
Abstract
Background
Lymph-node (LN) metastasis in prostate cancer (PC) is a main risk factor for tumor recurrence after radical prostatectomy (RP). Molecular analysis facilitates detection of small-volume LN metastases with higher sensitivity than histopathology. We aimed to prospectively evaluate six candidate gene markers for detection of pelvic LN metastases and to determine their ability to predict biochemical recurrence-free survival (bRFS) in patients treated with RP.
Methods
The expression of kallikrein 2, 3, and 4 (KLK2, KLK3, and KLK4), prostate-specific membrane antigen (PSMA), transmembrane serine protease 2 (TMPRSS2) and transient receptor potential cation channel subfamily M member 8 (TRPM8) was assessed using qPCR. We analyzed LNs from 111 patients (intermediate PC, n = 32 (29%); high-risk PC, n = 79 (71%)) who underwent RP and extended pelvic lymph-node dissection without neoadjuvant treatment.
Results
Overall, 2411 LNs were examined by molecular and histopathologic examination. Histopathology detected 69 LN metastases in 28 (25%) patients. KLK2 and KLK3 diagnostically performed best and classified all pN1-patients correctly as molecular node-positive (molN1/pN1). The concordance on LN level was best for KLK3 (96%). KLK2, KLK3, KLK4, PSMA, TMPRSS2, and TRPM8 reclassified 27 (24%), 32 (29%), 29 (26%), 8 (7%), 13 (12%), and 23 (21%) pN0-patients, respectively, as node-positive (pN0/molN1). On multivariable cox regression analysis molecular LN status (molN1 vs. molN0) using KLK3 (HR 4.0, p = 0.04) and TMPRSS2 (HR 5.1, p = 0.02) were independent predictors of bRFS. Median bRFS was shorter in patients with only molecular positive LNs (molN1/pN0) for KLK3 (24 months, p = 0.001) and for TMPRSS2 (12 months, p < 0.001) compared to patients with negative nodes (molN0/pN0) (median bRFS not reached).
Conclusions
For diagnostic purposes, KLK3 showed highest concordance with histopathology for detection of LN metastases in PC patients undergoing RP. For prognostic purposes, KLK3 and TMPRSS2 expression were superior to histopathologic LN status and other transcripts tested for molecular LN status. We suggest a combined KLK3/TMPRSS2 panel as a valuable diagnostic and prognostic tool for molecular LN analysis.
Similar content being viewed by others


Introduction
Prostate cancer (PC) remains the most common cancer among men both in Europe and the US and the second to third leading cancer-specific cause of death [1]. Presence of lymph-node (LN) metastasis in patients with PC undergoing radical prostatectomy (RP) is the strongest risk factor for both, tumor recurrence and cancer-specific mortality [2, 3]. In patients with LN-positive PC, adjuvant treatment after RP with either androgen-deprivation therapy (ADT) alone or ADT in combination with pelvic radiation therapy (RT) has shown a benefit in overall survival (OS), cancer-specific survival (CSS), and progression-free survival (PFS) [4,5,6,7]. LN staging is crucial to assign node-positive patients to adjuvant treatment and thereby prolong CSS in these patients [8, 9].
Cancer recurrence occurs in about 20% of patients with postoperative node-negative status following RP and is even more frequently observed in patients with high-risk features [10,11,12]. This might be explained by LN-understaging due to insufficient extent of LN dissection or localization of LN metastases outside of the dissection template, leading to false node-negative results. Accordingly, an extended pelvic LN dissection (ePLND) respecting the lymphatic draining sites of the prostate including the obturatoric fossa, internal, external, and common iliac field has been recommended by the European Association of Urology guidelines [13]. Another reason might be the presence of small-volume metastases within the dissected tissue that remain undetected by standard histopathology.
Previous studies therefore aimed to address this issue by applying quantitative polymerase chain reaction (qPCR) for molecular LN analysis to enhance sensitivity in comparison with histopathology [14,15,16]. Our group recently established a novel, validated qPCR assay quantifying prostate-specific Kallikrein 3 expression (KLK3 gene coding for PSA (prostate-specific antigen)) in fresh-frozen tissue from LNs [17]. We applied this method in a prospective biomarker trial with intermediate and high-risk PC patients undergoing RP with ePLND [18]. Herein, we demonstrated upstaging of one third of patients as node-positive by molecular LN examination (molN1) despite histopathologic negative LN status (pN0). Moreover, molecular LN status was a better predictor for biochemical recurrence than histopathologic LN status. Thus, molecular LN analysis has the potential to guide adjuvant treatment as a diagnostic tool and eventually to improve survival in PC.
Despite advances in the field, studies investigating the most suitable marker for molecular LN-staging accounting for the genetic intratumor heterogeneity in PC remain scarce [19]. Several candidate genes have been described but common study limitations are arbitrary gene selection, retrospective trial design and a lack of direct comparison between the described genes [20, 21].
Following a literature review and subsequent preclinical evaluation of candidate genes we identified six genes (kallikrein 2, 3, and 4 (KLK2, KLK3, and KLK4), prostate-specific membrane antigen (PSMA), transmembrane serine protease 2 (TMPRSS2), and transient receptor potential cation channel subfamily M member 8 (TRPM8)) suitable for molecular LN analysis with high expression in PC and low expression in peripheral blood mononuclear cells (PBMCs), which can be used as a model for detection of disseminated tumor cells in LNs [22]. Subsequently, this study aimed to prospectively investigate molecular LN analysis comparing the six candidate genes with histopathologic LN analysis as part of the aforementioned prospective biomarker trial in patients with intermediate and high-risk PC undergoing RP with ePLND. Objectives of this study were the assessment of detection rate of each gene in comparison with standard histopathology for detection of LN metastases as well as the association with biochemical recurrence-free survival (bRFS).
Patients and methods
The local ethics committee approved the present study (ID 2607/09), which was conducted according to the Declaration of Helsinki (NCT01615965). Written informed consent was obtained in all patients prior to participation. LN specimens were obtained from 111 prospectively enrolled patients who underwent open RP and ePLND between February 2010 and February 2013 for intermediate or high-risk PC at our institution according to D’Amico criteria (Gleason score at biopsy ≥ 7 or PSA ≥ 10 ng/ml or clinical tumor extension ≥ cT2b) [23]. The study was prospectively planned for the evaluation of the abovementioned six target genes. In a previously published, first analysis of this prospective biomarker trial we reported on the use of one of the six investigated candidate genes (KLK3) for molecular staging [18].
Exclusion criteria were the presence of any concomitant malignant tumor at the time of inclusion, previous radiation or ADT, acute or chronic infectious or inflammatory disease, severe cardiopulmonary, renal, hepatic or hematopoietic disease.
Open RP and ePLND were performed following a predefined template comprising the bilateral removal of LN tissue in the obturator fossa region and along the iliac vessels (external, internal, and common) [17].
The selection of target genes for this study, a detailed explanation on LN preparation and fixation, applied qPCR analyses, the method for cut-off determination as well as applied statistical methods are described in the Supplementary Material.
Endpoints and follow-up
Follow-up for determination of PSA levels and postoperative PC treatment was obtained at 3 month intervals during the first postoperative year, every 6 months during the second postoperative year and once every 12 months thereafter. A confirmed postoperative PSA value of >0.2 ng/ml was considered as biochemical recurrence. bRFS was defined as the time from RP to biochemical recurrence.
Results are reported in compliance with the REMARK criteria [24]. Primary objectives of this study are the diagnostic accuracy of each gene to correctly identify node-positive patients also detected by standard histopathology (pN1), the ability of each gene to detect LN metastases in pN0-patients as well as the potential of each marker to yield prognostic information.
Results
Patient characteristics and histopathology
Patient characteristics have been reported previously [18] (Supplementary Table 1). In brief, median patient age was 67. The evaluation of preoperative PC cancer risk revealed that 32 (29%) patients had intermediate and 79 (71%) had high-risk PC according to D’Amico et al. criteria [23].
A total of 3173 LNs were harvested from 111 patients, corresponding to a median of 27 LNs/patient (range 9–78) (Supplementary Fig. 1). After retrieval, 2411 LNs had a diameter > 3 mm and were analysed by both histopathology and qPCR as described (median 21 LNs/patient, range 6–48).
Overall, histopathology detected 69 LN metastases in 28 (25%) patients. Of 69 LN metastases, 66 were detected in LNs >3 mm and were thus also available for molecular LN analysis. The remaining three LN metastases were identified in histopathology as micrometastases in LNs <3 mm. These LNs were found in patients that were already staged as node positive in LNs >3 mm.
Comparison of detection rate of molecular and histopathologic lymph-node analysis
Detection rate of LN metastasis (patient- and lymph nodewise) according to molecular LN analysis and histopathology is given in Table 1.
On patient level, both KLK3 and KLK2 identified all histopathological node-positive patients (n = 28; 100%) by molecular examination. KLK4 and TRPM8 were able to correctly identify 26/28 patients, respectively, whereas PSMA and TMPRSS2 identified a total of 25/28 patients node positive by standard histopathology. Compared to histopathology, molecular staging using KLK3, KLK2, KLK4, PSMA, TMPRSS2, and TRPM8 led to an upstaging from N0 to N1 of 32 (29%), 27 (24%), 31 (28%), 11 (10%), 16 (14%), and 25 (23%) patients, respectively, otherwise missed by standard histopathology (molN1/pN0).
On LN level KLK3 yielded the highest concordance with histopathologic positive LNs (66 of 69; 96%) followed by KLK2 (62 of 69; 90%), TMPRSS2 (56 of 69; 83%), KLK4 (56 of 69; 81%), PSMA (53 of 59; 77%), and TRPM8 (56 of 69; 81%). The concordance for different transcripts used for molecular LN analysis is depicted in Supplementary Fig. 2.
Association of molecular and histopathologic lymph-node status with biochemical recurrence-free survival
Median follow-up for all 111 patients was 48 months (95% CI: 44–49 months). Overall, biochemical recurrence was observed in 52 patients (47%).
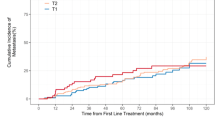
In a multivariable cox regression model including established risk factors and LN status with dichotomous marker expression, TMPRSS2 (HR 5.1, 95% CI (1.4–19.0), p = 0.02) and KLK3 (HR 4.0, 95% CI (1.1–15.2), p = 0.04) remained the only statistically significant, independent predictors of bRFS and thus were superior to histopathologic LN examination (HR 1.1, 95% CI (0.5–2.2), p = 0.8) (Table 2a). Figure 1 shows the corresponding Kaplan–Meier curves for the estimation of bRFS by histopathology alone (pN0 vs. pN1), TMPRSS2 alone (molN1 vs. molN0) and KLK3 alone (molN1 vs. molN0), illustrating a shorter bRFS for patients with positive LNs. Median bRFS was 12 months (95% CI 6.1 vs. 17.9) in patients with TMPRSS2-positive LNs and not reached in patients in patients with TMPRSS2-negative LNs (log-rank p value < 0.001; Fig. 1b). Median bRFS was 24 months (95% CI 0 vs. 49.2) in patients with KLK3-positive LNs and not reached in patients in patients with KLK3-negative LNs (log-rank p value < 0.001; Fig. 1c).

Patients with positive lymph nodes, both by histopathology (a, pN1 vs. pN0) or molecular lymph-node analysis using KLK3 (b, molN1 vs. molN0), and TMPRSS2 (c, molN1 vs. molN0) had a shorter biochemical recurrence-free survival. Pt Patients.
In a multivariable cox regression model analysis including established risk factors and LN status with continuous molecular marker expression only TMPRSS2 remained an independent predictor of bRFS (Table 2b).
When combining both molecular and histopathologic LN status, we evaluated four patient risk groups with either negative LNs (molN0/pN0), only molecular positive LNs (molN1/pN0), only histopathologic positive LNs (molN0/pN1) or molecular and histopathologic positive LNs (molN1/pN1) and assessed their association with bRFS (Supplementary Table 2, Fig. 2). When compared to patients with LN-negative patients (molN0/pN0), both patients with only molecular positive LNs (molN1/pN0) as well as patients with molecular and histopathologic positive LNs exhibited a significantly elevated risk of biochemical recurrence for each of the selected genes (Supplementary Table 2). Figure 2 depicts the corresponding Kaplan–Meier curves for the combination of either histopathologic LN status with KLK3 (Fig. 2a) or histopathologic LN status with TMPRSS2 (Fig. 2b). For KLK3, median bRFS was significantly shorter in molN1/pN1-patients (9 months; (HR 5.4 (95% CI 2.6–11.5) p < 0.001) and molN0/pN1-patients (24 months; (HR 3.7 (95% CI 1.8–7.6) p = 0.001) compared to molN0/pN0-patients, in whom median bRFS was not reached. For TMPRSS2, median bRFS was significantly shorter in molN1/pN1-patients (6 months; (HR 5.4 (95% CI 2.8–10.5) p < 0.001) and molN0/pN1-patients (12 months; (HR 5.6 (95% CI 2.8–11.2) p < 0.001) compared to molN0/pN0-patients, in whom median bRFS also was not reached. Notably, two patients were LN-positive in histopathology but negative for TMPRSS2 expression (pN1/molN0) and both did not show biochemical recurrence during the observation period. One of the two pN1/molN0-patients received adjuvant ADT; the other patient, however, did not receive adjuvant radiation or ADT.

For both KLK3 (a) and TMPRSS2 (b), median bRFS was significantly shorter in molN1/pN1-patients and molN0/pN1-patients as compared to molN0/pN0-patients, in whom median bRFS was not reached. Pt Patients.
When combining molecular status for KLK3 and TMPRSS2, three risk groups were identified: patients negative for either marker (molN0_KLK3 and molN0_TMPRSS2), patients positive for KLK3 but negative for TMPRSS2 (molN1_KLK3 and molN0_TMPRSS2) as well as patients positive for both KLK3 and TMPRSS2 (molN1_KLK3 and molN1_TMPRSS2). There was no patient positive for TMPRSS2 but negative for KLK3. Positivity for both KLK3 and TMPRSS2 was a statistically significant predictor of biochemical recurrence-free survival (HR = 6.8 95% CI 3.4–13.5), while patients only positive for KLK3 showed an elevated risk, which was not statistically significant (HR = 1.7 95% CI 0.7–4.4) (Supplementary Fig. 3).
Discussion
About 20% of patients develop biochemical recurrence after RP [25, 26]. The identification of patients at risk for biochemical recurrence is crucial to guide adjuvant treatment and thereby improve prognosis.
In a previous analysis of this prospective biomarker trial we demonstrated the diagnostic and prognostic superiority of molecular LN staging using expression of the prostate-specific gene KLK3 as compared to conventional histopathology for detection of LN metastasis in PC patients undergoing RP with ePLND for intermediate and high-risk PC [18]. Of note, there is a substantial genetic heterogeneity in PC and the optimal transcript used for molecular LN analysis has yet to be defined [19, 27].
In this study we prospectively compared the candidate transcripts KLK2, KLK3, KLK4, PSMA, TMPRSS2, and TRPM8 for molecular LN staging, which were identified from a systematic literature review and were selected based on systematic preclinical evaluation [22]. These transcripts were subsequently evaluated in a large, homogeneous cohort of intermediate and high-risk PC patients treated with RP and template ePLND. Our results suggest that for diagnostic purposes KLK2 or KLK3 quantification alone may suffice to identify patients harboring PC metastases. On patient level, each of both transcripts showed 100% concordance with histopathologic pN1-status and lead to upstaging from N0 to N1 in about one quarter of patients. In addition, on LN level KLK3 showed the highest concordance with histopathologic positive nodes and showed the highest sensitivity with upstaging from N0 to N1 suggesting that KLK3 analysis might be the optimal diagnostic transcript for molecular LN analysis.
Considering prognostic purposes, on the other hand, quantification of both KLK3 and TMPRSS2 in LNs were independent predictors of bRFS in a dichotomous marker expression model and TMPRSS2 was the only independent predictor in a continuous marker expression model. While TMPRSS2 missed two patients with histopathologic positive LNs, interestingly these patients did not develop biochemical recurrence. While in one patient this observation is explained by adjuvant ADT, the other patient did not receive any adjuvant treatment which provokes the hypothesis of lower risk of biochemical recurrence in patients with TMPRSS2-negative but histopathologic positive LNs. However, given the low prevalence this observation is hypothesis-generating at best and warrants further evaluation in larger patient cohorts. Taken together, our data support a combined approach of KLK3 and TMPRSS2 quantification in LNs to yield optimal diagnostic and prognostic information.
Our findings extend previous studies which proposed that a combination of either KLK3 with PSMA or KLK3 with KLK2 might most precisely identify PC metastases and predict biochemical recurrence [15, 28]. Miyake et al. prospectively evaluated the combination of KLK3 with PSMA for molecular LN staging and found that positivity for this combination was an independent predictor of bRFS [15, 16]. However, in their trial both transcripts were only analyzed as a combination and their unique utility for diagnostic and prognostic purposes was not reported. Kusuda et al. expanded the analysis of Miyake et al. by retrospectively quantifying the KLK2, PSCA, and DD3 in the same LNs obtained from 120 patients and compared them to KLK3 and PSMA-based molecular LN staging [16]. Kusuda et al. suggested that a combination of KLK3 and KLK2 most precisely predicted bRFS.
In our prospective trial, we only included candidate genes showing high expression in PC cell lines and low expression in PBMCs at preclinical evaluation [22]. PSCA and DD3 failed these criteria and were therefore not included. Nonetheless, the Kallikreins 2, 3 and 4 as well as PSMA, TMPRSS2 and TRPM8 passed these criteria. While our clinical trial validated the genes KLK2 and KLK3 as sufficient for diagnostic purposes to detect LN metastases, KLK3 and TMPRSS2 expression in LNs were identified as independent predictors of bRFS. A clinical application could be the use of KLK3 and TMPRSS2 to trigger adjuvant treatment such as radiation of the pelvic lymphatic draining sites, which has been shown to improve CSS in patients with limited histopathologic nodal involvement [4].
While the genes KLK2 and KLK3 have been studied extensively, only few reports exist on TMPRSS2. TMPRSS2, a member of the serine protease family, was found upregulated in PC and downregulated in androgen-independent PC, underlining its potential role in molecular PC detection. Ko et al. demonstrated that TMPRSS2 mediates maltriptase activation along with damage to the extracelluar matrix, hence promoting androgen-induced PC cell invasion, growth, and metastatic spread [29]. In PC, the 5-prime untranslated region of the TMPRSS2 gene was demonstrated to frequently bind to the oncogene ERG, generating TMPRSS2/ERG fusion transcripts [30]. One previous study confirmed the overexpression of TMPRSS2 mRNA in poorly differentiated PC [31]. Research on the expression of TMPRSS2 RNA expression in the human body revealed enhanced expression of TMPRSS2 RNA in the small intestine, pancreas and the prostate [32]. However, to our knowledge our study for the first time evaluated its use for molecular LN staging in PC.
A common limitation of molecular staging is that nodal morphology (e.g., metastasis size and extracapsular extension) cannot be obtained. However, mRNA transcript quantification by qPCR (especially considering small-volume metastases) shows increased sensitivity in comparison with standard histopathology and overcomes the issue of histopathology-associated sampling errors on nodal slicing or failure to detect small lesions on microscopic examination. Strengths of this study were above all its prospective design with inclusion of intermediate and high-risk PC patients treated with RP and a standardized template ePLND as well as the inclusion of candidate genes following systematic selection with preclinical evaluation and the determination of molecular cut-offs (molN1 vs. molN0) by a validated statistical method.
The results of this study suggest that the quantification of KLK3 by qPCR is sufficient for diagnostic purposes for molecular LN evaluation. For prognostic information, however, both KLK3 and TMPRSS2 were independent predictors for biochemical recurrence in PC patients undergoing RP with ePLND for intermediate and high-risk localized PC. A combined panel for KLK3 and TMPRSS2 transcript quantification ought to be evaluated prospectively to gain insight on stronger endpoints than bRFS.
References
Center MM, Jemal A, Lortet-Tieulent J, Ward E, Ferlay J, Brawley O, et al. International variation in prostate cancer incidence and mortality rates. Eur Urol. 2012;61:1079–92.
Cheng L, Zincke H, Blute ML, Bergstralh EJ, Scherer B, Bostwick DG. Risk of prostate carcinoma death in patients with lymph node metastasis. Cancer. 2001;91:66–73.
Briganti A, Karnes JR, Da Pozzo LF, Cozzarini C, Gallina A, Suardi N, et al. Two positive nodes represent a significant cut-off value for cancer specific survival in patients with node positive prostate cancer. A new proposal based on a two-institution experience on 703 consecutive N+ patients treated with radical prostatectomy, extended pelvic lymph node dissection and adjuvant therapy. Eur Urol. 2009;55:261–70.
Abdollah F, Karnes RJ, Suardi N, Cozzarini C, Gandaglia G, Fossati N, et al. Impact of adjuvant radiotherapy on survival of patients with node-positive prostate cancer. J Clin Oncol. 2014;32:3939–47.
Messing EM, Manola J, Yao J, Kiernan M, Crawford D, Wilding G, et al. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol. 2006;7:472–9.
Touijer KA, Karnes RJ, Passoni N, Sjoberg DD, Assel M, Fossati N, et al. Survival outcomes of men with lymph node-positive prostate cancer after radical prostatectomy: a comparative analysis of different postoperative management strategies. Eur Urol. 2018;73:890–6.
Siddiqui ZA, Krauss DJ. Adjuvant androgen deprivation therapy for prostate cancer treated with radiation therapy. Transl Androl Urol. 2018;7:378–89.
Jang TL, Patel N, Faiena I, Radadia KD, Moore DF, Elsamra SE, et al. Comparative effectiveness of radical prostatectomy with adjuvant radiotherapy versus radiotherapy plus androgen deprivation therapy for men with advanced prostate cancer. Cancer. 2018;124:4010–22.
De Cicco L. Effectiveness of radical prostatectomy with adjuvant radiotherapy versus radiotherapy plus androgen deprivation therapy for men with advanced prostate cancer: do we have certainties today? Cancer. 2019. https://doi.org/10.1002/cncr.32055.
Mullins JK, Feng Z, Trock BJ, Epstein JI, Walsh PC, Loeb S. The impact of anatomical radical retropubic prostatectomy on cancer control: the 30-year anniversary. J Urol. 2012;188:2219–24.
Boorjian SA, Eastham JA, Graefen M, Guillonneau B, Karnes RJ, Moul JW, et al. A critical analysis of the long-term impact of radical prostatectomy on cancer control and function outcomes. Eur Urol. 2012;61:664–75.
Krimphove MJ, Theissen LH, Cole AP, Preisser F, Mandel PC, Chun FKH. Performance and Impact of prostate specific membrane antigen-based diagnostics in the management of men with biochemical recurrence of prostate cancer and its role in salvage lymph node dissection. World J Mens Health. 2019. https://doi.org/10.5534/wjmh.180133.
Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2017;71:618–29.
Shariat SF, Roudier MP, Wilcox GE, Kattan MW, Scardino PT, Vessella RL, et al. Comparison of immunohistochemistry with reverse transcription-PCR for the detection of micrometastatic prostate cancer in lymph nodes. Cancer Res. 2003;63:4662–70.
Miyake H, Hara I, Kurahashi T, Inoue TA, Eto H, Fujisawa M. Quantitative detection of micrometastases in pelvic lymph nodes in patients with clinically localized prostate cancer by real-time reverse transcriptase-PCR. Clin Cancer Res. 2007;13:1192–7.
Kusuda Y, Miyake H, Kurahashi T, Fujisawa M. Assessment of optimal target genes for detecting micrometastases in pelvic lymph nodes in patients with prostate cancer undergoing radical prostatectomy by real-time reverse transcriptase-polymerase chain reaction. Urol Oncol. 2013;31:615–21.
Heck MM, Retz M, Bandur M, Souchay M, Vitzthum E, Weirich G, et al. Topography of lymph node metastases in prostate cancer patients undergoing radical prostatectomy and extended lymphadenectomy: results of a combined molecular and histopathologic mapping study. Eur Urol. 2014;66:222–9.
Heck MM, Retz M, Bandur M, Souchay M, Vitzthum E, Weirich G, et al. Molecular lymph node status for prognostic stratification of prostate cancer patients undergoing radical prostatectomy with extended pelvic lymph node dissection. Clin Cancer Res. 2018;24:2342–9.
Cancer Genome Atlas Research N. The molecular taxonomy of primary prostate cancer. Cell. 2015;163:1011–25.
Shariat SF, Kattan MW, Erdamar S, Nguyen C, Scardino PT, Spencer DM, et al. Detection of clinically significant, occult prostate cancer metastases in lymph nodes using a splice variant-specific rt-PCR assay for human glandular kallikrein. J Clin Oncol. 2003;21:1223–31.
Offermann A, Roth D, Hupe MC, Hohensteiner S, Becker F, Joerg V, et al. TRIM24 as an independent prognostic biomarker for prostate cancer. Urol Oncol. 2019;37:576.e1–e10.
Heck MM, Thalgott M, Schmid SC, Oh WK, Gong Y, Wang L, et al. A 2-gene panel derived from prostate cancer-enhanced transcripts in whole blood is prognostic for survival and predicts treatment benefit in metastatic castration-resistant prostate cancer. Prostate. 2016;76:1160–8.
D’Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, Broderick GA, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998;280:969–74.
McShane LM, Altman DG, Sauerbrei W, Taube SE, Gion M, Clark GM, et al. REporting recommendations for tumour MARKer prognostic studies (REMARK). Br J Cancer. 2005;93:387–91.
Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999;281:1591–7.
Boorjian SA, Thompson RH, Tollefson MK, Rangel LJ, Bergstralh EJ, Blute ML, et al. Long-term risk of clinical progression after biochemical recurrence following radical prostatectomy: the impact of time from surgery to recurrence. Eur Urol. 2011;59:893–9.
Attard G, Parker C, Eeles RA, Schroder F, Tomlins SA, Tannock I, et al. Prostate cancer. Lancet. 2016;387:70–82.
Ferrari AC, Stone NN, Kurek R, Mulligan E, McGregor R, Stock R, et al. Molecular load of pathologically occult metastases in pelvic lymph nodes is an independent prognostic marker of biochemical failure after localized prostate cancer treatment. J Clin Oncol. 2006;24:3081–8.
Ko CJ, Huang CC, Lin HY, Juan CP, Lan SW, Shyu HY, et al. Androgen-induced TMPRSS2 activates matriptase and promotes extracellular matrix degradation, prostate cancer cell invasion, tumor growth, and metastasis. Cancer Res. 2015;75:2949–60.
Wang Z, Wang Y, Zhang J, Hu Q, Zhi F, Zhang S, et al. Significance of the TMPRSS2: ERG gene fusion in prostate cancer. Mol Med Rep. 2017;16:5450–8.
Vaarala MH, Porvari K, Kyllonen A, Lukkarinen O, Vihko P. The TMPRSS2 gene encoding transmembrane serine protease is overexpressed in a majority of prostate cancer patients: detection of mutated TMPRSS2 form in a case of aggressive disease. Int J Cancer. 2001;94:705–10.
Uhlen M, Zhang C, Lee S, Sjöstedt E, Fagerberg L, Bidkhori G, et al. A pathology atlas of the human cancer transcriptome. Science. 2017;357. https://doi.org/10.1126/science.aan2507.
Acknowledgements
We thank Monika Moissl for her support in the laboratory with molecular LN analysis. Also, we thank all patients for their participation in the study. This work was funded by the German Wilhelm-Sander Foundation (grant no. 2010.011.1; MMH, MR, and RN) and the Reinhard-Nagel Foundation (MMH) of the German Association of Urology. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lunger, L., Retz, M., Bandur, M. et al. KLK3 and TMPRSS2 for molecular lymph-node staging in prostate cancer patients undergoing radical prostatectomy. Prostate Cancer Prostatic Dis 24, 362–369 (2021). https://doi.org/10.1038/s41391-020-00283-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41391-020-00283-3
This article is cited by
-
Remodelling of the tumour microenvironment by the kallikrein-related peptidases
Nature Reviews Cancer (2022)
-
On the probability of lymph node negativity in pN0-staged prostate cancer—a theoretically derived rule of thumb for adjuvant needs
Strahlentherapie und Onkologie (2022)
-
Clinical significance of STEAP1 extracellular vesicles in prostate cancer
Prostate Cancer and Prostatic Diseases (2021)
-
Prostate cancer hijacks the microenvironment
Nature Cell Biology (2021)
