
Abstract
Purpose
To describe the management of vitreoretinal complications of sickle cell retinopathy.
Design
A retrospective interventional case series
Methods
Review of an electronic patient record and clinical notes of 27 patients with vitreoretinal complications of sickle retinopathy.
Results
Six male patients and 21 female patients presented with a mean age of 41 years (range 28–67), 12 left eyes and 16 right eyes. The mean follow-up was 15.5 months (range: 3–60). Two patients were SS, and the remainders were doubly heterozygous (SC). In all, 10 were observed without surgery— three with vitreous haemorrhage, four tractional retinal detachments (TRD), and three rhegmatogenous retinal detachments (RRD). Two patients demonstrated spontaneous flattening of the retina— one RRD and one TRD. Eighteen eyes had pars plana vitrectomies (PPVs)— seven with vitreous haemorrhage, three RRD, three TRD, three ERM (one bilateral), and two macular holes. In all, 15 patients (83%) had improved vision postoperatively. The mean logMar preoperative visual acuity was 1.07 (Snellen equivalent 6/70), SD 0.62 was significantly improved postoperatively (mean 0.42 (6/15), SD 0.48, P=0.001).
Conclusions
Sickle retinopathy occasionally presents with vitreoretinal complications. These can often be observed and may spontaneously regress. If surgery is required eyes respond to vitrectomy procedures with segmentation of sea fan proliferation.
Similar content being viewed by others


Introduction
Sickle cell haemoglobinopathies result from an abnormality in the β-chain of the haemoglobin molecule. This causes chronic haemolytic anaemia and vaso-occlusive crises and a number of clinical features in the eye.1, 2 The conjunctival and optic nerve head blood vessels show characteristic segmentation of blood columns in the homozygous sickle cell disease (SS). In the retina, occlusion of the peripheral retinal vasculature occurs, accompanied by black sunburst spots, iridescent spots, retinal haemorrhages (salmon patches), and sea fan neovascular proliferation. Retinal complications are seen in 43% of patients aged between 20 and 30 years with doubly heterozygous (SC) sickle cell.3 These include vitreous haemorrhage, tractional retinal detachment (TRD), rhegmatogenous retinal detachment (RRD), macular epiretinal membrane (ERM), and macular hole.4 Reports of vitreoretinal surgery for these complications are few and tend to be from a period when scleral buckling and panretinal photocoagulation were used.5, 6, 7 More recent reports on modern vitreoretinal techniques in sickle cell retinopathy are lacking and yet there has been considerable development of surgical technique. In this report, we reviewed the records of patients with vitreoretinal complications of sickle cell retinopathy referred to tertiary referral centre at St Thomas' hospital in a 9-year period.
Materials and methods
Since 1997, the clinical details of patients attending the vitreoretinal service have been entered into an electronic patient record (available with the book Vitreoretinal Surgery, Springer). Clinical data at presentation and follow-up, operative procedure, and peroperative and postoperative complications are routinely recorded on the electronic patient record. A retrospective review of the database and the clinical records of all patients with sickle cell retinopathy with vitreoretinal disorders presenting to the vitreoretinal service at St Thomas' Hospital from November 1997 to November 2006 was performed. Data were collected on demographics, sickle cell status, clinical presentation, operative procedure, and postoperative outcome. Snellen visions were reviewed and converted into logMar for statistical analysis.
Patients were operated upon when there was evidence of recent loss of vision, or a threat to vision was perceived when the observation was employed. Routine 20-gauge PPV was employed with general anaesthesia or subtenon's local anaesthesia exchange transfusions have been given during surgery in the past these were not used.8 All procedures were performed using a BIOM wide-angle viewing system. Segmentation of peripheral neovascular scar tissue was performed with vertical cutting scissors with trimming of the complexes with the vitrectomy cutter as required. Initially, delamination of the peripheral neovascular complexes was attempted, but the complexes were found to be too adherent for the removal of ‘en bloc’ and the process caused iatrogenic retinal tear formation and was later abandoned. No patients had peripheral retinectomy or feeder vessel laser. No attempt was made to regress sea fan neovascularisation by scatter laser, but one patient with significant diabetic retinopathy received peroperative pan retinal photocoagulation.
Pupils were dilated with topical phenylephrine 2.5% and cyclopentolate 1% preoperatively (peroperative epinephrine was not used). During the 1 month postoperatively, topical maxitrol was prescribed q.d.s. and atropine 1% b.i.d. No patients had need for antiocular hypertensive therapy outside the immediate postoperative period of 2 months. Paired student's t-test was employed where appropriate. The study conformed to the Declaration of Helsinki.
Results
Twenty-eight patients with sickle cell retinopathy were referred to the retinal service with vitreoretinal conditions over a 9-year period representing 4.6% of the patients registered with the sickle service at the hospital. A 39-year-old male patient presented with RRD and was operated upon by vitrectomy and silicone oil insertion, but defaulted from the follow-up and was excluded from the analysis. There were six male patients and 21 female patients with a mean age of 41 years (range: 28–67). The patients represent 0.8% of the patients referred for surgery to the service. Two patients were pregnant at presentation, both with vitreous haemorrhage. Twelve left eyes and 16 right eyes were observed with vitreoretinal pathology, one patient had bilateral ERM. Where ethnic data were provided by the patients, they were black African or Caribbean. In all, 18 eyes of 17 patients were operated on and 10 patients were observed. The mean follow-up was 15.5 months (range: 3–60 months). Two patients were homozygous SS, and the remainders were SC. Two patients were type 2 diabetic, one had signs consistent with diabetic retinopathy as well as sickle cell retinopathy and the other had no signs consistent with diabetic retinopathy. The results are summarised in Tables 1 and 2.
Patients who were observed without surgical intervention
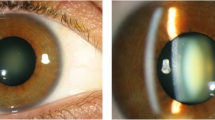
The presentations and visual outcomes of 10 patients who were observed without surgical intervention are shown in Table 1. Two patients demonstrated spontaneous resolution of their retinal conditions. A 40-year-old female SC patient with RRD refused surgery because of a poor outcome of surgery in her sister in the past. She had an attached vitreous gel, and during observation, spontaneously reattached the retina at 6 months with 6/6 vision maintained after 4 years of follow-up, Figures 1 and 2. A 38-year-old female SC patient, who presented with TRD and ERM (macular pucker membrane with attached vitreous) with pseudo hole, had spontaneous separation of the ERM off the retina with resolution of the TRD during PVD formation. Thereafter, the ERM could be seen on the posterior hyaloid surface. Her final vision was 6/18.

A 40-year-old female doubly heterozygous patient with RRD refused surgery because of a poor outcome of surgery in her sister in the past. The RRD edge can be seen.

During observation, the retina has spontaneously reattached with 6/6 vision maintained after 4 years of follow-up. Retinal pigment changes are visible in the area of reattachment of the retina.
Patients requiring surgical intervention
Eighteen eyes of 17 patients received surgery (one patient with bilateral macular pucker ERM had both eyes operated upon) with one vitreoretinal procedure per eye in 16 eyes, and two procedures in each of the remaining two eyes, Tables 2 and 3. Operative complications were seen in 11 patients, postoperative vitreous cavity haemorrhage in two patients operated upon for vitreous haemorrhage. One required repeat PPV, the other resolved without further surgery. Iatrogenic breaks were created in seven patients, which were treated by laser retinopexy or cryotherapy and internal gas tamponade, sulphahexafluoride or perfluoropropane (one of these was subsequently the patient who required silicone oil insertion at a second procedure and ultimately failed). Three cataracts were seen postoperatively one of which was scheduled for surgery, but spontaneously reabsorbed after a bout of uveitis. This patient was eventually left aphakic with a vision of 6/18 with contact lens correction.
In all, 15 of 18 eyes (83%) had improved vision postoperatively. The mean logMar preoperative visual acuity was 1.07 (Snellen equivalent 6/70, SD 0.62, 95% confidence interval 0.76–1.38), and was significantly improved postoperatively with a mean of 0.42 (6/15) (SD 0.48, confidence interval 0.21–0.56, P=0.001) Figure 3. All patients with RRD achieved flat retinas; two of three patients with TRD had a flat retina postoperatively. A patient with TRD presented with active neovascularisation, which included the features of diabetic retinopathy and sickle cell retinopathy (the patient had type 2 diabetes mellitus). This patient required two PPVs, the second with silicone oil insertion because of inferior retinal detachment and traction from localised proliferative vitreoretinopathy. She had 6/60 vision at the follow-up with persistent inferior retinal detachment under silicone oil.

A scattergram of the logMar visual acuities of those patients who had pars plana vitrectomy for the complications of sickle cell retinopathy.
Discussion
Descriptions of vitreoretinal surgery for the management of the complications of sickle cell retinopathy are very few (the most recent one in 1988).8 Vitreoretinal surgery has gradually evolved since these early descriptions. As part of that evolution, there is less use of scleral buckling or scatter photocoagulation9 (which has been used both preoperatively10 and peroperatively11) in many centres. Both interventions were associated with the development of anterior segment ischaemia in these patients,11, 12 a complication rarely seen today.7 The use of scatter laser as a means of regressing neovascularisation is controversial because of the high incidence of autoinfarction of the retinal proliferation in 30%.13, 14 In this study, all patients who received surgery were treated by PPV without external plombage or scatter laser—no cases of anterior segment ischaemia were encountered. Occlusion of the feeder vessels supplying sea fans has been employed but was not used in our study. Feeder vessel laser has been associated with retinal break formation and choroidal neovascularisation, but has been shown in a small randomised study to reduce the risk of vitreous haemorrhage.15, 16 It has been used to treat a patient with exudative retinal detachment apparently from sickle cell retinopathy.17 The patients described in this study were advanced cases (Goldberg stages 4 and 5). It is possible that laser interventions may be more advantageous to patients with earlier manifestations of the condition.
A description of the natural history of the condition (with patients with an age group similar this study) has demonstrated a moderate risk of vitreous haemorrhage (5.3%) and macular lesions (4.6%), and a low risk of retinal detachment (2%) over a mean follow-up of 6.3 years.1 In one study, blindness in patients with proliferative vitreoretinopathy was seen in 12%.14 However, in a larger study of young patients in Jamaica (307 patients with SS and 166 with SC), followed for 20 years up to the age of 26 years, only two patients had sight-threatening disease, one patient suffering irreversible sight loss in one eye and one patient with a successfully treated RRD.3 The Jamaican study provides the best incidence information available to date on complications from a population group. Patients in our study presented with vitreous haemorrhage, TRD, RRD, and macular disorders, such as ERM and macular holes. The numbers of patients were small preventing meaningful analysis for the prediction of visual outcome in these patients according to their presentation pattern. However, combining all of the patients together, the surgical outcomes for visions were good with 10 of 18 eyes achieving 6/12 vision or better, and 15 eyes (83%) with improved vision postoperatively. This is higher than the 50% success rates quoted elsewhere.12
Peroperative complications were frequent; in particular, we noted a high incidence of iatrogenic tear formation during PPV, especially around sea fan complexes during the study period. This has been noted before.18 It was our initial intention to delaminate the complexes in a similar fashion to diabetic neovascularisation. However, this was found to be surgically difficult as reflected by the formation of retinal tears and bleeding. Delamination was subsequently found to be unnecessary and abandoned as a practice. We found that the sea fans can be safely left in situ and that a segmentation technique used if necessary to remove vitreal attachments. There was no need to try to induce regression of the sea fans with scatter laser or feeder vessel laser.
In contrast to previous reports,18, 19 the rate of postoperative complications was low with only one patient requiring a repeat vitrectomy for recurrent vitreous haemorrhage and one patient for recurrent RD. Cataract formation after surgery was uncommon, perhaps relating to the young age of many of the patients or to the relative ischaemia of these eyes, which may protect against cataractogenesis as has been suggested in diabetic retinopathy.20
Not all patients with vitreoretinal complications from sickle cell retinopathy require surgery. We were able to observe 10 patients without signs of progression of their clinical features. Vitreous haemorrhage can be allowed to clear without detriment and TRD observed without apparent progression in some patients. Indeed, two patients showed spontaneous improvement, one patient with RRD, which reattached and one patient with TRD and ERM, which separated during PVD formation. Unfortunately, the numbers of patients were too small to determine an exact pattern of presentation that could lead to the spontaneous resolution.
In conclusion, sickle cell retinopathy occasionally presents with vitreoretinal complications. These can often be observed and may spontaneously regress. If surgery is required, these eyes respond to vitrectomy procedures with segmentation of sea fan proliferation. Neither scleral buckling nor panretinal photocoagulation (nor feeder vessel laser) is necessary for good outcomes.
References
Clarkson JG . The ocular manifestations of sickle-cell disease: a prevalence and natural history study. Trans Am Ophthalmol Soc 1992; 90: 481–504.
Welch RB, Goldberg MF . Sickle-cell hemoglobin and its relation to fundus abnormality. Arch Ophthalmol 1966; 75: 353–362.
Downes SM, Hambleton IR, Chuang EL, Lois N, Serjeant GR, Bird AC . Incidence and natural history of proliferative sickle cell retinopathy: observations from a cohort study. Ophthalmology 2005; 112: 1869–1875.
Brazier DJ, Gregor ZJ, Blach RK, Porter JB, Huehns ER . Retinal detachment in patients with proliferative sickle cell retinopathy. Trans Ophthalmol Soc UK 1986; 105 (Part 1): 100–105.
Treister G, Machemer R . Results of vitrectomy for rare proliferative and hemorrhagic diseases. Am J Ophthalmol 1977; 84: 394–412.
Ryan SJ . Role of the vitreous in the haemoglobinopathies. Trans Ophthalmol Soc UK 1975; 95: 403–406.
Morgan CM, D'Amico DJ . Vitrectomy surgery in proliferative sickle retinopathy. Am J Ophthalmol 1987; 104: 133–138.
Pulido JS, Flynn Jr HW, Clarkson JG, Blankenship GW . Pars plana vitrectomy in the management of complications of proliferative sickle retinopathy. Arch Ophthalmol 1988; 106: 1553–1557.
Jampol LM, Farber M, Rabb MF, Serjeant G . An update on techniques of photocoagulation treatment of proliferative sickle cell retinopathy. Eye 1991; 5 (Part 2): 260–263.
Kimmel AS, Magargal LE, Stephens RF, Cruess AF . Peripheral circumferential retinal scatter photocoagulation for the treatment of proliferative sickle retinopathy. An update. Ophthalmology 1986; 93: 1429–1434.
Goldbaum MH, Peyman GA, Nagpal KC, Goldberg MF, Asdourian GK . Vitrectomy in sickling retinopathy: report of five cases. Ophthalmic Surg 1976; 7: 92–102.
Cohen SB, Fletcher ME, Goldberg MF, Jednock NJ . Diagnosis and management of ocular complications of sickle hemoglobinopathies: Part V. Ophthalmic Surg 1986; 17: 369–374.
Fox PD, Minninger K, Forshaw ML, Vessey SJ, Morris JS, Serjeant GR . Laser photocoagulation for proliferative retinopathy in sickle haemoglobin C disease. Eye 1993; 7 (Part 5): 703–706.
Condon PI, Serjeant GR . Behaviour of untreated proliferative sickle retinopathy. Br J Ophthalmol 1980; 64: 404–411.
Condon P, Jampol LM, Farber MD, Rabb M, Serjeant G . A randomized clinical trial of feeder vessel photocoagulation of proliferative sickle cell retinopathy. II. Update and analysis of risk factors. Ophthalmology 1984; 91: 1496–1498.
Jampol LM, Goldberg MF . Retinal breaks after photocoagulation of proliferative sickle cell retinopathy. Arch Ophthalmol 1980; 98: 676–679.
Durant WJ, Jampol LM, Daily M . Exudative retinal detachment in hemoglobin SC disease. Retina 1982; 2: 152–154.
Jampol LM, Green Jr JL, Goldberg MF, Peyman GA . An update on vitrectomy surgery and retinal detachment repair in sickle cell disease. Arch Ophthalmol 1982; 100: 591–593.
Goldberg MF . Retinal neovascularization in sickle cell retinopathy. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol 1977; 83: OP409–OP431.
Holekamp NM, Shui YB, Beebe D . Lower intraocular oxygen tension in diabetic patients: possible contribution to decreased incidence of nuclear sclerotic cataract. Am J Ophthalmol 2006; 141: 1027–1032.
Acknowledgements
We thank THW and RR for the design and conduct of the study; THW, RR, DAHL, and BM for the collection, management, analysis, and interpretation of the data; and also thank THW and BM for the preparation, review, or approval of the manuscript.
The study conformed to the declaration of Helsinki.
Author information
Authors and Affiliations
Corresponding author
Additional information
Financial Disclosures: None
Funding Support: None
Rights and permissions
About this article
Cite this article
Williamson, T., Rajput, R., Laidlaw, D. et al. Vitreoretinal management of the complications of sickle cell retinopathy by observation or pars plana vitrectomy. Eye 23, 1314–1320 (2009). https://doi.org/10.1038/eye.2008.296
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2008.296
Keywords
This article is cited by
-
Proliferative Sickle Cell Retinopathy: A Patient and a Physician’s Perspective on Quality of Life and Quality of Eye Care
Ophthalmology and Therapy (2024)
-
Action on sickle cell retinopathy: the time is now
Eye (2022)
-
Makulopathie bei Sichelzellerkrankung
Der Ophthalmologe (2021)
-
Sickle cell retinopathy. A focused review
Graefe's Archive for Clinical and Experimental Ophthalmology (2019)
