
Abstract
Rectal bleeding and faecal incontinence are serious injuries that men with prostate cancer who receive radiotherapy can experience. Although technical advances—including the use of intensity-modulated radiotherapy coupled with image-guided radiotherapy—have enabled the delivery of dose distributions that conform to the shape of the tumour target with steep dose gradients that reduce the dose given to surrounding tissues, radiotherapy-associated toxicity can not be avoided completely. Many large-scale prospective studies have analysed the correlations of patient-related and treatment-related parameters with acute and late toxicity to optimize patient selection and treatment planning. The careful application of dose–volume constraints and the tuning of these constraints to the individual patient's characteristics are now considered the most effective ways of reducing rectal morbidity. Additionally, the use of endorectal balloons (to reduce the margins between the clinical target volume and planning target volume) and the insertion of tissue spacers into the region between the prostate and anterior rectal wall have been investigated as means to further reduce late rectal injury. Finally, some drugs and other compounds are also being considered to help protect healthy tissue. Overall, a number of approaches exist that must be fully explored in large prospective trials to address the important issue of rectal toxicity in prostate cancer radiotherapy.
Key Points
-
Understanding the dose–volume effects involved in rectal injury following pelvic radiotherapy has enabled the development of toxicity models to guide treatment optimization towards favourable dose distributions in the rectum and anal canal
-
Intensity-modulated radiotherapy and image-guided radiotherapy are powerful tools to shape doses and reduce margins between the clinical target volume and planning target volume, reducing normal tissue volumes in the high-dose regions and, consequently, toxicity
-
Endorectal balloons can reduce intrafraction motion and tissue spacers can move the rectum away from the high-dose regions; these tools are beneficial when using external-beam radiotherapy with high doses per fraction
-
Some studies have confirmed that certain patients are remarkably radiosensitive; consequently, clinicians should be particularly vigilant towards patients with predisposing risk factors for rectal toxicity
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
Bhide, S. A. & Nutting, C. M. Recent advances in radiotherapy. BMC Med. 8, 25 (2010).
Bauman, G., Rumble, R. B., Chen, J., Loblaw, A. & Warde, P. Members of the IMRT Indications Expert Panel. Intensity-modulated radiotherapy in the treatment of prostate cancer. Clin. Oncol. (R. Coll. Radiol.) 24, 461–473 (2012).
Diez, P., Vogelius, I. S. & Bentzen, S. M. A new method for synthesizing radiation dose-response data from multiple trials applied to prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 77, 1066–1071 (2010).
Valdagni, R. et al. Increasing the risk of late rectal bleeding after high-dose radiotherapy for prostate cancer: the case of previous abdominal surgery. Results from a prospective trial. Radiother. Oncol. 103, 252–255 (2012).
Cesaretti, J. A. et al. ATM sequence variants are predictive of adverse radiotherapy response among patients treated for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 61, 196–202 (2005).
Cesaretti, J. A. et al. A genetically determined dose-volume histogram predicts for rectal bleeding among patients treated with prostate brachytherapy. Int. J. Radiat. Oncol. Biol. Phys. 68, 1410–1416 (2007).
Peters, C. A. et al. TGFB1 single nucleotide polymorphisms are associated with adverse quality of life in prostate cancer patients treated with radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 70, 752–759 (2008).
Damaraju, S. et al. Association of DNA repair and steroid metabolism gene polymorphisms with clinical late toxicity in patients treated with conformal radiotherapy for prostate cancer. Clin. Cancer Res. 12, 2545–2554 (2006).
Burri, R. J. et al. Association of single nucleotide polymorphisms in SOD2, XRCC1 and XRCC3 with susceptibility for the development of adverse effects resulting from radiotherapy for prostate cancer. Radiat. Res. 170, 49–59 (2008).
Valdagni, R. et al. To bleed or not to bleed. A prediction based on individual gene profiling combined with dose–volume histogram shapes in prostate cancer patients undergoing three-dimensional conformal radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 74, 1431–1440 (2009).
Denham, J. W. et al. Is there more than one late radiation proctitis syndrome? Radiother. Oncol. 51, 43–53 (1999).
Peeters, S. T. et al. Acute and late complications after radiotherapy for prostate cancer: results of a multicenter randomized trial comparing 68 Gy to 78 Gy. Int. J. Radiat. Oncol. Biol. Phys. 61, 1019–1034 (2005).
Fellin, G. et al. Clinical and dosimetric predictors of late rectal toxicity after conformal radiation for localized prostate cancer: results of a large multicenter observational study. Radiother. Oncol. 93, 197–202 (2009).
Syndikus, I. et al. Late gastrointestinal toxicity after dose-escalated conformal radiotherapy for early prostate cancer: results from the UK Medical Research Council RT01 trial (ISRCTN47772397). Int. J. Radiat. Oncol. Biol. Phys. 77, 773–783 (2010).
Tucker, S. L. et al. Late rectal toxicity on RTOG 94–06: analysis using a mixture Lyman model. Int. J. Radiat. Oncol. Biol. Phys. 78, 1253–1260 (2010).
Fonteyne, V., De Neve, W., Villeirs, G., De Wagter, C. & De Meerleer, G. Late radiotherapy-induced lower intestinal toxicity (RILIT) of intensity-modulated radiotherapy for prostate cancer: the need for adapting toxicity scales and the appearance of the sigmoid colon as co-responsible organ for lower intestinal toxicity. Radiother. Oncol. 84, 156–163 (2007).
Tucker, S. L. et al. Dose–volume response analyses of late rectal bleeding after radiotherapy for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 59, 353–365 (2004).
Rancati, T. et al. Fitting late rectal bleeding data using different NTCP models: results from an Italian multi-centric study (AIROPROS0101). Radiother. Oncol. 73, 21–32 (2004).
Gulliford, S. L. et al. Parameters for the Lyman Kutcher Burman (LKB) model of Normal Tissue Complication Probability (NTCP) for specific rectal complications observed in clinical practise. Radiother. Oncol. 102, 347–351 (2012).
Fiorino, C. et al. Late fecal incontinence after high-dose radiotherapy for prostate cancer: better prediction using longitudinal definitions. Int. J. Radiat. Oncol. Biol. Phys. 83, 38–45 (2012).
Peeters, S. T. et al. Rectal bleeding, fecal incontinence, and high stool frequency after conformal radiotherapy for prostate cancer: normal tissue complication probability modeling. Int. J. Radiat. Oncol. Biol. Phys. 66, 11–19 (2006).
Valdagni, R. et al. Development of a set of nomograms to predict acute lower gastrointestinal toxicity for prostate cancer 3D-CRT. Int. J. Radiat. Oncol. Biol. Phys. 71, 1065–1073 (2008).
Valdagni, R. et al. Is it time to tailor the prediction of radio-induced toxicity in prostate cancer patients? Building the first set of nomograms for late rectal syndrome. Int. J. Radiat. Oncol. Biol. Phys. 82, 1957–1966 (2012).
Defraene, G. et al. The benefits of including clinical factors in rectal normal tissue complication probability modeling after radiotherapy for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 82, 1233–1342 (2012).
Rancati, T. et al. Inclusion of clinical risk factors into NTCP modelling of late rectal toxicity after high dose radiotherapy for prostate cancer. Radiother. Oncol. 100, 124–130 (2011).
Barnett, G. C. et al. The impact of clinical factors on the development of late radiation toxicity: results from the Medical Research Council RT01 trial (ISRCTN47772397). Clin. Oncol. (R. Coll. Radiol.) 23, 613–624 (2011).
Zelefsky, M. J. et al. Long-term outcome of high dose intensity modulated radiation therapy for patients with clinically localized prostate cancer. J. Urol. 176, 1415–1419 (2006).
Zelefsky, M. J. et al. Incidence of late rectal and urinary toxicities after three-dimensional conformal radiotherapy and intensity-modulated radiotherapy for localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 70, 1124–1129 (2008).
Cahlon, O. et al. Ultra-high dose (86.4 Gy) IMRT for localized prostate cancer: toxicity and biochemical outcomes. Int. J. Radiat. Oncol. Biol. Phys. 71, 330–337 (2008).
Kupelian, P. A., Willoughby, T. R., Reddy, C. A., Klein, E. A. & Mahadevan, A. Hypofractionated intensity-modulated radiotherapy (70 Gy at 2.5 Gy per fraction) for localized prostate cancer: Cleveland Clinic experience. Int. J. Radiat. Oncol. Biol. Phys. 68, 1424–1430 (2007).
Spratt, D. E. et al. Long-term survival and toxicity in patients treated with high-dose intensity modulated radiation therapy for localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 85, 686–692 (2013).
International Commission on Radiation Units & Measurements. Prescribing, Recording, and Reporting Photon Beam Therapy (Report 50) (Oxford University Press, 1993).
International Commission on Radiation Units & Measurements. Prescribing, Recording and Reporting Photon Beam Therapy (Report 62) (Oxford University Press, 1999).
Zelefsky, M. J. et al. Improved clinical outcomes with high-dose image guided radiotherapy compared with non-IGRT for the treatment of clinically localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 84, 125–129 (2012).
Noyes, W. R., Hosford, C. C. & Schultz, S. E. Human collagen injections to reduce rectal dose during radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 82, 1918–1922 (2012).
Prada, P. J. et al. Transperineal injection of hyaluronic acid in anterior perirectal fat to decrease rectal toxicity from radiation delivered with intensity modulated brachytherapy or EBRT for prostate cancer patients. Int. J. Radiat. Oncol. Biol. Phys. 69, 95–102 (2007).
Pinkawa, M. et al. Application of a spacer gel to optimize three-dimensional conformal and intensity modulated radiotherapy for prostate cancer. Radiother. Oncol. 100, 436–441 (2011).
Song, D. et al. A multi-institutional trial of rectal dose reduction during prostate radiotherapy via polyethyleneglycol hydrogel injection: initial results [abstract 2420]. Int. J. Radiat. Oncol. Biol. Phys. 81 (Suppl.), S412 (2011).
Jabbari, S. et al. Stereotactic body radiotherapy as monotherapy or post-external beam radiotherapy boost for prostate cancer: technique, early toxicity, and PSA response. Int. J. Radiat. Oncol. Biol. Phys. 82, 228–234 (2012).
Smeenk, R. J., Teh, B. S., Butler, E. B., van Lin, E. N. & Kaanders, J. H. Is there a role for endorectal balloons in prostate radiotherapy? A systematic review. Radiother. Oncol. 95, 277–282 (2010).
Vernia, P. et al. Topical butyrate for acute radiation proctitis: randomised, crossover trial. Lancet 356, 1232–1235 (2000).
Hille, A. et al. Sodium butyrate enemas in the treatment of acute radiation-induced proctitis in patients with prostate cancer and the impact on late proctitis. A prospective evaluation. Strahlenther. Onkol. 184, 686–692 (2008).
Ahmad, I. U. et al. Soy isoflavones in conjunction with radiation therapy in patients with prostate cancer. Nutr. Cancer 62, 996–1000 (2010).
Lam, T. J., Kuik, D. J. & Felt-Bersma, R. J. Anorectal function evaluation and predictive factors for faecal incontinence in 600 patients. Colorectal Dis. 14, 214–223 (2012).
Smeenk, R. J., Hoffmann, A. L., Hopman, W. P., van Lin, E. N. & Kaanders, J. H. Dose–effect relationships for individual pelvic floor muscles and anorectal complaints after prostate radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 83, 636–644 (2012).
Radiation Oncology Therapy Group. RTOG/EORTC late radiation morbidity scoring schema [online], (2013).
[No authors listed]. LENT SOMA scales for all anatomic sites. Int. J. Radiat. Oncol. Biol. Phys. 31, 1049–1091 (1995).
Geinitz, H. et al. Longitudinal study of intestinal symptoms and fecal continence in patients with conformal radiotherapy for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 79, 1373–1380 (2011).
Gulliford, S. L., Partridge, M., Sydes, M. R., Andreyev, J. & Dearnaley, D. P. A comparison of dose-volume constraints derived using peak and longitudinal definitions of late rectal toxicity. Radiother. Oncol. 94, 241–247 (2010).
Michalski, J. M., Gay, H., Jackson, A., Tucker, S. L. & Deasy, J. O. Radiation dose-volume effects in radiation-induced rectal injury. Int. J. Radiat. Oncol. Biol. Phys. 76 (Suppl. 3), S123–S129 (2010).
Fiorino, C., Valdagni, R., Rancati, T. & Sanguineti, G. Dose-volume effects for normal tissues in external radiotherapy: pelvis. Radiother. Oncol. 93, 153–167 (2009).
Fiorino, C. et al. Clinical and dosimetric predictors of late rectal syndrome after 3D-CRT for localized prostate cancer: preliminary results of a multicenter prospective study. Int. J. Radiat. Oncol. Biol. Phys. 70, 1130–1137 (2008).
Boersma, L. J. et al. Estimation of the incidence of late bladder and rectum complications after high-dose (70–78 GY) conformal radiotherapy for prostate cancer, using dose–volume histograms. Int. J. Radiat. Oncol. Biol. Phys. 41, 83–92 (1998).
Jackson, A. et al. Late rectal bleeding after conformal radiotherapy of prostate cancer. II. Volume effects and dose–volume histograms. Int. J. Radiat. Oncol. Biol. Phys. 49, 685–698 (2001).
Skwarchuk, M. W. et al. Late rectal toxicity after conformal radiotherapy of prostate cancer (I): multivariate analysis and dose-response. Int. J. Radiat. Oncol. Biol. Phys. 47, 103–113 (2000).
Wachter, S. et al. Rectal sequelae after conformal radiotherapy of prostate cancer: dose-volume histograms as predictive factors. Radiother. Oncol. 59, 65–70 (2001).
Zapatero, A. et al. Impact of mean rectal dose on late rectal bleeding after conformal radiotherapy for prostate cancer: dose–volume effect. Int. J. Radiat. Oncol. Biol. Phys. 59, 1343–1351 (2004).
Fiorino, C. et al. Rectal dose-volume constraints in high-dose radiotherapy of localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 57, 953–962 (2003).
Vargas, C. et al. Dose-volume analysis of predictors for chronic rectal toxicity after treatment of prostate cancer with adaptive image-guided radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 62, 1297–1308 (2005).
Shn, M. et al. Incidence of late rectal bleeding in high-dose conformal radiotherapy of prostate cancer using equivalent uniform dose-based and dose-volume-based normal tissue complication probability models. Int. J. Radiat. Oncol. Biol. Phys. 67, 1066–1073 (2007).
Gulliford, S. L. et al. Dose–volume constraints to reduce rectal side effects from prostate radiotherapy: evidence from MRC RT01 Trial ISRCTN 47772397. Int. J. Radiat. Oncol. Biol. Phys. 76, 747–754 (2010).
Mavroidis, P. et al. Dose–response relations for anal sphincter regarding fecal leakage and blood or phlegm in stools after radiotherapy for prostate cancer. Radiobiological study of 65 consecutive patients. Strahlenther. Onkol. 181, 293–306 (2005).
Fokdal, L., Honor, H., Høyer, M. & von der Maase, H. Dose–volume histograms associated to long-term colorectal functions in patients receiving pelvic radiotherapy. Radiother. Oncol. 74, 203–210 (2005).
Acosta, O. et al. 2036 POSTER Voxel based analysis of dose for prediction of urinary and rectal toxicity in prostate cancer radiotherapy [abstract]. Eur. J. Cancer 47 (Suppl. 1), S199 (2011).
Drean, G. et al. 2034 POSTER Evaluation of two registration strategies for inter-patient dose mapping in prostate radiotherapy [abstract]. Eur. J. Cancer 47 (Suppl. 1), S198 (2011).
Pinkawa, M. et al. Consequential late effects after radiotherapy for prostate cancer - a prospective longitudinal quality of life study. Radiat. Oncol. 5, 27–36 (2010).
Heemsbergen, W. D., Peeters, S. T., Koper, P. C., Hoogeman, M. S. & Lebesque, J. V. Acute and late gastrointestinal toxicity after radiotherapy in prostate cancer patients: consequential late damage. Int. J. Radiat. Oncol. Biol. Phys. 66, 3–10 (2006).
Barnett, G. C. et al. Independent validation of genes and polymorphisms reported to be associated with radiation toxicity: a prospective analysis study. Lancet Oncol. 13, 65–77 (2012).
Yorke, E. D. Modelling the effects of inhomogeneous dose distributions in normal tissues. Semin. Radiat. Oncol. 11, 197–209 (2001).
Travis, E. L. Organizational response of normal tissues to irradiation. Semin. Radiat. Oncol. 11, 184–196 (2001).
Gulliford, S. L., Webb, S., Rowbottom, C. G., Corne, D. W. & Dearnaley, D. P. Use of artificial neural networks to predict biological outcomes for patients receiving radical radiotherapy of the prostate. Radiother. Oncol. 71, 3–12 (2004).
Tomatis, S. et al. Late rectal bleeding after 3D-CRT for prostate cancer: development of a neural-network-based predictive model. Phys. Med. Biol. 57, 1399–1412 (2012).
Carrara, M. et al. Predicting late faecal incontinence after high-dose radiotherapy for prostate cancer: application of artificial neural network classification on a longitudinal definition [abstract 290]. Radiother. Oncol. 102 (Suppl. 1), S153 (2012).
Ospina, J. D. et al. Random forest versus published NTCP models for rectal toxicity prediction [abstract OC-0477]. Radiother. Oncol. 102 (Suppl. 1), S153 (2012).
Kuban, D. A. et al. Long-term results of the, M. D. Anderson randomized dose-escalation trial for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 70, 67–74 (2008).
Zietman, A. L. et al. Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: a randomized controlled trial. JAMA 294, 1233–1239 (2005).
Peeters, S. T. et al. Dose-response in radiotherapy for localized prostate cancer: results of the Dutch multicenter randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy. J. Clin. Oncol. 24, 1990–1996 (2006).
Ling, C. C. et al. Conformal radiation treatment of prostate cancer using inversely-planned intensity-modulated photon beams produced with dynamic multileaf collimation. Int. J. Radiat. Oncol. Biol. Phys. 35, 721–730 (1996).
Heemsbergen, W. D., Hoogeman, M. S., Hart, G. A., Lebesque, J. V. & Koper, P. C. Gastrointestinal toxicity and its relation to dose distributions in the anorectal region of prostate cancer patients treated with radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 61, 1011–1018 (2005).
Peeters, S. T. et al. Localized volume effects for late rectal and anal toxicity after radiotherapy for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 64, 1151–1161 (2006).
Dearnaley, D. P. et al. The early toxicity of escalated versus standard dose conformal radiotherapy with neo-adjuvant androgen suppression for patients with localised prostate cancer: results from the MRC RT01 trial (ISRCTN47772397). Radiother. Oncol. 83, 31–41 (2007).
Matzinger, O. et al. Acute toxicity of curative radiotherapy for intermediate- and high-risk localised prostate cancer in the EORTC trial 22991. Eur. J. Cancer 45, 2825–2834 (2009).
Pinkawa, M. et al. Combination of dose escalation with technological advances (intensity-modulated and image-guided radiotherapy) is not associated with increased morbidity for patients with prostate cancer. Strahlenther. Onkol. 187, 479–484 (2011).
Shirato, H. et al. Feasibility of insertion/implantation of 2.0-mm-diameter gold internal fiducial markers for precise setup and real-time tumor tracking in radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 56, 240–247 (2003).
Lu, W. et al. Deformable registration of the planning image (kVCT) and the daily images (MVCT) for adaptive radiation therapy. Phys. Med. Biol. 51, 4357–4374 (2006).
Willoughby, T. R. et al. Target localization and real-time tracking using the Calypso 4D localization system in patients with localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 65, 528–534 (2006).
Rajendran, R. R. et al. Daily isocenter correction with electromagnetic-based localization improves target coverage and rectal sparing during prostate radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 76, 1092–1099 (2010).
Wachter, S. et al. The influence of a rectal balloon tube as internal immobilization device on variations of volumes and dose-volume histograms during treatment course of conformal radiotherapy for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 52, 91–100 (2002).
Ciernik, I. F., Baumert, B. G., Egli, P., Glanzmann, C. & Lütolf, U. M. On-line correction of beam portals in the treatment of prostate cancer using an endorectal balloon device. Radiother. Oncol. 65, 39–45 (2002).
Patel, R. R., Orton, N., Tomé, W. A., Chappell, R. & Ritter, M. A. Rectal dose sparing with a balloon catheter and ultrasound localization in conformal radiation therapy for prostate cancer. Radiother. Oncol. 67, 285–294, (2003).
Sanghani, M. V. et al. Impact on rectal dose from the use of a prostate immobilization and rectal localization device for patients receiving dose escalated 3D conformal radiation therapy. Urol. Oncol. 22, 165–168 (2004).
Hille, A. et al. The impact of varying volumes in rectal balloons on rectal dose sparing in conformal radiation therapy of prostate cancer. A prospective three-dimensional analysis. Strahlenther. Onkol. 181, 709–716 (2005).
Elsayed, H. et al. Organ movements and dose exposures in teletherapy of prostate cancer using a rectal balloon. Strahlenther. Onkol. 183, 617–624 (2007).
van Lin, E. N., Hoffmann, A. L., van Kollenburg, P., Leer, J. W. & Visser, A. G. Rectal wall sparing effect of three different endorectal balloons in 3D conformal and IMRT prostate radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 63, 565–576 (2005).
Smeenk, R. J., van Lin, E. N., van Kollenburg, P., Kunze-Busch, M. & Kaanders, J. H. Anal wall sparing effect of an endorectal balloon in 3D conformal and intensity modulated prostate radiotherapy. Radiother. Oncol. 93, 131–136 (2009).
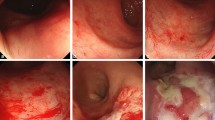
van Lin, E. N. et al. Reduced late rectal mucosal changes after prostate three-dimensional conformal radiotherapy with endorectal balloon as observed in repeated endoscopy. Int. J. Radiat. Oncol. Biol. Phys. 67, 799–811 (2007).
Lindsey, I., Guy, R. J., Warren, B. F. & Mortensen, N. J. Anatomy of Denonvilliers' fascia and pelvic nerves, impotence, and implications for the colorectal surgeon. Br. J. Surg. 87, 1288–1299 (2000).
Villers, A., McNeal, J. E., Freiha, F. S., Boccon-Gibod, L. & Stamey, T. A. Invasion of Denonvilliers' fascia in radical prostatectomy specimens. J. Urol. 149, 793–798 (1993).
Prada, P. J. et al. Transperineal injection of hyaluronic acid in the anterior perirectal fat to decrease rectal toxicity from radiation delivered with low-dose-rate brachytherapy for prostate cancer patients. Brachytherapy 8, 210–217 (2009).
Prada, P. J. et al. High-dose-rate interstitial brachytherapy as monotherapy in one fraction and transperineal hyaluronic acid injection into the perirectal fat for the treatment of favorable stage prostate cancer: treatment description and preliminary results. Brachytherapy 11, 105–110 (2012).
Wilder, R. B. et al. Cross-linked hyaluronan gel improves the quality of life of prostate cancer patients undergoing radiotherapy. Brachytherapy 10, 44–50 (2011).
Susil, R. C., McNutt, T. R., DeWeese, T. L. & Song, D. Effects of prostate-rectum separation on rectal dose from external beam radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 76, 1251–1258 (2010).
Hatiboglu, G., Pinkawa, M., Vallée, J. P., Hadaschik, B. & Hohenfellner, M. Application technique: placement of a prostate-rectum spacer in men undergoing prostate radiation therapy. BJU Int. 110, E647–652 (2012).
Levy, Y. et al. Biodegradable inflatable balloon for reducing radiation adverse effects in prostate cancer. J. Biomed. Mater. Res. B Appl. Biomater. 91, 855–867 (2009).
Garg, M. K. et al. Novel biodegradable balloon (Bioprotect Spaceguard) provides reproducible geometry and significantly reduces rectal dose in patients receiving IMRT for prostate cancer: single arm phase I multi-institutional international study [abstract 2384]. Int. J. Radiat. Oncol. Biol. Phys. 81 (Suppl. 1), S394 (2011).
D'Argenio, G. et al. Butyrate, mesalamine, and factor XIII in experimental colitis in the rat: effects on transglutaminase activity. Gastroenterology 106, 399–404 (1994).
Mortensen, F. V., Nielsen, H., Aalkjaer, C., Mulvany, M. J. & Hessov, I. Short chain fatty acids relax isolated resistance arteries from the human ileum by a mechanism dependent on anion-exchange. Pharmacol. Toxicol. 75, 181–185 (1994).
Kvietys, P. R. & Granger, D. N. Effect of volatile fatty acids on blood flow and oxygen uptake by the dog colon. Gastroenterology 80, 962–969 (1981).
Vavassori, V. et al. Predictors for rectal and intestinal acute toxicities during prostate cancer high-dose 3D-CRT: results of a prospective multicenter study. Int. J. Radiat. Oncol. Biol. Phys. 67, 1401–1410 (2007).
Zapatero, A. et al. Risk-adapted androgen deprivation and escalated three-dimensional conformal radiotherapy for prostate cancer: does radiation dose influence outcome of patients treated with adjuvant androgen deprivation? A GICOR study. J. Clin. Oncol. 23, 6561–6568 (2005).
D'Amico, A. V. et al. A practical method to achieve prostate gland immobilization and target verification for daily treatment. Int. J. Radiat. Oncol. Biol. Phys. 51, 1431–1436 (2001).
McGary, J. E., Teh, B. S., Butler, E. B. & Grant, W. 3rd. Prostate immobilization using a rectal balloon. J. Appl. Clin. Med. Phys. 3, 6–11 (2002).
El-Bassiouni, M. et al. Target motion variability and on-line positioning accuracy during externa-beam radiation therapy of prostate cancer with an endorectal balloon device. Strahlenther. Onkol. 182, 531–536 (2006).
Vargas, C. et al. Cine-magnetic resonance imaging assessment of intrafraction motion for prostate cancer patients supine or prone with and without a rectal balloon. Am. J. Clin. Oncol. 33, 11–16 (2010).
Both, S. et al. Real-time study of prostate intrafraction motion during external beam radiotherapy with daily endorectal balloon. Int. J. Radiat. Oncol. Biol. Phys. 81, 1302–1309 (2011).
van Lin, E. N. et al. The effect of an endorectal balloon and off-line correction on the interfraction systematic and random prostate position variations: a comparative study. Int. J. Radiat. Oncol. Biol. Phys. 61, 278–288 (2005).
Wang, K. K. A study to quantify the effectiveness of daily endorectal balloon for prostate intrafraction motion management. Int. J. Radiat. Oncol. Biol. Phys. 83, 1055–1063 (2012).
Smeenk, R. J. et al. An endorectal balloon reduces intrafraction prostate motion during radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 83, 661–669 (2012).
Author information
Authors and Affiliations
Contributions
Both authors researched the data for the article, contributed to the discussion of its content, wrote and edited the manuscript before submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
About this article
Cite this article
Valdagni, R., Rancati, T. Reducing rectal injury during external beam radiotherapy for prostate cancer. Nat Rev Urol 10, 345–357 (2013). https://doi.org/10.1038/nrurol.2013.96
Published:
Issue Date:
DOI: https://doi.org/10.1038/nrurol.2013.96
This article is cited by
-
Real-time in vivo rectal wall dosimetry using MOSkin detectors during linac based stereotactic radiotherapy with rectal displacement
Radiation Oncology (2017)
-
Multivariate normal tissue complication probability modeling of gastrointestinal toxicity after external beam radiotherapy for localized prostate cancer
Radiation Oncology (2013)
