
Abstract
Plasma aldosterone concentrations (PACs) are often increased in the advanced stages of chronic kidney disease (CKD); however, PAC has not been fully investigated in early CKD. Moreover, little is known about the relationship between aldosteronemia and left ventricular (LV) mass in subjects with mild-to-moderate CKD. The study objectives were to analyze PAC, LV mass (LVM), LV geometry and their relationships, in a group of hypertensive patients with stage I–III CKD. One hundred ninety-five hypertensive patients with stage I–III CKD were enrolled and compared with a control group of 82 hypertensive patients without renal dysfunction. LVM was higher in subjects with CKD than in the control group and increased progressively with advancing stages of CKD (P=0.004). A similar trend was observed for PAC (P<0.0001), in which PAC was greater in CKD subjects with LV concentric geometry than in those with eccentric LV hypertrophy (P=0.01). Furthermore, in CKD patients, PAC was directly and significantly correlated with LVM (r=0.29; P<0.0001) and with relative wall thickness (RWT; r=0.36; P<0.0001). These associations remained significant even after adjustment for various confounding factors in multiple regression analyses (P<0.001). In summary, the results demonstrated that in CKD hypertensive patients, LVM, RWT and PAC are increased and related to each other from the earliest stages of renal dysfunction. Furthermore, it seems biologically plausible to speculate that aldosterone may promote a concentric geometry of the left ventricle and increase LVM in hypertensive patients with early CKD.
Similar content being viewed by others

Introduction
Since the earliest stages, chronic kidney disease (CKD) is associated with a high risk of premature cardiovascular (CV) death and morbidity1, 2 and may lead to increased medical expenditures.3 Although people with end-stage renal disease (ESRD) are at the highest risk of CV diseases, there will likely be more events in subjects with early-stage CKD owing to increased prevalence.1, 2 Pathological left ventricular hypertrophy (LVH) is particularly common in CKD patients.4, 5, 6, 7 The association between kidney injury and increased left ventricular (LV) mass occurs so early that a direct relation between subclinical renal damage (that is, the percentage of global glomerulosclerosis) and LV mass (LVM) may be observed in kidney donors with normal renal function.7 Increased LVM is a proven independent predictor of CV events.6, 8 It has also been suggested that assessment of LV geometry may add prognostic information in hypertensive patients beyond assessment of LVM alone, because concentric remodeling, as well as eccentric and concentric LVH patterns, increases the risk of CV disease when compared with normal geometry, being concentric hypertrophy the condition that most markedly raises the risk.8 Therefore, exploring LVM and LV geometry and their correlates in early CKD may improve understanding of why increased CV risk is observed in subjects in the first stages of CKD.
Plasma aldosterone concentrations (PACs) often increase in subjects with CKD, especially in those with ESRD.9, 10, 11, 12, 13, 14 Limited information is available on aldosterone levels in early CKD. Sound evidence indicates that aldosterone has a fundamental role in determining functional and structural changes in the heart.14, 15 Moreover, it has been observed that higher PACs are related to resistant hypertension16 and are independently associated with the development of congestive heart failure17 and with CV mortality among the subjects with CKD.18 However, previous studies on the association between LVM and LV geometry and circulating aldosterone levels in subjects without primary aldosteronism yielded conflicting results.19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29 Little is known regarding the relationships between aldosteronemia and LVM in subjects with mild-to-moderate CKD.
The study objectives were to analyze PAC, LVM and LV geometry and their relationships in hypertensive patients with stage I–III CKD and compare them with a control group of hypertensive patients without renal dysfunction.
Methods
The study population was selected from the hypertensive patients consecutively attending our hypertension center.
Exclusion criteria were:
-
Age <18 years and >70 years
-
Known diabetes or fasting glycaemia ⩾126 mg dl−1
-
Renovascular, malignant, endocrine hypertension or hypertension associated with obstructive sleep apnea syndrome
-
Known proteinuria and hematuria
-
Estimated glomerular filtration rate (eGFR)<30 ml min−1 per 1.73 m2
-
Previous known nephritic diseases and hereditary renal diseases
-
Heart failure
-
Positive history or clinical signs of ischemic heart disease
-
Positive history or clinical signs of cerebrovascular diseases
-
Major non-cardiovascular diseases
-
Unreliable 24-h urine collection.
Endocrine and renovascular hypertension were ruled out by clinical examination and determination of serum electrolytes, plasma renin activity and plasma aldosterone, and where appropriate, by determining the plasma catecholamine levels and performing renal echography, echo Doppler of renal arteries and renoscintigraphy. To screen for obstructive sleep apnea, we used the Berlin questionnaire and the Epworth Sleepiness Scale, followed by polysomnography when appropriate.30
Primary aldosteronism was excluded on the basis of an aldosterone/renin ratio (ARR) >40. For ARR calculation, the plasma renin activity (PRA) values <0.2 ng ml−1 h−1 were arbitrarily set to 0.2, in line with the PAPY (Primary Aldosteronism Prevalence in Hypertensives) study.31
Written informed consent was obtained from each patient. The study protocol conformed to the ethical guidelines of the Declaration of Helsinki and was approved by the local review board.
Study design
In patients previously treated for hypertension pharmacologically, treatment was withdrawn for at least 2 weeks. No subject was taking aldosterone antagonists. Patients whose blood pressure (BP) increased to >180/110 mm Hg during the washout period were not enrolled. Clinic BP was recorded in a sitting position by a doctor and was considered as the average of three consecutive measurements obtained by a sphygmomanometer after 5 min of rest. Furthermore, an echocardiographic study and 24-h ambulatory BP monitoring were carried out. In addition, a 24-h urine sample was collected to evaluate albumin excretion rate (AER) and electrolyte excretion. The following morning, after an overnight fast of at least 10 h and after 1 h in the supine position, blood samples were drawn to perform routine blood chemistry and to assay PRA and PAC. All subjects were instructed to ingest a diet containing 130–140 mmol per day sodium and 40–50 mmol per day potassium before the biochemical evaluation.
Measurements
Routine biochemical parameter determination was performed with standard techniques using an autoanalyzer (Boehringer Mannheim for Hitachi system 911, Mannheim, Germany). Low-density lipoprotein cholesterol was calculated by the Friedwald formula. The 24-h AER was assayed by a solid-phase enzyme immunoassay (Microalbumin-ELISA, DRG Diagnostics, Marburg, Germany).
eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration equation.32 The classification proposed by the Kidney Disease: Improving Global Outcomes 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease was used to define the first three stages of renal function impairment.2 The stages of CKD were defined as follows: stage I, eGFR >90 ml min−1 per 1.73 m2 and 24-h AER >20 μg min−1; stage II, eGFR of 60–89 ml min−1 per 1.73 m2 and 24-h AER >20 μg min−1; stage III, eGFR of 30 to 59 ml min−1 per 1.73 m2.2
Plasma renin activity and PAC were measured by radioimmunoassay with commercially available kits (RENCTK for the former and ALDCTK-2 for the latter), both purchased from Sorin Biomedica Diagnostics (Saluggia, Italy). The normal range of PAC in supine position and on a normal sodium diet was 7.5–15 ng dl−1. Within-assay and between-assay coefficients of variation were 5.3% and 7%, respectively.
A portable, non-invasive SpaceLabs 90207 recorder (Redmond, WA, USA) performed the 24-h ambulatory BP monitoring. M-mode echocardiography, guided by two-dimensional echocardiography, was performed in line with the American Society of Echocardiography (ASE) recommendations33 by a single cardiologist who was unaware of the patient’s clinical characteristics, using an Acuson Sequoia 512 (Siemens Mountain View, Mountain View, CA, USA).
Myocardial relative wall thickness (RWT) was calculated as twice the posterior wall thickness in diastole divided by the internal diameter and was used as an estimate of LV geometry.8, 33 Left ventricular mass was determined using the ASE-corrected cube formula.33 It was indexed by both body surface area (LVMI) and by height elevated by a power of 2.7 (LVMH2.7), as suggested by de Simone et al.,34 to provide a more stringent allowance for obesity. The mean intra-observer variability for LVM was 8.6%. LVH was defined as LVMH2.7 ⩾51 g m−2.7 in both sexes,34 and as LVMI >95 g m−2 for women and >115 g m−2 for men, as suggested by the 2013 guidelines of the European Society of Hypertension.8 LVH was classified as concentric in the presence of an RWT >42% and as eccentric with an RWT ⩽42%.4, 30 Left ventricular concentric remodeling was diagnosed in the presence of an RWT >42% and of a normal LVM.8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33 This classification was performed twice, using both of the aforementioned criteria to define LVH.
Statistics
We included 195 patients with hypertensive CKD in the study. As a control, we selected 82 essential hypertensive patients without renal dysfunction (eGFR >60 ml min−1 per 1.73 m2 and albuminuria <20 μg min−1), comparable for age (45.6±12.3 vs. 44.1±12.8 years) and sex (males 61% vs. 60%) with the overall population of CKD subjects. Continuous variables with a Gaussian distribution were given as means±s.d. The assumption of satisfactory normal distribution was not met for the following variables: duration of hypertension, AER, triglycerides, plasma aldosterone and PRA. For their skewed distribution, these parameters were expressed as the median and interquartile range and were log-transformed before starting the statistical tests. Differences between the groups for continuous variables were evaluated using the independent sample Student’s t-test for continuous variables. When more than two groups were compared (patients without CKD and patients with CKD divided in three stages of increasing severity), we performed one-way analysis of variance, and this was followed by the Holm–Sidak test for multiple comparisons if the overall F-test was significant. Adjustment for age was carried out by analysis of covariance. Proportional differences between the groups were assessed using a χ2-test.
Univariate associations between PAC, LVM and RWT, and between these parameters and other variables, were assessed by simple linear regression analyses and Pearson correlation coefficients. Partial correlation coefficients were also calculated to take into account the potential influence of age on the relationships of (Log) aldosterone with RWT, LVMI or LVMH2.7. Multiple stepwise linear regression analyses were used in the group with CKD to assess the independent correlates of left ventricular mass or RWT, including as the dependent variable alternatively LVMI, LVMH2.7 or RWT. Age, sex, and those parameters significantly associated with PAC, LVM or RWT in univariate analyses were included as explanatory variables. The potential influence of gender and of previous antihypertensive drug therapy on the relationships between aldosterone and cardiac structure was tested by including in the multivariate models the multiplicative two-way interaction terms ‘gender x (Log) PAC’ and ‘previous therapy x (Log) PAC’. A two-tailed P<0.05 was considered statistically significant. The statistical analyses were performed using the SYSTAT DATA software package, version 12 (Systat, San Jose, CA, USA).
Results
As shown in Table 1, serum creatinine, AER, serum uric acid and waist circumference were greater and eGFR was lower in the overall population of 195 patients with CKD compared with the control group of hypertensive patients without renal dysfunction. Table 1 also lists the main clinical characteristics, serum and urinary electrolytes and PRA of the CKD patients divided according to the three stages of increasing severity. Although age was not different in the control group with normal renal function compared with the CKD patients as a whole, CKD patients belonging to stage III and those belonging to stage II were older compared with the subjects without CKD. Moreover, CKD patients of the first stage were younger compared with those of stage II and stage III. Whereas PRA, serum and urinary potassium did not differ across all the four groups studied, PAC was significantly higher in the overall population of CKD subjects (11.6 (6.5–17.3) pg ml−1) when compared with the patients without CKD (8.1 (5.6–12.7) ng dl−1; P<0.0001). The Holm–Sidak test for multiple comparisons showed that in each stage of CKD, PAC was greater than in subjects without renal dysfunction. Moreover, the PAC of patients belonging to stage II was lower compared with that of stage III (Figure 1). These results were also observed when this comparison was performed in the patients never pharmacologically treated for hypertension (F=12.04; P<0.0001, before the adjustment; F=11.72; P<0.0001 after the adjustment for age). In this subset of study participants, plasma aldosterone levels were: 8.0 (5.1–12.0) ng dl−1 in the group without CKD; 9.8 (6.3–14.7) ng dl−1 in stage I CKD; 7.6 (5.9–15.7) ng dl−1 in stage II CKD; 18.0 (7.8–28.6) ng dl−1 in stage III CKD. The differences between the group with normal renal function and the three stages of CKD were all highly significant (P<0.001). As reported in Table 2, 24-h systolic (SBP) and diastolic BPs (DBP), daytime SBP and DBP, nighttime SBP and DBP, interventricular septum, posterior wall thickness, RWT, LVM, LVMI and LVMH2.7 and the prevalence of LVH, regardless of the criteria used to define it, were significantly higher in subjects with CKD than in those without it. In the same Table, BPs, heart rate and echocardiographic parameters of the CKD patients grouped according to their level of renal function are shown. The differences among the four groups regarding RWT and LVM remained significant even after adjustment for age. Among the CKD subjects, the patients previously treated with antihypertensive drugs tended to be older (P=0.08) and had a longer duration of hypertension (P=0.03) compared with those never pharmacologically treated. All the other variables listed in Tables 1 and 2 did not differ between these two subgroups (data not shown).

Box plots showing plasma aldosterone levels in hypertensive patients with chronic kidney disease (CKD), grouped in the first three stages of the Kidney Disease: Improving Global Outcomes classification and in hypertensive subjects without CKD. In the box-and-whisker plots, the central boxes represent the values from the lower to upper quartile (25th to 75th percentile). The middle lines represent the medians. Lower and upper whiskers extend to the 5th and 95th percentiles, respectively. (1)After adjustment by analysis of covariance for age, the P-value remained highly significant (P<0.0001) *P<0.001 vs. CKD I, vs. CKD II and vs. CKD III; ^P=0.04 vs. CKD I.
The prevalence of eccentric LVH was not significantly different among the groups examined and was 16% in stage III; 18% in stage II; 15% in stage I CKD and 16% in subjects without CKD (P of overall χ2-test: 0.98) when using the criteria based on the sex-specific cut-off of LVH. Analogous results obtained when the classification of LVH was based on LVMH2.7 (P of overall χ2-test: 0.818; data not shown). In contrast, concentric LVH was more common in subjects with CKD (36% in stage III; 26% in stage II; 23% in stage I) than in those with normal renal function (10%; P of overall χ2-test: 0.01; P=0.001 stage III vs. no CKD; P=0.006 stage II vs. no CKD; P=0.017 stage I vs. no CKD). This finding, obtained when LVM was indexed for body surface area, was replicated by indexing LVM for height2.7 (P of overall χ2 test: 0.02).
The CKD patients with LVMH2.7 ⩾51 g m−2.7 (n=89) had greater levels of plasma aldosterone than those with lower values of LVMH2.7 (n=106) (12.7 (8.1–19.4) vs. 9.8 (6–15.2) ng dl−1). Similarly, subjects with LVH (n=82) defined on the basis of the sex-specific cutoffs of LVMI had higher levels of PAC than those without it (n=113; 12.7 (7.7–19.8) vs. 10 (6.1–15) ng dl−1; P=0.004). This was also true considering only the CKD patients never treated for hypertension. In this subset of patients, by using the criteria based on LVM indexed for body surface area , PAC was 12.5 (7.1–18.7) ng dl−1 in the subgroup with LVH (n=33) and 7.6 (6.0–14.7) ng dl−1 in that without it (n=62; P=0.017). Similar findings were observed when using the classification based on LVMH2.7 (P=0.019).
Pooling together all the CKD subjects with LV concentric geometry (patients with concentric LVH and those with concentric remodeling of LV without LVH), we observed higher PAC (14.7 (9.6–20.9) ng dl−1) in this subgroup (n=69) than in patients with eccentric LVH (n=38; 10.6 (7.4–15.7) ng dl−1; P=0.013). These results, which were obtained by using the limit of 51 g m−2.7 to detect LVH, were confirmed when the classification of LVH was based on the sex-specific cutoffs of LVMI (Figure 2).

Box plots comparing plasma aldosterone concentration in chronic kidney disease patients with eccentric left ventricular (LV) hypertrophy, defined by the presence of a value of LV mass indexed for body surface area (LVMI) >95 g m−2 for women and >115 g m−2 for men, and a myocardial relative wall thickness (RWT) ⩽42%, and in those with a concentric geometry of the left ventricle, defined by a RWT >42% regardless of the value of LVMI. In the box-and-whisker plots, the central boxes represent the values from the lower to upper quartile (25th to 75th percentile). The middle lines represent the medians. Lower and upper whiskers extend to the 5th and 95th percentiles, respectively.
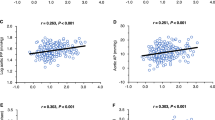
The univariate correlations of PAC, LVMI, LVMH2.7 and RWT with other variables in the overall group of CKD patients are displayed in Table 3. Highly significant correlations were observed between PAC and LVMI (Figure 3), between PAC and LVMH2.7 and, even more closely, between PAC and RWT. As reported at the bottom of Table 3, the correlations of PAC with LVMH2.7, LVMI and RWT held even after adjustment for age and were also significant in the CKD patients never treated, as well as in those previously treated with antihypertensive drugs. The relationships of PAC with LVMI (β=0.256, P<0.001), LVMH2.7 (β=0.231, P=0.001) and RWT (β=0.312, P<0.001) in the group with CKD remained statistically significant in stepwise multiple regression models in which LVMI, LVMH2.7 and RWT were considered alternatively as dependent variables. In addition to PAC, LVMI, LVMH2.7 and RWT were independently associated with nighttime systolic BP (all P<0.001); LVMI and LVMH2.7 with (Log) AER (P=0.014 and P=0.001, respectively); and only LVMH2.7 with body mass index (P=0.026). The multiplicative two-way interaction terms ‘gender x (Log) PAC’ and ‘previous therapy x (Log) PAC’, which were introduced into the multiple regression models to assess the influence of sex and previous antihypertensive treatment on the association between PAC and LVM and LV geometry, did not show statistical significance. These results did not change substantially when nighttime BPs were replaced by clinic BPs and body mass index was replaced by waist circumference in the multivariate models.

Scattergram showing the relationship between plasma aldosterone (transformed as a logarithm owing to its skewed distribution) and left ventricular mass indexed for body surface area in hypertensive patients with chronic kidney disease (CKD). Circles represent stage I CKD patients; squares represent stage II CKD patients; diamonds represent stage III CKD patients. Dashed hyperbolic lines represent the 95% confidence bands around the regression line.
Discussion
The main results of the present study are:
-
1)
The demonstration of higher levels of plasma aldosterone in early-stage CKD patients with primary hypertension compared with hypertensive patients with normal renal function.
-
2)
The evidence of a direct and independent association of PAC with LVM and with a concentric remodeling of the LV in patients with CKD.
There is an extensive body of evidence from clinical and experimental studies showing that advanced stages of renal diseases are characterized, with few exceptions, by elevations in mineralocorticoid activity, mainly owing to hyperkalemia and to inappropriate activation of the renin–angiotensin system.9, 10, 11, 12, 13, 14 Indeed, aldosterone levels may also be normal9 or decreased.35, 36 This variability may be related to differences in the serum concentrations of potassium and in PRA. Indeed, in patients with CKD with hyporeninemia and hyperkalemia, plasma aldosterone levels are low, and these patients have the hyporeninemic hypoaldosteronism syndrome.35, 36 The behavior of PAC in subjects with minor degrees of renal function impairment has been less investigated.
Our results seem to suggest that PAC may be increased also in the early stages of renal dysfunction, especially in subjects belonging to stage III of the Kidney Disease: Improving Global Outcomes classification, even without elevations in PRA and serum potassium levels.
Our findings are partially in agreement with previous reports. Hene et al.13 described elevations in plasma aldosterone levels among patients with stable, chronic renal insufficiency. In their cross-sectional analysis, PAC increased when creatinine clearance was less than approximately 70 ml min−1, even with normal serum potassium and normal PRA. Aldosterone levels were greatest among patients with the greatest impairment in renal function.13
Data more recently obtained in The Ludwigshafen Risk and Cardiovascular Health (LURIC) study,18 a prospective investigation including 3153 patients free of primary kidney disease at baseline and referred for coronary angiography, appear to be in line with the present study. The LURIC study showed that PAC was progressively higher across decreasing eGFR tertiles.18 On the other hand, in animal models of kidney disease, elevated aldosterone levels and adrenal hypertrophy precede the development of hypertension, proteinuria and glomerulosclerosis.14
Putative factors that may explain the increased PAC observed in patients with stage I–III CKD may be slightly augmented levels of parathyroid hormone, which may be found in the early phases of CKD,37 or endothelin-1, a modulator of aldosterone production and secretion, which is implicated in the development and progression of CKD.38, 39 Our study revealed also that PAC was higher in CKD subjects with LVH than in those without it. This result was driven by the close association we found between PAC and the concentric remodeling of the LV. Indeed, plasma aldosterone levels were not different between subjects with or without eccentric hypertrophy. In contrast, patients with eccentric LVH showed lower PAC than subjects with a concentric geometric pattern, including study participants with concentric LVH and those with concentric LV remodeling without LVH. Moreover, PAC was correlated positively, and independently of BP and other potential confounders, with LVM, regardless of the method of indexation used. A close relationship was found between PAC and the index of LV geometry, that is, myocardial RWT. This was true in CKD patients previously treated with antihypertensive drugs, as well as in those never treated. Moreover, in linear multiple regression analyses, the multiplicative two-way interaction term ‘previous therapy x (Log) PAC’ was not significantly associated with either LVM or RWT. Therefore, if a residual influence of the previous antihypertensive therapy on the parameters we explored exists, it has a negligible effect on the relationships between plasma aldosterone and LVH and geometry.
LVH is very frequent among CKD patients.4, 5, 6 It is a complex process driven by the responses of the cardiomyocytic and the noncardiomyocytic components of the heart to hemodynamic (pressure or volume overload), genetic and humoral stimuli. It is well known that pressure overload results in concentric hypertrophy, whereas volume overload leads to eccentric hypertrophy.6 In our study, concentric LVH was more frequent in subjects with CKD than in those without it. However, both the patterns of geometric remodeling of the LV and a mixed pattern characterized by the increase of both diameters and wall thicknesses can often be recognized in more advanced stages of CKD and in ESRD.4, 6
Aldosterone can influence LV remodeling by altering cardiac loading conditions through its effects on renal sodium and water retention and augmented conduit artery stiffness and via direct effects on the cardiac extracellular matrix.14, 15 Mineralocorticoid receptors are present in the human heart and chronic administration of aldosterone in animal models leads to cardiac fibrosis and LVH. Moreover, subjects with primary aldosteronism have early and more severe development of LVH when compared with subjects with essential hypertension. These data would suggest a BP-independent effect of aldosterone on the heart.15 However, previous literature on the association between LVM and circulating aldosterone levels in subjects without primary aldosteronism yielded conflicting results.19, 20, 21, 22, 23, 24 Similar inconsistent findings have been reported on the association of PAC with LV geometry.22, 25, 26, 27, 28, 29 In some of these investigations, an association of plasma aldosterone with RWT has been found only in women. Our results are not in agreement with the studies reporting sex-related differences in the influence of aldosterone on LV remodeling, because we did not observe modification of the relations of PAC to LVM and LV geometry by gender (all the P-values for the interaction term ‘gender x (Log) PAC’ exceeded 0.05) The discrepancies between these studies could be owing to the heterogeneity of study populations, that is, general vs. hypertensive populations or differences in dietary salt intake, ethnicity, gender distribution or sample size, to incomplete adjustment for confounders or to concomitant therapy with drugs that could alter the renin–angiotensin–aldosterone system.
To the best of our knowledge, the present study is the first exploring this issue in patients with early CKD. Sato et al.24 analyzed the association between cardiac hypertrophy and aldosterone in 29 patients (18 patients with nondiabetic nephropathy and 11 patients with diabetic nephropathy) with ESRD treated with hemodialysis. They observed a significant and BP-independent correlation in nondiabetic patients.
More recently, Edwards et al.40 provided an indirect evidence of aldosterone involvement in the development of LVH in early-stage CKD subjects. They demonstrated a reduction of LVM in these patients after the use of spironolactone 25 mg once daily.
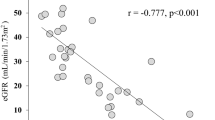
Another finding of our study deserves to be underlined. In univariate analysis, we noted a negative correlation between eGFR and LVM, which lost statistical significance in multivariate analysis, after adding aldosterone as a covariate in the multiple regression model. Therefore, one could hypothesize that the inverse association between renal function and LVM observed in early CKD in the current study and in the previous one5 may be, at least in part, mediated by aldosterone.
In conclusion, our results seem to suggest that PAC is increased in subjects with early-stage CKD. These elevated levels may help to explain the increased LVM observed in these patients and may thereby contribute toward enhancing the CV risk associated with stage I–III CKD. Although there is need for caution in interpreting the results, because of the cross-sectional design of this study, our results, along with those of Edwards et al., lead to the hypothesis that treatment with small doses of aldosterone antagonists may have potential beneficial effects in early-CKD hypertensive subjects with LVH. Additional investigations are needed to test this hypothesis.
References
Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJ, Mann JF, Matsushita K, Wen CP . Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet 2013; 382: 339–352.
Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Work Group Kidney Int Suppl 2013; 3: 1–163.
Higashiyama A, Okamura T, Watanabe M, Murakami Y, Otsuki H, Adachi N, Kaneko C, Uehara E, Okayama A, Ueshima H . Effect of chronic kidney disease on individual and population medical expenditures in the Japanese population. Hypertens Res 2009; 32: 450–454.
Nardi E, Palermo A, Mulè G, Cusimano P, Cottone S, Cerasola G . Left ventricular hypertrophy and geometry in hypertensive patients with chronic kidney disease. J Hypertens 2009; 27: 633–641.
Cerasola G, Nardi E, Mulè G, Palermo A, Cusimano P, Guarneri M, Arsena R, Giammarresi G, Foraci AC, Cottone S . Left ventricular mass in hypertensive patients with mild-to-moderate reduction of renal function. Nephrology 2010; 15: 203–210.
Cerasola G, Nardi E, Palermo A, Mulè G, Cottone S . Epidemiology and pathophysiology of left ventricular abnormalities in chronic kidney disease: a review. J Nephrol 2011; 24: 1–10.
Haruyama N, Tsuchimoto A, Masutani K, Nagata M, Kitada H, Tanaka M, Tsuruya K, Kitazono T . Subclinical nephrosclerosis is linked to left ventricular hypertrophy independent of classical atherogenic factors. Hypertens Res 2014; 37: 472–477.
Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Bhöm M, Christiaens T, Cifkova R, De Backer G, Dominiczak A, Galderisi M, Grobbee DE, Jaarsma T, Kirchhof P, Kjeldsen SE, Laurent S, Manolis AJ, Nilsson PM, Ruilope LM, Schmieder RE, Sirnes PA, Sleight P, Viigimaa M, Waeber B, Zannad F . Task Force Members. 2013 ESH/ESC Guidelines for the Management of Arterial Hypertension. The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2013; 31: 1281–1357.
Weidmann P, Maxwell MH, Lupu AN . Plasma aldosterone in terminal renal failure. Ann Intern Med 1973; 78: 13–18.
Saruta T, Nagahama S, Eguchi T, Oka M, Kambegawa A . Renin, aldosterone, and other mineralocorticoids in hyperkalemic patients with chronic renal failure showing mild azotemia. Nephron 1981; 29: 128–132.
Weidmann P, Maxwell MH, Rowe P, Winer R, Massry SG . Role of the renin–angiotensin–aldosterone system in the regulation of plasma potassium in chronic renal disease. Nephron 1975; 15: 35–49.
Berl T, Katz FH, Henrich WL, de Torrente A, Schrier RW . Role of aldosterone in the control of sodium excretion in patients with advanced chronic renal failure. Kidney Int 1978; 14: 228–235.
Hene RJ, Boer P, Koomans HA, Mees EJ . Plasma aldosterone concentrations in chronic renal disease. Kidney Int 1982; 21: 98–101.
Hostetter TH, Ibrahim HN . Aldosterone in chronic kidney and cardiac disease. J Am Soc Nephrol 2003; 14: 2395–2401.
Catena C, Colussi G, Marzano L, Sechi LA . Aldosterone and the heart: from basic research to clinical evidence. Horm Metab Res 2012; 44: 181–187.
deFaria AP, Demacq C, Figuiredo VN, Moraes CH, Santos RC, Sabbatini AR, Barbaro NR, Boer-Martins L, Fontana V, Moreno H Jr . Hypoadiponectinemia and aldosterone excess are associated with lack of blood pressure control in subjects with resistant hypertension. Hypertens Res 2013; 36: 1067–1072.
Deo R, Yang W, Khan M, Bansal N, Zhang X, Leonard MB, Keane MG, Soliman EZ, Steigerwalt S, Townsend RR, Shlipak MG, Feldman HI . CRIC Study Investigators. Serum aldosterone and death, end-stage renal disease, and cardiovascular events in Blacks and Whites. Findings from The Chronic Renal Insuffuciency Cohort (CRIC) Study. Hypertension 2014; 64: 103–110.
Tomaschitz A, Pilz S, Ritz E, Grammer T, Drechsler C, Boehm BO, März W . Association of plasma aldosterone with cardiovascular mortality in patients with low estimated GFR: the Ludwigshafen Risk and Cardiovascular Health (LURIC) Study. Am J Kidney Dis 2011; 57: 403–414.
Duprez DA, Bauwens FR, De Buyzere ML, De Backer TL, Kaufman JM, Van Hoecke J, Vermeulen A, Clement DL . Influence of arterial blood pressure and aldosterone on left ventricular hypertrophy in moderate essential hypertension. Am J Cardiol 1993; 71: 17A–20A.
Schroeder AP, Sihm I, Morn B, Thygesen K, Pedersen EB, Lederballe O . Influence of humoral and neurohormonal factors on cardiovascular hypertrophy in untreated essential hypertensives. Am J Hypertens 1996; 9: 207–215.
Malmqvist K, Ohman KP, Lind L, Nystrom F, Kahan T . Relationships between left ventricular mass and the renin–angiotensin system, catecholamines, insulin and leptin. J Intern Med 2002; 252: 430–439.
Vasan RS, Evans JC, Benjamin EJ, Levy D, Larson MG, Sundstrom J, Murabito JM, Sam F, Colucci WS, Wilson PWF . Relations of serum aldosterone to cardiac structure: gender-related differences in the Framingham Heart study. Hypertension 2004; 43: 957–962.
Mulè G, Nardi E, Cusimano P, Cottone S, Seddio G, Geraci C, Palermo A, Andronico G, Cerasola G . Plasma aldosterone and its relationships with left ventricular mass in essential hypertensive patients with the metabolic syndrome. Am J Hypertens 2008; 21: 1055–1061.
Sato A, Funder JW, Saruta T . Involvement of aldosterone in left ventricular hypertrophy of patients with end-stage renal failure treated with hemodialysis. Am J Hypertens 1999; 12: 867–873.
Schunkert H, Hense HW, Muscholl M, Luchner A, Kurzinger S, Danser AH, Riegger GA . Associations between circulating components of the renin-angiotensin-aldosterone system and left ventricular mass. Heart 1997; 77: 24–31.
Shigematsu Y, Hamada M, Mukai M, Matsuoka H, Sumimoto T, Hiwada K . Clinical evidence for an association between left ventricular geometric adaptation and extracardiac target organ damage in essential hypertension. J Hypertens 1995; 13: 155–160.
Soylu A, Temizhan A, Duzenli MA, Sokmen G, Koylu O, Telli HH . The influence of aldosterone on the development of left ventricular geometry and hypertrophy in patients with essential hypertension. Jpn Heart J 2004; 45: 807–821.
Iwashima Y, Horio T, Kuroda S, Takishita S, Kawano Y . Influence of plasma aldosterone on left ventricular geometry and diastolic function in treated essential hypertension. Hypertens Res 2002; 25: 49–56.
Edelmann F, Tomaschitz A, Wachter R, Gelbrich G, Knoke M, Dungen HD, Pilz S, Binder L, Stahrenberg R, Schmidt A, März W, Pieske B . Serum aldosterone and its relationship to left ventricular structure and geometry in patients with preserved left ventricular ejection fraction. Eur Heart J 2012; 33: 203–212.
Parati G, Lombardi C, Hedner J, Bonsignore MR, Grote L, Tkacova R, Lévy P, Riha R, Bassetti C, Narkiewicz K, Mancia G, McNicholas WT . EU COST Action B26 members. Recommendations for the management of patients with obstructive sleep apnoea and hypertension. Eur Respir J 2013; 41: 523–538.
Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C, Ganzaroli C, Giacchetti G, Letizia C, Maccario M, Mallamaci F, Mannelli M, Mattarello MJ, Moretti A, Palumbo G, Parenti G, Porteri E, Semplicini A, Rizzoni D, Rossi E, Boscaro M, Pessina AC, Mantero F . PAPY Study Investigators. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol 2006; 48: 2293–2300.
Levey A, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J . CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med 2009; 150: 604–612.
Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise J, Solomon S, Spencer KT St, John Sutton M, Stewart W . American Society of Echocardiography's Nomenclature and Standards Committee; Task Force on Chamber Quantification; American College of Cardiology Echocardiography Committee; American Heart Association; European Association of Echocardiography, European Society of Cardiology. Recommendations for chamber quantification. Eur J Echocardiography 2006; 7: 79–108.
de Simone G, Daniels SR, Devereux RB, Meyer RA, Roman MJ, de Divitiis O, Alderman MH . Left ventricular mass and body size in normotensive children and adults: assessment of allometric relations and the impact of overweight. J Am Coll Cardiol 1992; 20: 1251–1260.
DeFronzo RA . Hyperkalemia and hyporeninemic hypoaldosteronism. Kidney Int 1980; 17: 118–134.
Schambelan M, Sebastian A, Biglieri E . Prevalence pathogenesis, and functional significance of aldosterone deficiency in hyperkalemic patients with chronic renal insufficiency. Kidney Int 1980; 17: 89–101.
Tomaschitz A, Ritz E, Pieske B, Fahrleitner-Pammer A, Kienreich K, Horina JH, Drechsler C, Marz W, Ofner M, Pieber TR, Pilz S . Aldosterone and parathyroid hormone: a precarious couple for cardiovascular disease. Cardiovasc Res 2012; 94: 10–19.
Rossi GP, Albertin G, Neri G, Andreis PG, Hofmann S, Pessina AC, Nussdorfer GG . Endothelin-1 stimulates steroid secretion of human adrenocortical cells ex vivo via both ETA and ETB receptor subtypes. J Clin Endocrinol Metab 1997; 82: 3445–3449.
Cottone S, Mulè G, Guarneri M, Palermo A, Lorito M, Riccobene R, Palermo A, Lorito MC, Riccobene R, Arsena R, Vaccaro F, Vadalà A, Nardi E, Cusimano P, Cerasola G . Endothelin-1 and F2-isoprostane relate to and predict renal dysfunction in hypertensive patients. Nephrol Dial Transplant 2009; 24: 497–503.
Edwards NC, Steeds RP, Stewart PM, Ferro CJ, Townend JN . Effect of spironolactone on left ventricular mass and aortic stiffness in early stage chronic kidney disease. J Am Coll Cardiol 2009; 54: 505–512.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mulè, G., Nardi, E., Guarino, L. et al. Plasma aldosterone and its relationship with left ventricular mass in hypertensive patients with early-stage chronic kidney disease. Hypertens Res 38, 276–283 (2015). https://doi.org/10.1038/hr.2014.171
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2014.171
Keywords
This article is cited by
-
Association between early-stage chronic kidney disease and reduced choroidal thickness in essential hypertensive patients
Hypertension Research (2019)
-
Is echocardiography mandatory for patients with chronic kidney disease?
Internal and Emergency Medicine (2019)
-
Cardiac hypertrophy in chronic kidney disease—role of Aldosterone and FGF23
Renal Replacement Therapy (2018)
-
Comparison of left ventricular structure and function in primary aldosteronism and essential hypertension by echocardiography
Hypertension Research (2017)
-
Advanced glycation of high-density lipoprotein and the functionality of aldosterone release in type 2 diabetes
Hypertension Research (2017)
