
Abstract
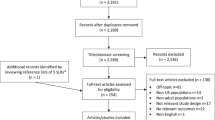
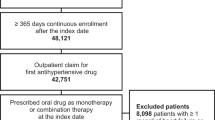
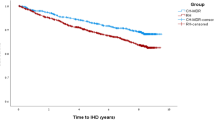
The objective was to assess persistence with antihypertensive therapy (AHT) and discontinuation patterns in patients newly dispensed different antihypertensive drug classes in a natural Canadian population-based setting. Hypertensive patients initiating AHT monotherapy were included in this 3-year retrospective cohort study (N=21 326) using the Saskatchewan health-care databases. Persistence was defined as consistently refilling a new prescription for AHT within 90 days of a previous dispensing. New courses of AHT were also documented in nonpersistent patients. Kaplan–Meier and Cox regression analyses were used to compare persistence and new courses of therapy across initial drugs. Compared to the newer angiotensin II antagonists (AIIAs), the likelihood of discontinuing therapy over the 39-month study period was significantly higher for angiotensin-converting enzymes inhibitors (HR=1.29; 95% CI=1.16–1.43), calcium channel blockers (HR=1.42; 95% CI=1.27–1.60), beta blockers (HR=1.62; 95% CI=1.45–1.80) and diuretics (HR=1.92; 95% CI=1.73–2.14). In the year following treatment discontinuation, between 54 and 75% of patients initiated a second course of treatment. Patients initiated on an AIIA had a significantly higher likelihood of starting a new course of therapy after a first treatment discontinuation, compared to all other agents. In conclusion, hypertensive patients initiated on an AIIA not only had greater persistence to AHT but were also more likely to initiate a new course of AHT after discontinuation than those initiating treatment with other agents. Further studies are required that relate intermittent treatment behaviours to health outcomes and costs in hypertension.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others
References
The Heart and Stroke Foundation of Canada. The Growing Burden of Heart Disease and Stroke in Canada, 2003. Health Canada: Ottawa, 2003.
Chobanian AV et al. Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003; 42: 1206–1252.
Joffres MR et al. Awareness, treatment, and control of hypertension in Canada. Am J Hypertens 1997; 10(10 Part 1): 1097–1102.
Paramore LC et al. Impact of poorly controlled hypertension on healthcare resource utilization and cost. Am J Managed Care 2001; 7: 389–398.
Khan NA et al. Canadian Hypertension Education Program. The 2004 Canadian recommendations for the management of hypertension: Part II — Therapy. Can J Cardiol 2004; 20: 41–54.
Whitworth JA;, World Health Organization, International Society of Hypertension Writing Group. 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens 2003; 21: 1983–1992.
Joffres MR, MacLean DR . Comparison of the prevalence of cardiovascular risk factors between Quebec and other Canadian provinces: the Canadian heart health surveys. Ethn Dis 1999; 9: 246–253.
MacMahon S et al. Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 1990; 335: 765–774.
Gueyffier F et al. Effect of antihypertensive drug treatment on cardiovascular outcomes in women and men. A meta-analysis of individual patient data from randomized, controlled trials. The INDANA Investigators. Ann Intern Med 1997; 126: 761–767.
Collins R et al. Blood pressure, stroke, and coronary heart disease. Part 2, Short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet 1990; 335: 827–838.
Urquhart J . Some economic consequences of noncompliance. Curr Hypertens Rep 2001; 3: 473–480.
McCombs JS, Nichol MB, Newman CM, Sclar D . The costs of interrupting antihypertensive drug therapy in a Medicaid population. Med Care 1994; 32: 214–226.
Hughes D, McGuire A . The direct costs to the NHS of discontinuing and switching prescriptions for hypertension. J Hum Hypertens 1998; 12: 533–537.
Jones JK et al. Discontinuation of and changes in treatment after start of new courses of antihypertensive drugs: a study of a United Kingdom population. BMJ 1995; 311: 293–295.
Monane M et al. The effects of initial drug choice and comorbidity on antihypertensive therapy compliance: results from a population-based study in the elderly. Am J Hypertens 1997; 10(7 Part 1): 697–704.
Okano GJ et al. Patterns of antihypertensive use among patients in the US Department of Defense database initially prescribed an angiotensin-converting enzyme inhibitor or calcium channel blocker. Clin Ther 1997; 19: 1433–1445 discussion 1424-5.
Caro JJ et al. Persistence with treatment for hypertension in actual practice. Can Med Assoc J 1999; 160: 31–37.
Caro JJ et al. Effect of initial drug choice on persistence with antihypertensive therapy: the importance of actual practice data. Can Med Assoc J 1999; 160: 41–46.
Bourgault C, Rainville B, Suissa S . Antihypertensive drug therapy in Saskatchewan: patterns of use and determinants in hypertension. Arch Intern Med 2001; 161: 1873–1879.
Bloom BS . Continuation of initial antihypertensive medication after 1 year of therapy. Clin Ther 1998; 20: 671–681.
Hasford J, Mimran A, Simons WR . A population-based European cohort study of persistence in newly diagnosed hypertensive patients. J Hum Hypertens 2002; 16: 569–575.
Degli EL et al. A retrospective, population-based analysis of persistence with antihypertensive drug therapy in primary care practice in Italy. Clin Ther 2002; 24: 1347–1357 discussion 1346.
Marentette MA, Gerth WC, Billings DK, Zarnke KB . Antihypertensive persistence and drug class. Can J Cardiol 2002; 18: 649–656.
Gregoire JP et al. Determinants of discontinuation of new courses of antihypertensive medications. J Clin Epidemiol 2002; 55: 727–734.
Conlin PR et al. Four-year persistence patterns among patients initiating therapy with the angiotensin II receptor antagonist losartan versus other antihypertensive drug classes. Clin Ther 2001; 23: 1999–2010.
Malcolm E et al. Saskatchewan Health's linkable databases and pharmacoepidemiology. Post Marketing Surveillance 1993; 6: 175–264.
Downey W et al. Health databases in Saskatchewan. In: Strom BL (ed) Pharmacoepidemiology, 3rd edn. John Wiley & Sons Ltd: Chichester (England), 2000, pp 325–345.
World Health Organization. The International Classification of Diseases: Ninth revision (ICD-9). Office of Publications World Health Organization: Geneva, 1978.
Degli EE et al. Long-term persistence with antihypertensive drugs in new patients. J Hum Hypertens 2002; 16: 439–444.
Rogers PG, Bullman WR . Prescription medicine compliance: a review of the baseline of knowledge. A report of the National Council on Patient Information and Education. J Pharmacoepidemiol 1995; 3(2): 3–36.
Gregoire JP et al. Tolerability of antihypertensive drugs in a community-based setting. Clin Ther 2001; 23: 715–726.
Ambrosioni E . Pharmacoeconomics of hypertension management: the place of combination therapy. Pharmacoeconomics 2001; 19: 337–347.
Caro JJ, Speckman JL . Existing treatment strategies: does noncompliance make a difference? J Hypertens –Supplement 1998; 16: S31–S34.
Hughes D, McGuire A . The direct costs to the NHS of discontinuing and switching prescriptions for hypertension. J Hum Hypert 1998; 12: 533–537.
Billups SJ, Malone DC, Carter BL . The relationship between drug therapy noncompliance and patient characteristics, health-related quality of life, and health care costs. Pharmacotherapy 2000; 20: 941–949.
McCombs JS, Nichol MB, Newman CM, Sclar DA . The costs of interrupting antihypertensive drug therapy in a Medicaid population. Med Care 1994; 32: 214–226.
Rizzo JA, Simons WR . Variations in compliance among hypertensive patients by drug class: implications for health care costs. Clin Ther 1997; 19: 1446–1457.
Christensen DB et al. Comparison of prescription and medical records in reflecting patient antihypertensive drug therapy. Ann Pharmacother 1994; 28: 99–104.
Choo PW et al. Validation of patient reports, automated pharmacy records, and pill counts with electronic monitoring of adherence to antihypertensive therapy. Med Care 1999; 37: 846–857.
Acknowledgements
Funding for this study was contributed by Merck Frosst Canada Ltd, Kirkland, QC, Canada. Parts of these results were presented at the 20th International Conference on Pharmacoepidemiology & Therapeutic Risk Management, Bordeaux, France, August 24, 2004.
This study is based on administrative data provided by the Saskatchewan Department of Health. The interpretation and conclusions contained herein do not necessarily represent those of the Government of Saskatchewan or the Saskatchewan Department of Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bourgault, C., Sénécal, M., Brisson, M. et al. Persistence and discontinuation patterns of antihypertensive therapy among newly treated patients: a population-based study. J Hum Hypertens 19, 607–613 (2005). https://doi.org/10.1038/sj.jhh.1001873
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jhh.1001873
Keywords
This article is cited by
-
Personalized hypertension treatment recommendations by a data-driven model
BMC Medical Informatics and Decision Making (2023)
-
Non-persistence to antihypertensive drug therapy in Lithuania
European Journal of Clinical Pharmacology (2022)
-
The benefit of angiotensin AT1 receptor blockers for early treatment of hypertensive patients
Internal and Emergency Medicine (2017)
-
Quality of Life in Treatment-Resistant Hypertension
Current Hypertension Reports (2015)
-
Antihypertensive drug treatment changes in the general population: the colaus study
BMC Pharmacology and Toxicology (2014)
