
Abstract
Background:
Ureaplasma causes sepsis in human neonates. Although erythromycin has been the standard treatment, it is not always effective. No published reports have evaluated Ureaplasma sepsis in a neonatal model. We hypothesized that appropriate antibiotic treatment improves Ureaplasma sepsis in a neonatal mouse model.
Methods:
Two ATCC strains and two clinical strains of Ureaplasma were evaluated in vitro for antibiotic minimum inhibitory concentration (MIC). In addition, FVB albino mice pups infected with Ureaplasma were randomly assigned to saline, erythromycin, or azithromycin therapy and survival, quantitative blood culture, and growth were evaluated.
Results:
MICs ranged from 0.125 to 62.5 µg/ml and 0.25 to 1.0 µg/ml for erythromycin and azithromycin, respectively. The infecting strain and antibiotic selected for treatment appeared to affect survival and bacteremia, but only the infecting strain affected growth. Azithromycin improved survival and bacteremia against each strain, whereas erythromycin was effective against only one of four strains.
Conclusion:
We have established a neonatal model of Ureaplasma sepsis and observed that treatment outcome is related to infecting strain and antibiotic treatment. We speculate that appropriate antibiotic selection and dosing are required for effective treatment of Ureaplasma sepsis in neonates, and this model could be used to further evaluate these relationships.
Similar content being viewed by others

Main
Ureaplasma is the single most common microorganism isolated from the lower respiratory tract of newborn infants (1,2,3) and causes neonatal sepsis (4,5,6,7,8,9,10,11) and meningitis (10,12,13,14). The sepsis events have been associated with pulmonary hypertension (7,11), pneumonia (9), increased systemic inflammatory response syndrome (6,10), chronic lung disease (6), and intraventricular hemorrhage (10).
Erythromycin has been the drug of choice to prevent or treat Ureaplasma infection in the neonate (15,16,17). However, it failed to prevent infection in 17 studies (18) and failed as treatment in five studies (19). More recently, several studies have reported on the variable sensitivity of Ureaplasma to antibiotics (20,21). A recent Cochrane review suggested that controlled trials are required to determine whether antibiotic therapy of Ureaplasma reduces infection or death in preterm infants (18). It would appear logical that such an evaluation should initially begin in animals so that clinical studies could be optimized. However, no one has developed an animal model of Ureaplasma sepsis or evaluated antibiotic prevention or treatment in such a model.
It was our objective to determine whether appropriate antibiotic treatment improves Ureaplasma sepsis in the neonatal mouse. Specifically, we sought to (i) determine the antibiotic sensitivity of several Ureaplasma strains in vitro; (ii) develop a Ureaplasma suckling mouse model of sepsis; (iii) determine the efficacy of common antibiotics (i.e., erythromycin and azithromycin) in treating Ureaplasma sepsis due to various strains using this model; and (iv) determine the relationship between infecting strain and/or antibiotic and outcome of sepsis in this model.
Results
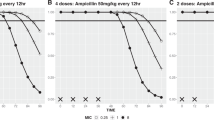
A description of the four selected organisms, including name, source, species, serotype, minimum inhibitory concentration (MIC), and minimum bactericidal concentration (MBC), is given in Table 1 . MICs ranged from 0.125 to 62.50 and 0.25 to 1.00 µg/ml for erythromycin and azithromycin, respectively. MBCs ranged from 0.25 to 125.00 and 1.00 to 3.90 µg/ml for erythromycin and azithromycin, respectively. For the organisms evaluated, the erythromycin MIC and MBC ranged widely, whereas the range for azithromycin was much narrower.
Figure 1 illustrates the survival percentage of suckling mice after Ureaplasma infection by various strains and treatments. The pup survival was significantly dependent on the infecting strain (P < 0.001), treatment (P < 0.001), and interaction of the infecting strain with treatment (P = 0.037). For strains 33697, B140, and B079, the survival rate was significantly increased with azithromycin treatment as compared with erythromycin or saline, whereas erythromycin was not significantly different from saline. For strain 33698, the survival rate was significantly increased with azithromycin or erythromycin as compared with saline, whereas azithromycin was not significantly different from erythromycin.

Percentage survival of suckling mice 8 d after Ureaplasma infection by various strains. Treatment groups include saline (white), erythromycin (black), and azithromycin (dark gray). For strains 33697, B140, and B079, the survival rate was significantly increased (P ≤ 0.05) with azithromycin (*) treatment as compared with erythromycin, or azithromycin (†) vs. saline, whereas erythromycin was not significantly different from saline. For strain 33698, the survival rate was significantly increased (P ≤ 0.05) with azithromycin (†) or erythromycin (†) vs. saline, whereas azithromycin was not significantly different from erythromycin. Each group began with 70 pups. A P value ≤0.05 was considered significant.
Figure 2 illustrates the quantitative bacteremia of suckling mice after Ureaplasma infection by various strains and treatments. The quantitative bacteremia was significantly dependent on the infecting strain (P < 0.001) and treatment (P < 0.001), and suggested an interaction of the infecting strain with treatment (P = 0.003). For strain 33697, the bacterial concentration was significantly decreased with azithromycin or erythromycin vs. saline, whereas azithromycin was not significantly different from erythromycin. For strain 33698, the bacterial concentration was significantly decreased with azithromycin treatment as compared with saline but not erythromycin, and erythromycin was not significantly different from saline. For strains B140 and B079, the bacterial concentrations were significantly decreased with azithromycin treatment as compared with erythromycin or azithromycin as compared with saline, whereas erythromycin was not significantly different from saline.

Mean number of bacteria (colony-changing units (ccu)/ml) in the blood of suckling mice 30 h after Ureaplasma infection by various strains. Treatment groups include saline (white), erythromycin (black), and azithromycin (dark gray). For strain 33697, the bacterial concentration was significantly decreased (P ≤ 0.05) with azithromycin (†) or erythromycin (†) vs. saline, whereas azithromycin was not significantly different from erythromycin. For strain 33698, the bacterial concentration was significantly decreased (P ≤ 0.05) with azithromycin (†) treatment as compared with saline but not erythromycin, and erythromycin was not significantly different from saline. For strains B140 and B079, the bacterial concentrations were significantly decreased (P ≤ 0.05) with azithromycin (*) treatment as compared with erythromycin, or azithromycin (†) vs. saline, whereas erythromycin was not significantly different from saline. Each group contained 18 pups. A P value ≤0.05 was considered significant.
Figure 3 illustrates the rate of growth of suckling mice after Ureaplasma infection by various strains and treatments. The pup growth rate after infection did not appear to vary with the infecting strain, but did vary with the treatment group (P < 0.05). For strains 33697, 33698, and B 140, the rate of growth was significantly increased with azithromycin treatment as compared with saline but not with erythromycin treatment, and erythromycin was not significantly different from saline. For strain B079, the pup rate of growth was significantly increased with azithromycin treatment as compared with erythromycin or saline, whereas erythromycin was not significantly different from saline.

Growth. Mean growth (g/d) of suckling mice over 8 d after Ureaplasma infection by various strains. Treatment groups include saline (white), erythromycin (black), and azithromycin (dark gray). For strains 33697, 33698, and B140, the pup rate of growth was significantly increased (P ≤ 0.05) with azithromycin (†) treatment as compared with saline but not erythromycin, and erythromycin was not significantly different from saline. For strain B079, the pup rate of growth was significantly increased (P ≤ 0.05) with azithromycin (*) treatment as compared with erythromycin or azithromycin (†) vs. saline, whereas erythromycin was not significantly different from saline. Each group began with 70 pups. A P value ≤0.05 was considered significant.
Discussion
Specialized, but not routine, blood culture methods are required to identify Ureaplasma from blood specimens (22). Several studies have identified Ureaplasma in neonatal blood cultures as part of sepsis evaluations using specialized techniques, including: two case reports of neonatal sepsis with pulmonary hypertension (7,11); one case report of neonatal sepsis with pneumonia (9); 17.4% of cord blood cultures from 351 preterm infants (6); 18.7% of cord blood from 246 preterm infants (10); 12.6% of neonatal blood cultures from 106 preterm infants (8); and 6% of 221 preterm infants with clinical sepsis (4). Despite the potential for Ureaplasma sepsis, blood cultures of the neonate generally do not include investigation for Ureaplasma as a source of infection. In part, the lack of Ureaplasma identification may be due to limited information about this pathogen and/or the significant additional cost of the process for identification of this organism (e.g., specialized culture media, training, staffing, additional equipment, and supplies needed for confirmation). Most laboratories send their few requests for detection of Ureaplasma in blood culture to central specialized laboratories, with frequent loss of the organism in transport (22).
Antibiotic treatment for suspected or confirmed Ureaplasma infection has generally consisted of erythromycin (15,16,17); however, this drug has failed to prevent (18) or treat infection (19). Recently, several studies have reported the variable sensitivity of Ureaplasma to antibiotics (20,21), and some small studies have found azithromycin (23) or clarithromycin (24) to be effective for treatment of chronic lung disease. A Cochrane review suggests that controlled trials are required to determine whether (and which) antibiotic therapy of Ureaplasma reduces infection or death in preterm infants (18).
This is the first study to report an animal model for Ureaplasma sepsis. Although there are several animal models for Ureaplasma-associated lung disease, only one has been evaluated for bacteremia (21). In that model, blood culture and PCR, following a much smaller infecting dose and several weeks after treatment, were also evaluated. Thus, the organism may have been cleared, the infecting dose may have been too small (50% of the dose used in this study), or the organism undetectable because of its mucosal and intracellular association (21). Our model is less expensive and could be used to evaluate future treatments for this infection.
This study also reveals that in vitro and in vivo Ureaplasma sensitivity to antibiotics varies with the infecting strain and antibiotic used. As a result, to optimize treatment, clinicians should be aware of the sensitivity of their infecting strain or of those in their community. Initial antibiotic therapy should begin based on local data of Ureaplasma antibiotic sensitivities and may need to be adjusted once susceptibility of the specific isolate is available (25). It is now possible to detect antibiotic resistance in Ureaplasma within 48 h of a positive culture identifying them for further molecular analysis (26).
The pharmacokinetics of similar doses of azithromycin and erythromycin therapy in mice has been previously reported (21). Whereas serum levels of erythromycin appeared to reflect clinical activity, those of azithromycin did not. It may be that azithromycin efficacy is better reflected with tissue levels due to its bacterial killing and other effects (27) such as downregulation of inflammation, increased mucous clearance, prevention of bacterial biofilm formation, reduced activation of the immune system (cytokines, chemokines, and neutrophils), decreased production of reactive oxygen species, and blocking activation of nuclear transcription factors (28). Macrolide effects are also time- and dose-dependent, although the mechanisms underlying this are not clear. Antibiotic serum levels may not be helpful in the routine treatment of this infection; however, the sensitivity of the organism in vitro does appear to be related to outcome in this mouse sepsis model.
We conclude that Ureaplasma in vitro sensitivity via MIC and MBC ranged widely for erythromycin and more narrowly for azithromycin. In our neonatal mouse model of Ureaplasma sepsis, the infecting strain and antibiotic selected for treatment appeared to affect survival and bacteremia, but only the infecting strain affected growth. We speculate that development of effective strategies to treat Ureaplasma infection in the neonate will improve clinical outcomes, and those strategies should include early identification of infected neonates, determination of organism sensitivity in vitro, and selection of appropriate antibiotic therapy and dosing.
Methods
Organisms
We selected four strains of Ureaplasma: an ATCC (Manassas, VA) strain 33698 with serotype 13 (Ureaplasma urealyticum); an ATCC strain 33697 with serotype 14 (Ureaplasma parvum); a clinical strain B140 from a 23-wk placenta with serotype 6 (U. parvum); and a clinical strain B079 from a 25-wk placenta with serotype 14 (U. parvum). The species and serotypes selected reflected the predominant species and serotypes in the clinical strains from placentas and amniotic fluid of preterm births as reported by others (29,30,31,32) and observed by us (unpublished data: Weisman LE, et al. E-PAS 2009:3877.412). Ureaplasma species was identified utilizing PCR as described previously (33).
Organism Preparation
Strains were obtained from a frozen stock solution (5 × 106 color-changing units (ccu)/ml) diluted 1/100 with 10B broth (Remel, Lenexa, KS), grown 16 h at 37 °C, and spun down at 3,000 rpm for 30 min. Supernatant was poured off and precipitate resuspended in 900 µl of 10B. This suspension was used for intramuscular injection at a final concentration of 5 × 106 ccu/ml. The concentration was confirmed by quantitative culturing of the injectate.
Antibiotics
Erythromycin (USP, Rockville, MD) was selected based on historical data and practice (1,18,34) and administered intraperitoneally at 20 mg/kg/dose twice a day for 3 d (21). Azithromycin (Baxter, Deerfield, IL) was selected based on current and local data (17,21) and administered intraperitoneally at 12 mg/kg/dose once a day for 3 d (21).
MIC and MBC
MIC and MBC were determined using a microdilution method as previously reported (35). In brief, each antibiotic was serially twofold diluted in 10B broth to achieve final well concentrations ranging from 0.03 to 500 µg/ml. The Ureaplasma strain was added to achieve a final well concentration of 105 ccu/ml. Plates were sealed, incubated aerobically at 37 °C, and examined frequently until there was color change in the antibiotic-free control wells (usually <24 h). MIC was the lowest concentration of drug with no medium color change. From each well of the MIC microtiter plate that did not change color, 30 µl was added to 2.97 ml of 10B broth (1:100 dilution) and incubated at 37 °C for 7 d. The MBC was the lowest concentration of antibiotic in which no color change in the medium was observed. All wells had culture confirmation performed on an A7 agar plate.
Animals
FVB albino mice (Charles River Laboratories, Wilmington, MA) were time impregnated and fed antibiotic-free water and food ad libitum, and delivered about 10 pups per dam at 18–20 d gestation. Pups were kept with their delivering dam throughout each experiment. Animals were placed under barrier conditions before infection. Surviving pups were euthanized with injection of 2.25–4.5 ml/kg of 20% Rodent Comboanesthetic III (ketamine 37.6 mg/ml, xylazine 1.92 mg/ml, and acepromazine 0.38 mg/ml). The Baylor College of Medicine Institutional Animal Care and Use Committee approved these experiments.
Sepsis Model
Two-day-old mice pups were infected with a single strain of Ureaplasma twice daily for 3 d via intramuscular injection (0.1 ml day 2, 0.2 ml day 3, and 0.3 ml day 4). One hour after initial infection, littermates were randomly assigned to treatment with normal saline, erythromycin, or azithromycin intraperitoneally (refer to Antibiotics section). Pups were evaluated daily for survival and growth for 8 d.
Ureaplasma Blood Cultures
Blood of 100 µl was obtained via cardiac puncture from each pup of selected litters 30 h after treatment was initiated. The culture samples were placed in 900 µl of 10B broth, serially diluted, and incubated at 37 °C. Samples were examined for 2 wks for color change and cultures confirmed on A7 agar (36) and by PCR (21).
Statistical Analysis
Sample size was estimated to be 70 pups per group on the basis of the assumptions that the normal saline-treated survival would be 40% and antibiotic-treated survival would be 65%, with a P value < 0.05 and a power of 0.80. Survival was evaluated by χ2 or Fisher’s exact test as appropriate. Blood culture data were analyzed by Kruskal–Wallis test. Growth curves were constructed for individual pups (even those who died in the study period), slopes calculated, and means of slopes compared for each group by one-way ANOVA. A P value < 0.05 was considered significant. Multiple logistic regression or multiple linear regression was used to determine interaction of variables with outcomes. IBM SPSS Release 19 (International Business Machines, Armonk, NY) and GraphPad Prism Release 5 (GraphPad Software, La Jolla, CA) were used for analysis.
Statement of Financial Support
No extramural financial assistance was received in support of the study.
References
Cassell GH, Waites KB, Watson HL, Crouse DT, Harasawa R . Ureaplasma urealyticum intrauterine infection: role in prematurity and disease in newborns. Clin Microbiol Rev 1993;6:69–87.
Katz B, Patel P, Duffy L, Schelonka RL, Dimmitt RA, Waites KB . Characterization of ureaplasmas isolated from preterm infants with and without bronchopulmonary dysplasia. J Clin Microbiol 2005;43:4852–4.
Zheng X, Watson HL, Waites KB, Cassell GH . Serotype diversity and antigen variation among invasive isolates of Ureaplasma urealyticum from neonates. Infect Immun 1992;60:3472–4.
Berger A, Witt A, Haiden N, Kretzer V, Heinze G, Pollak A . Amniotic cavity cultures, blood cultures, and surface swabs in preterm infants–useful tools for the management of early-onset sepsis? J Perinat Med 2004;32:446–52.
Cassell GH, Waites KB, Crouse DT, et al. Association of Ureaplasma urealyticum infection of the lower respiratory tract with chronic lung disease and death in very-low-birth-weight infants. Lancet 1988;2:240–5.
Goldenberg RL, Andrews WW, Goepfert AR, et al. The Alabama Preterm Birth Study: umbilical cord blood Ureaplasma urealyticum and Mycoplasma hominis cultures in very preterm newborn infants. Am J Obstet Gynecol 2008;198:43.e1–5.
Brus F, van Waarde WM, Schoots C, Oetomo SB . Fatal ureaplasmal pneumonia and sepsis in a newborn infant. Eur J Pediatr 1991;150:782–3.
Fonseca LT, Silveira RC, Procianoy RS . Ureaplasma bacteremia in very low birth weight infants in Brazil. Pediatr Infect Dis J 2011;30:1052–5.
Morioka I, Fujibayashi H, Enoki E, Yokoyama N, Yokozaki H, Matsuo M . Congenital pneumonia with sepsis caused by intrauterine infection of Ureaplasma parvum in a term newborn: a first case report. J Perinatol 2010;30:359–62.
Viscardi RM, Hashmi N, Gross GW, Sun CC, Rodriguez A, Fairchild KD . Incidence of invasive ureaplasma in VLBW infants: relationship to severe intraventricular hemorrhage. J Perinatol 2008;28:759–65.
Waites KB, Crouse DT, Philips JB III, Canupp KC, Cassell GH . Ureaplasmal pneumonia and sepsis associated with persistent pulmonary hypertension of the newborn. Pediatrics 1989;83:79–85.
Waites KB, Rudd PT, Crouse DT, et al. Chronic Ureaplasma urealyticum and Mycoplasma hominis infections of central nervous system in preterm infants. Lancet 1988;1:17–21.
Heggie AD, Jacobs MR, Butler VT, Baley JE, Boxerbaum B . Frequency and significance of isolation of Ureaplasma urealyticum and Mycoplasma hominis from cerebrospinal fluid and tracheal aspirate specimens from low birth weight infants. J Pediatr 1994;124:956–61.
Sethi S, Sharma M, Narang A, Aggrawal PB . Isolation pattern and clinical outcome of genital mycoplasma in neonates from a tertiary care neonatal unit. J Trop Pediatr 1999;45:143–5.
Waites KB, Crouse DT, Cassell GH . Antibiotic susceptibilities and therapeutic options for Ureaplasma urealyticum infections in neonates. Pediatr Infect Dis J 1992;11:23–9.
Tay ST, Boo NY, Khoo TB, Koay AS, Rohani MY . Prevalence and antibiotic susceptibility of Ureaplasma urealyticum in Malaysian neonates with respiratory distress. Med J Malaysia 1997;52:409–11.
Matlow A, Th’ng C, Kovach D, Quinn P, Dunn M, Wang E . Susceptibilities of neonatal respiratory isolates of Ureaplasma urealyticum to antimicrobial agents. Antimicrob Agents Chemother 1998;42:1290–2.
Mabanta CG, Pryhuber GS, Weinberg GA, Phelps DL . Erythromycin for the prevention of chronic lung disease in intubated preterm infants at risk for, or colonized or infected with Ureaplasma urealyticum. Cochrane Database Syst Rev 2003:CD003744.
Baier RJ, Loggins J, Kruger TE . Failure of erythromycin to eliminate airway colonization with ureaplasma urealyticum in very low birth weight infants. BMC Pediatr 2003;3:10.
Bayraktar MR, Ozerol IH, Gucluer N, Celik O . Prevalence and antibiotic susceptibility of Mycoplasma hominis and Ureaplasma urealyticum in pregnant women. Int J Infect Dis 2010;14:e90–5.
Walls SA, Kong L, Leeming HA, Placencia FX, Popek EJ, Weisman LE . Antibiotic prophylaxis improves Ureaplasma-associated lung disease in suckling mice. Pediatr Res 2009;66:197–202.
Pinna GS, Skevaki CL, Kafetzis DA . The significance of Ureaplasma urealyticum as a pathogenic agent in the paediatric population. Curr Opin Infect Dis 2006;19:283–9.
Ballard HO, Shook LA, Bernard P, et al. Use of azithromycin for the prevention of bronchopulmonary dysplasia in preterm infants: a randomized, double-blind, placebo controlled trial. Pediatr Pulmonol 2011;46:111–8.
Ozdemir R, Erdeve O, Dizdar EA, et al. Clarithromycin in preventing bronchopulmonary dysplasia in Ureaplasma urealyticum-positive preterm infants. Pediatrics 2011;128:e1496–501.
Clifford V, Tebruegge M, Everest N, Curtis N . Ureaplasma: pathogen or passenger in neonatal meningitis? Pediatr Infect Dis J 2010;29:60–4.
Beeton ML, Chalker VJ, Maxwell NC, Kotecha S, Spiller OB . Concurrent titration and determination of antibiotic resistance in ureaplasma species with identification of novel point mutations in genes associated with resistance. Antimicrob Agents Chemother 2009;53:2020–7.
Ballard HO, Bernard P, Qualls J, Everson W, Shook LA . Azithromycin protects against hyperoxic lung injury in neonatal rats. J Investig Med 2007;55:299–305.
Zarogoulidis P, Papanas N, Kioumis I, Chatzaki E, Maltezos E, Zarogoulidis K . Macrolides: from in vitro anti-inflammatory and immunomodulatory properties to clinical practice in respiratory diseases. Eur J Clin Pharmacol 2012;68:479–503.
Kasper DC, Mechtler TP, Reischer GH, et al. The bacterial load of Ureaplasma parvum in amniotic fluid is correlated with an increased intrauterine inflammatory response. Diagn Microbiol Infect Dis 2010;67:117–21.
Yi J, Yoon BH, Kim EC . Detection and biovar discrimination of Ureaplasma urealyticum by real-time PCR. Mol Cell Probes 2005;19:255–60.
Kim M, Kim G, Romero R, Shim SS, Kim EC, Yoon BH . Biovar diversity of Ureaplasma urealyticum in amniotic fluid: distribution, intrauterine inflammatory response and pregnancy outcomes. J Perinat Med 2003;31:146–52.
Martínez MA, Ovalle A, Santa-Cruz A, Barrera B, Vidal R, Aguirre R . Occurrence and antimicrobial susceptibility of Ureaplasma parvum (Ureaplasma urealyticum biovar 1) and Ureaplasma urealyticum (Ureaplasma urealyticum biovar 2) from patients with adverse pregnancy outcomes and normal pregnant women. Scand J Infect Dis 2001;33:604–10.
Kong F, Ma Z, James G, Gordon S, Gilbert GL . Species identification and subtyping of Ureaplasma parvum and Ureaplasma urealyticum using PCR-based assays. J Clin Microbiol 2000;38:1175–9.
Waites KB, Katz B, Schelonka RL . Mycoplasmas and ureaplasmas as neonatal pathogens. Clin Microbiol Rev 2005;18:757–89.
Waites KB, Crabb DM, Duffy LB . Comparative in vitro susceptibilities and bactericidal activities of investigational fluoroquinolone ABT-492 and other antimicrobial agents against human mycoplasmas and ureaplasmas. Antimicrob Agents Chemother 2003;47:3973–5.
Rudd PT, Cassell GH, Waites KB, Davis JK, Duffy LB . Ureaplasma urealyticum pneumonia: experimental production and demonstration of age-related susceptibility. Infect Immun 1989;57:918–25.
Acknowledgements
We thank Travis Markham for his work on the animal infection model and Elliot O’Brian Smith for his assistance in statistical analysis of the data.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Weisman, L., Leeming, A. & Kong, L. Appropriate antibiotic therapy improves Ureaplasma sepsis outcome in the neonatal mouse. Pediatr Res 72, 502–506 (2012). https://doi.org/10.1038/pr.2012.115
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2012.115
