history and diabetes.
Hypertension was one of the common complications of diabetes; the incidence of hypertension in domestic diabetes patients with hypertension was 20–30%22,23. The OR of interaction between family history and diabetes to hypertension was 16.537. It was showed that FH and DM have positive interaction with hypertension. The percentage of the interaction between the pure factors (PAP) was 55.86%, it indicated that 55.86% of hypertension was attributable to the interaction of them, when exposed to both family history and diabetes risk factors. Because the disorder of glucose metabolism could accelerate the hardening of renal artery and systemic arteriole, increase the peripheral resistance and blood pressure, hyperglycemia can increase blood volume, overload the kidneys, retention of water and sodium, and eventually raise blood pressure. The increase of blood pressure was related to cardiac output and peripheral resistance. The increase of cardiac output without peripheral change could lead to the rise of blood pressure; the increase of peripheral resistance without the change of cardiac output or blood volume could also lead to the rise of blood pressure, and both changes of diabetic patients led to the rapid rise of blood pressure and serious complications.
Alcohol was one of the risk factors of hypertension24,25,26,27. Long term small amount of alcohol could increase blood pressure; small amount of alcohol could increase blood pressure, heart rate and heart load of patients with hypertension. In this study, the result of the logistic regression analysis showed that drinking behavior were risk factor to hypertension, the OR of drinking behavior was 1.391. Family history of hypertension and drinking behavior had reverse interaction on hypertension. This might be due to the interference of occasional drinking behavior, small amount of alcohol may have vascular protection. It needs further study.
High salt intake in salt sensitive individuals could lead to elevated blood pressure by affecting water and sodium metabolism, vascular function and sympathetic nervous system28,29. In this study, the result of the logistic regression analysis showed that personal taste were risk factor to hypertension, the OR of personal taste was 1.256. Family history of hypertension and drinking behavior had positive interaction on hypertension. The lower of 95%CI of OR < 1 (0.991), perhaps it was related to the fact that Shanghai residents generally like light food. It needs further study.
Smoking is a risk factor for cardiovascular disease, and smoking is associated with hypertension30,31. In this study, the result of the logistic regression analysis showed that smoking behavior were risk factor to hypertension, the OR of personal taste was 1.256. Family history and smoking behavior had positive interaction on hypertension.
Due to space limitation, only the interaction between family history and several common acquired factors were analyzed in this study. In fact, there were also interactions among acquired factors, and the interaction among multiple factors may be even more different. In short, the individual effect of single factor was strong did not mean that it must be very important role in the outcome of disease, the individual effect of single factor was weak did not mean that it must be very unimportant role in the outcome of disease. Pay attention to the interaction between factors, and expect more and better research results appear.
Conclusion
Family history and diabetes were very important risk factors with significant effect for hypertension. FH and DM, taste preference, smoking behavior had positive interaction with hypertension, but FH and sport habits, drinking behavior, work/life pressure had reverse interaction with hypertension.
Data availability
The questionnaire and database supporting the conclusions of this article are available, through contact with anle_li@aliyun.com.
References
Li, A. L., Peng, Q., Shao, Y. Q., Fang, X. & Zhang, Y. Y. The effect of body mass index and its interaction with family history on hypertension: A case-control study. Clin. Hypertens. 25(6), 1–8 (2019).
Zaw, K. K. et al. Prevalence of hypertension and its associated factors in the adult population in Yangon Division, Myanmar. Asia Pac. J. Public Health 23(4), 496–506 (2011).
Center for chronic non communicable diseases control and prevention of China Center for Disease Control and Prevention. Surveillance report of chronic diseases and their risk factors in China (2010) (Military Medical Science Press, Beijing, 2012).
Ehrel, G. B. Genome-wide association studies: Contribution of genomic to understanding blood pressure and essential hypertension. Curr. Hypertens. Rep. 12, 17–25 (2010).
Li, A. L., Fang, X., Zhang, Y. Y., Peng, Q. & Yin, X. H. Familial aggregation and heritability of hypertension in Han population in Shanghai China: A case-control study. Clin. Hypertens. 25(17), 1–7 (2019).
Levy, D. et al. Genome-wide association study of blood pressure and hypertension. Nat. Genet. 41(6), 677–687 (2009).
Millar, S., Perry, I. J. & Phillips, C. M. Surrogate measures of adiposity and cardio- metabolic risk—why the uncertainty? A review of recent meta-analytic studies. J. Diabetes Metab. S11, 004 (2013).
Tadic, M. et al. The association between obesity, blood pressure variability and right ventricular function and mechanics in hypertensive patients. J. Am. Soc. Echo Cardiogr. 29(8), 802–811 (2016).
Tadic, M. et al. The interaction between blood pressure variability, obesity, and left ventricular mechanics: Findings from the hypertensive population. J. Hypertens. 34(4), 772–780 (2016).
Manimunda, S. P. et al. Association of hypertension with risk factors & hypertension related behaviour among the aboriginal Nicobarese tribe living in Car Nicobar Island, India. Indian J. Med. Res. 133(3), 287–293 (2011).
Kotchen, T. A. Obesity-related hypertension: Epidemiology, pathophysiology, and clinical management. Am. J. Hypertens. 23(11), 1170–1178 (2010).
Modesti, P. A. et al. Cardiovascular risk assessment in low-resource settings: A consensus document of the European Society of Hypertension Working Group on Hypertension and Cardiovascular Risk in Low Resource Settings. J. Hypertens. 32(5), 951–960 (2014).
Ehret, G. B. et al. Genetic variants in novel pathways influence blood pressure and cardiovascular disease risk. Nature 478(7367), 103–109 (2011).
Kato, N. et al. Meta-analysis of genome-wide association studies identifies common variants associated with blood pressure variation in east Asians. Nat. Genet. 43(6), 531–538 (2011).
Zhang, Y. et al. A rare variant at the KYNU gene is associated with kynurenines activity and essential hypertension in the Han Chinese population. Circ. Cardiovasc. Genet. 4(6), 687–694 (2011).
Rafiq, S., Anand, S. & Roberts, R. Genome-wide association studies of hypertension: Have they been fruitful?. Cardiovasc. Transl. Res. 3(3), 189–196 (2010).
Raikou, V. D. & Gavriil, S. Body-mass index and the risk of albuminuria in hypertensive patients with a poor estimated glomerular filtration rate and the potential role of diabetes mellitus. Diabetes Metab. Syndr. 13(2), 1041–1046 (2019).
Ren, Q., Ma, C.-S., Wang, J.-G., Guo, X.-H. & Jia, L.-N. Albuminuria and other target organ damage in Chinese patients with hypertension and diabetes: A data analysis based on the ATTEND study. J. Diabetes Complicat. 34(1), 1070–1074 (2020).
Shibata, D. et al. Vascular risk factors and findings on brain MRI of elderly adult American Indians: The strong heart study. Neuro Epidemiol. 52(3–4), 173–180 (2019).
Liu, L. S. et al. 2018 Chinese guidelines for prevention and treatment of hypertension—a report of the revision committee of Chinese guidelines for prevention and treatment of hypertension. J. Geriatr. Cardiol. 16(3), 182–241 (2019).
Williams, B. et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. https://doi.org/10.1093/eurheartj/ehy339 (2018).
Wang, L., Li, J., Li, Y., Yao, S., Zhao, M. & Wang, C. The effects of hypertension and diabetes on new-onset chronic kidney disease: A prospective cohort study [J]. J. Clin. Hypertens. (2019).
Liu, J. et al. Prevalence of diabetes mellitus in out patients with essential hypertension in China: A cross-sectional study. BMJ Open. 3(11), e003798 (2013).
Jung, M. H. et al. The effect of alcohol dose on the development of hypertension in Asian and Western men: Systematic review and meta-analysis. Korean J. Intern. Med. https://doi.org/10.3904/kjim.2019.016 (2019).
Tatsumi, Y. et al. Hyperuricemia predicts the risk for developing hypertension independent of alcohol drinking status in men and women: The Saku study. Hypertens. Res. https://doi.org/10.1038/s41440-019-0361-0 (2019).
Puddey, I. B., Mori, T. A., Barden, A. E. & Beilin, L. J. Alcohol and hypertension-new insights and lingering controversies. Curr. Hypertens. Rep. 21(10), 79 (2019).
Arnold, C., Ullrich, C., Wensing, M. & Pfinder, M. Prenatal alcohol exposure and the associated risk of elevated blood pressure: A cross-sectional analysis of 3- to 17-year-olds in Germany. Am. J. Hypertens. 32(11), 1118–1125 (2019).
Bkaily, G., Simon, Y., Menkovic, I., Bkaily, C. & Jacques, D. High salt-induced hypertrophy of human vascular smooth muscle cells associated with a decrease in glycocalyx. J. Mol. Cell. Cardiol. https://doi.org/10.1016/j.yjmcc.2018.10.006 (2018).
Clemmer, J. S., Hester, R. L. & Pruett, W. A. Simulating a virtual population’s sensitivity to salt and uninephrectomy. J. R. Soc. Int. https://doi.org/10.1098/rsfs.2016.0134 (2018).
Ding, L. et al. Smoking, heavy drinking, physical inactivity, and obesity among middle-aged and older adults in China: Cross-sectional findings from the baseline survey of CHARLS 2011–2012. BMC Public Health https://doi.org/10.1186/s12889-020-08625-5 (2020).
Holanger, M., Kjeldsen, S. E., Jamerson, K. & Julius, S. Smoking and overweight associated with masked uncontrolled hypertension: A Hypertension Optimal Treatment (HOT) Sub-Study. Blood Press. https://doi.org/10.1080/08037051.2020.1787815 (2020).
Acknowledgements
Heartfelt thanks to all doctors, nurses and public health workers in 13 community health service centers in Jiading district in Shanghai for their hard work. Thank for some advice of the experts!
Funding
This study was funded by Jiading district health and family planning commission research project in Shanghai (No: 2016-KY-18).
Author information
Authors and Affiliations
Contributions
The original idea for the project was conceived by A.L.; Q.P., X.F. and Y.Z. participated in the collection of early data, quality control and gave a lot of administrative support. A.L. conceptualized the paper, analyzed data and wrote a first draft of the manuscript. All authors contributed to subsequent drafts and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, Al., Peng, Q., Shao, Yq. et al. The interaction on hypertension between family history and diabetes and other risk factors. Sci Rep 11, 4716 (2021). https://doi.org/10.1038/s41598-021-83589-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-83589-z
This article is cited by
-
The interaction between general or abdominal obesity and hypertension on the risk of type 2 diabetes mellitus: a cross-sectional analysis in Iranian adults from the RaNCD cohort study
BMC Public Health (2024)
-
The association of periodontal disease and oral health with hypertension, NHANES 2009–2018
BMC Public Health (2023)
-
Socioeconomic and behavioral determinants of non-compliance with physician referrals following community screening for diabetes, hypertension and hyperlipidemia: a mixed-methods study
Scientific Reports (2023)
-
Effects of additive interactions among obesity, visceral adiposity, and sarcopenia on nonalcoholic fatty liver disease
Scientific Reports (2023)
-
Risk probability and influencing factors of stroke in followed-up hypertension patients
BMC Cardiovascular Disorders (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
