
Abstract
The efficacy of programmed cell death protein 1 (PD-1) blockade in metastatic triple-negative breast cancer (TNBC) is low1,2,3,4,5, highlighting a need for strategies that render the tumor microenvironment more sensitive to PD-1 blockade. Preclinical research has suggested immunomodulatory properties for chemotherapy and irradiation6,7,8,9,10,11,12,13. In the first stage of this adaptive, non-comparative phase 2 trial, 67 patients with metastatic TNBC were randomized to nivolumab (1) without induction or with 2-week low-dose induction, or with (2) irradiation (3 × 8 Gy), (3) cyclophosphamide, (4) cisplatin or (5) doxorubicin, all followed by nivolumab. In the overall cohort, the objective response rate (ORR; iRECIST14) was 20%. The majority of responses were observed in the cisplatin (ORR 23%) and doxorubicin (ORR 35%) cohorts. After doxorubicin and cisplatin induction, we detected an upregulation of immune-related genes involved in PD-1–PD-L1 (programmed death ligand 1) and T cell cytotoxicity pathways. This was further supported by enrichment among upregulated genes related to inflammation, JAK–STAT and TNF-α signaling after doxorubicin. Together, the clinical and translational data of this study indicate that short-term doxorubicin and cisplatin may induce a more favorable tumor microenvironment and increase the likelihood of response to PD-1 blockade in TNBC. These data warrant confirmation in TNBC and exploration of induction treatments prior to PD-1 blockade in other cancer types.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


Data availability
DNA and RNA sequencing data have been deposited in the European Genome-phenome Archive (EGA) under accession number EGAS0001003535 and will be made available from the corresponding author on reasonable request. Data requests will be reviewed by the institutional review board of the NKI and applying researchers will need to sign a data access agreement with the NKI after approval. The TCR sequencing data are available from Adaptive Biotechnologies, but restrictions apply to their availability. However, data are available from the corresponding author on reasonable request and with permission of Adaptive Biotechnologies.
Change history
17 June 2019
In the version of this article originally published, there was an error in Fig. 3j. A label on the heatmap read “TGF-α signaling via NF-κB”. It should have read “TNF-α signaling via NF-κB”. The error has been corrected in the HTML and PDF versions of this article.
References
Adams, S. et al. Pembrolizumab monotherapy for previously treated metastatic triple-negative breast cancer: cohort A of the phase 2 KEYNOTE-086 study. Ann. Oncol. https://doi.org/10.1093/annonc/mdy517 (2018).
Nanda, R. et al. Pembrolizumab in patients with advanced triple-negative breast cancer: phase Ib KEYNOTE-012 study. J. Clin. Oncol. 34, 2460–2467 (2016).
Emens, L. A. et al. Long-term clinical outcomes and biomarker analyses of atezolizumab therapy for patients with metastatic triple-negative breast cancer: a phase 1 study. JAMA Oncol. 5, 74–82 (2018).
Dirix, L. Y. et al. Avelumab, an anti-PD-L1 antibody, in patients with locally advanced or metastatic breast cancer: a phase 1b JAVELIN solid tumor study. Breast Cancer Res. Treat. 167, 671–686 (2018).
Schmid, P. et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N. Engl. J. Med. 380, 987–988 (2018).
Demaria, S. et al. Ionizing radiation inhibition of distant untreated tumors (abscopal effect) is immune mediated. Int. J. Radiat. Oncol. Biol. Phys. 58, 862–870 (2004).
Vanpouille-Box, C. et al. DNA exonuclease Trex1 regulates radiotherapy-induced tumour immunogenicity. Nat. Commun. 8, 15618 (2017).
Scurr, M. et al. Low-dose cyclophosphamide induces antitumor T-cell responses, which associate with survival in metastatic colorectal cancer. Clin. Cancer Res. 23, 6771–6780 (2017).
de Biasi, A. R., Villena-Vargas, J. & Adusumilli, P. S. Cisplatin-induced antitumor immunomodulation: a review of preclinical and clinical evidence. Clin. Cancer Res. 20, 5384–5391 (2014).
Wan, S. et al. Chemotherapeutics and radiation stimulate MHC class I expression through elevated interferon-β signaling in breast cancer cells. PLoS ONE 7, e32542 (2012).
Alizadeh, D. et al. Doxorubicin eliminates myeloid-derived suppressor cells and enhances the efficacy of adoptive T-cell transfer in breast cancer. Cancer Res. 74, 104–118 (2014).
Sistigu, A. et al. Cancer cell-autonomous contribution of type I interferon signaling to the efficacy of chemotherapy. Nat. Med. 20, 1301–1309 (2014).
Casares, N. et al. Caspase-dependent immunogenicity of doxorubicin-induced tumor cell death. J. Exp. Med. 202, 1691–1701 (2005).
Seymour, L. et al. iRECIST: guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 18, e143–e152 (2017).
O’Brien, K. M. et al. Intrinsic breast tumor subtypes, race, and long-term survival in the Carolina Breast Cancer Study. Clin. Cancer Res. 16, 6100–6110 (2010).
den Brok, W. D. et al. Survival with metastatic breast cancer based on initial presentation, de novo versus relapsed. Breast Cancer Res. Treat. 161, 549–556 (2017).
Kassam, F. et al. Survival outcomes for patients with metastatic triple-negative breast cancer: implications for clinical practice and trial design. Clin. Breast Cancer 9, 29–33 (2009).
Adams, S. et al. Pembrolizumab monotherapy for previously untreated, PD-L1-positive, metastatic triple-negative breast cancer: cohort B of the phase 2 KEYNOTE-086 study. Ann. Oncol. https://doi.org/10.1093/annonc/mdy518 (2018).
Simon, R. Optimal two-stage designs for phase II clinical trials. Control. Clin. Trials 10, 1–10 (1989).
Kok, M. et al. Profound immunotherapy response in mismatch repair-deficient breast cancer. JCO Precis. Oncol. 1, 1–3 (2017).
Sørlie, T. et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl Acad. Sci. USA 98, 10869–10874 (2001).
Ayers, M. et al. IFN-γ-related mRNA profile predicts clinical response to PD-1 blockade. J. Clin. Invest. 127, 2930–2940 (2017).
Danaher, P. et al. Gene expression markers of tumor infiltrating leukocytes. J. Immunother. Cancer 5, 18 (2017).
Liberzon, A. et al. The Molecular Signatures Database (MSigDB) hallmark gene set collection. Cell Syst. 1, 417–425 (2015).
Bezzi, M. et al. Diverse genetic-driven immune landscapes dictate tumor progression through distinct mechanisms. Nat. Med. 24, 165–175 (2018).
Danaher, P., Warren, S. & Cesano, A. Development of gene expression signatures characterizing the tumor–immune interaction. J. Clin. Oncol. 36, 205 (2018).
Gu-Trantien, C. et al. CD4+ follicular helper T cell infiltration predicts breast cancer survival. J. Clin. Invest. 123, 2873–2892 (2013).
Adams, S. et al. Atezolizumab plus nab-paclitaxel in the treatment of metastatic triple-negative breast cancer with 2-year survival follow-up: a phase 1b clinical trial. JAMA Oncol. 5, 334–342 (2019).
Loibl, S. et al. Randomized phase II neoadjuvant study (GeparNuevo) to investigate the addition of durvalumab to a taxane-anthracycline containing chemotherapy in triple negative breast cancer (TNBC). J. Clin. Oncol. 36, 104 (2018).
Blank, C. U. et al. Neoadjuvant versus adjuvant ipilimumab plus nivolumab in macroscopic stage III melanoma. Nat. Med. 24, 1655–1661 (2018).
Forde, P. M. et al. Neoadjuvant PD-1 blockade in resectable lung cancer. N. Engl. J. Med. 378, 1976–1986 (2018).
Rizvi, N. A. et al. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 348, 124–128 (2015).
Van Allen, E. M. et al. Genomic correlates of response to CTLA-4 blockade in metastatic melanoma. Science 350, 207–211 (2015).
Samstein, R. M. et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat. Genet. 51, 202–206 (2019).
Molinero, L. et al. Molecular characterization of tumors from metastatic TNBC patients treated with atezolizumab (atezo). Cancer Res. 78, abstr. P2-09-13 (2018).
Davoli, T., Uno, H., Wooten, E. C. & Elledge, S. J. Tumor aneuploidy correlates with markers of immune evasion and with reduced response to immunotherapy. Science 355, eaaf8399 (2017).
Roh, W. et al. Integrated molecular analysis of tumor biopsies on sequential CTLA-4 and PD-1 blockade reveals markers of response and resistance. Sci. Transl Med. 9, eaah3560 (2017).
Rimm, D. L. et al. A prospective, multi-institutional, pathologist-based assessment of 4 immunohistochemistry assays for PD-L1 expression in non-small cell lung cancer. JAMA Oncol. 3, 1051–1058 (2017).
Zavalishina, L. et al. RUSSCO-RSP comparative study of immunohistochemistry diagnostic assays for PD-L1 expression in urothelial bladder cancer. Virchows Arch. 473, 719–724 (2018).
Eisenhauer, E. A. et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur. J. Cancer 45, 228–247 (2009).
Baselga, J. et al. Randomized phase II study of the anti-epidermal growth factor receptor monoclonal antibody cetuximab with cisplatin versus cisplatin alone in patients with metastatic triple-negative breast cancer. J. Clin. Oncol. 31, 2586–2592 (2013).
Singh, J. et al. Phase 2 trial of everolimus and carboplatin combination in patients with triple negative metastatic breast cancer. Breast Cancer Res. 16, R32 (2014).
O’Shaughnessy, J. et al. Iniparib plus chemotherapy in metastatic triple-negative breast cancer. N. Engl. J. Med. 364, 205–214 (2011).
Carey, L. A. et al. TBCRC 001: randomized phase II study of cetuximab in combination with carboplatin in stage IV triple-negative breast cancer. J. Clin. Oncol. 30, 2615–2623 (2012).
R Core Team R: a language and environment for statistical computing v3.3.2 (2018).
Cibulskis, K. et al. Sensitive detection of somatic point mutations in impure and heterogeneous cancer samples. Nat. Biotechnol. 31, 213–219 (2013).
Favero, F. et al. Sequenza: allele-specific copy number and mutation profiles from tumor sequencing data. Ann. Oncol. 26, 64–70 (2015).
Love, M. I., Hogenesch, J. B. & Irizarry, R. A. Modeling of RNA-seq fragment sequence bias reduces systematic errors in transcript abundance estimation. Nat. Biotechnol. 34, 1287–1291 (2016).
Nielsen, M., Lundegaard, C., Lund, O. & Kesmir, C. The role of the proteasome in generating cytotoxic T-cell epitopes: insights obtained from improved predictions of proteasomal cleavage. Immunogenetics 57, 33–41 (2005).
Kesmir, C., Nussbaum, A. K., Schild, H., Detours, V. & Brunak, S. Prediction of proteasome cleavage motifs by neural networks. Protein Eng. 15, 287–296 (2002).
Jurtz, V. et al. NetMHCpan-4.0: improved peptide–MHC class I interaction predictions integrating eluted ligand and peptide binding affinity data. J. Immunol. 199, 3360–3368 (2017).
Robinson, M. D., McCarthy, D. J. & Smyth, G. K. edgeR: a Bioconductor package for differential expression analysis of digital gene expression data. Bioinformatics 26, 139–140 (2010).
McCarthy, D. J., Chen, Y. & Smyth, G. K. Differential expression analysis of multifactor RNA-seq experiments with respect to biological variation. Nucleic Acids Res. 40, 4288–4297 (2012).
Efron, B. & Thisted, R. Estimating the number of unseen species: how many words did Shakespeare know? Biometrika 63, 435–447 (1976).
Subramanian, A. et al. Gene set enrichment analysis: a knowledge-based approach for interpreting genome-wide expression profiles. Proc. Natl Acad. Sci. USA 102, 15545–15550 (2005).
Gendoo, D. M. et al. Genefu: an R/Bioconductor package for computation of gene expression-based signatures in breast cancer. Bioinformatics 32, 1097–1099 (2016).
Carpenter, B. et al. Stan: a probabilistic programming language. J. Stat. Softw. 76, 1–32 (2017).
Joosse, S. A. et al. Prediction of BRCA1-association in hereditary non-BRCA1/2 breast carcinomas with array-CGH. Breast Cancer Res. Treat. 116, 479–489 (2009).
Schouten, P. C. et al. Robust BRCA1-like classification of copy number profiles of samples repeated across different datasets and platforms. Mol. Oncol. 9, 1274–1286 (2015).
Vollebergh, M. A. et al. An aCGH classifier derived from BRCA1-mutated breast cancer and benefit of high-dose platinum-based chemotherapy in HER2-negative breast cancer patients. Ann. Oncol. 22, 1561–1570 (2011).
Acknowledgements
We thank the patients and their families for participating in the study. We thank J. Foekema, M. Holtkamp, M. Delfos, J. van Zyl-de Jong and K. Kersten for their support in the care for patients. We thank S. Vanhoutvin for legal support. We thank the Core Facility of Molecular Pathology & Biobanking for their support in processing of samples. In addition, we acknowledge the Genomics Core Facility for their support regarding sequencing. We acknowledge J. Lips from Adaptive Biotechnologies for his support. We thank the scientific administration department, in particular L. Ruiter, for data management/monitoring. The Clinical Chemistry Department is thanked for their support in blood withdrawals. We thank H. Garner, M. van der Heijden and J. Stouthard for critical reading of the manuscript. We acknowledge D. Cullen, A. Evans, D. Zardavas and D. Feltquate of Bristol-Myers Squibb (BMS) for scientific input. We thank BMS/II-ON and the Dutch Cancer Society (NKI2015–7710, 10653 ALPE) for funding the study and a fellowship to M.K. (NKI2015–7542). Pink Ribbon (NKI2016–8214), the Breast Cancer Research Foundation (BCRF-17–188) and BMS/II-ON are thanked for the funding of the translational research. R.S. is supported by a grant from the Breast Cancer Research Foundation (BCRF-17–194).
Author information
Authors and Affiliations
Contributions
L.V. coordinated trial procedures, analyzed and interpreted clinical and translational data and wrote the manuscript with M.S., T.N.S., C.U.B. and M.K. M.S. performed and interpreted the bioinformatic analyses. H.M.H., K.K.v.d.V. and R.S. performed the histological scoring. K.S. performed the statistical analysis on the clinical data. M.d.M. was responsible for DNA and RNA isolations. I.N. provided input during work discussions. R.J.C.K. processed the raw DNA and RNA sequencing data. S. Warren and S. Ong were responsible for the NanoString nCounter assay experiments and analyses. T.G.W. and N.S.R. were responsible for initial screening and the patients treated with irradiation. F.L. revised the CT scans. P.C.S. adapted the BRCA1-like classifier and applied it to our data set. N.A.M.B. and L.V. performed and analyzed the cytokine assays. S.L.C.K. performed the prediction of neo-epitopes. D.P. was responsible for the double staining of CD4 and FOXP3. C.A.H.L. performed the majority of biopsies and assessment of the CT scans. E.v.W. and H.v.T. were involved in the statistical design. I.A.M.M. was the clinical projects manager involved in the trial. I.K. and S. Onderwater. were responsible for patient care. M.C., S. Wilgenhof, G.S.S., S.C.L. and M.K. included patients in the trial and were responsible for patient care. J.B.A.G.H. advised on the trial design. K.E.d.V. gave critical input and supervised the cytokine assays. L.F.A.W. supervised the bioinformatics analyses. G.S.S., S.C.L., C.U.B., T.N.S. and M.K. designed the trial. C.U.B., T.N.S. and M.K. made the experimental plan of investigation. All authors edited and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
L.V., M.S., H.M.H., K.S., K.K.v.d.V., M.d.M., I.N., R.J.C.K., T.G.W., N.S.R., F.L., N.A.M.B., S.L.C.K., D.P., C.A.H.L., E.v.W., H.v.T., I.A.M.M., I.K., S. Onderwater and S. Wilgenhof declare no competing interests. S.Warren reports employment and stockholdership of NanoString Technologies, an advisory role for Roche and being a former employee of Oncofactor Corp., outside the submitted work. S. Ong reports employment and stockholdership of NanoString Technologies. P.C.S. has a close relative employed by AstraZeneca. M.C. reports funding to the institute from BMS and Roche/Genentech, outside the submitted work. J.B.A.G.H. reports financial compensation to the NKI for advisory roles from Amgen, AZ, BMS, Bayer, MSD, Celsius Therapeutics, Gadeta, Immunocore, Seattle Genetics, Merck Serono, Sanofi, Roche, Neon therapeutics, Pfizer and Ipsen and NKI, and received grants from BMS, MSD, Novartis and Neon therapeutics, outside the submitted work. R.S. reports research funding from Merck, Roche and Puma, as well as travel funds from AstraZeneca, Roche, Merck and an advisory role for BMS, outside the scope of this work. K.E.d.V. reports research funding from Roche, outside the scope of this work. G.S.S. reports funding to the institute from AstraZeneca, Merck Sharp & Dohme, Novartis and Roche, outside the submitted work. L.F.A.W. reports receiving a commercial research grant from Genmab. S.C.L. reports funding to the institute from Agendia, Amgen, AstraZeneca, BMS, Eurocept, Roche/Genentech, Tesaro and an advisory role for AstraZeneca, Bayer and IBM, outside the submitted work. T.N.S. is a consultant for Adaptive Biotechnologies, AIMM Therapeutics, Allogene Therapeutics, Amgen, Merus, Neon Therapeutics, Scenic Biotech; received grant or research support from Merck, BMS and Merck KGaA; is a stockholder in AIMM Therapeutics, Allogene Therapeutics, Neon Therapeutics and Neogene Therapeutics, all outside the submitted work. C.U.B. reports personal fees for advisory roles for MSD, BMS, Roche, GSK, Novartis, Pfizer, Lilly, Pierre Fabre and GenMab and grants from BMS, Novartis and NanoString, outside the submitted work. M.K. reports funding and a speaker’s fee to the institute from BMS and Roche and an unpaid advisory role for BMS, outside the submitted work.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 CONSORT diagram.
Flowchart for the allocation of subjects enrolled in the trial.
Extended Data Fig. 2 Clinical and other baseline parameters associated with response.
Boxplots represent the median, 25th and 75th percentiles and the vertical bars span the 5th and 95th percentiles. Statistical significance was tested with a two-tailed Mann–Whitney U-test (unadjusted P values). a, ORR per subgroup. Depicted is the ORR (CR + PR of n = 66) per subgroup. Cut-offs are set at the median for carcinoembryonic antigen (CEA), CA 15-3, sTIL and CD8. Statistical significance was determined by a two-sided Fisher’s exact test. *P < 0.05. WHO, WHO performance status. 1Patients with de novo metastatic disease at diagnosis were excluded (n = 8). b, PD-L1 expression on immune cells. c, PD-L1 expression on tumor cells. d, Serum levels of CEA. e, Correlation of CA 15-3 and CEA with tumor burden and the number of metastatic sites. Spearman correlation coefficients are depicted. Tumor burden was measured as the sum of all target lesions in millimeters; *P < 0.05; ***P < 0.001. f, LDH levels. g, C-reactive protein (CRP) levels. h, Neutrophil counts. i, Lymphocyte counts. j, Neutrophil-to-lymphocyte ratio (NLR). k, Eosinophil counts. The dashed line indicates the detection limit. l, Intratumoral TCR clonality. m, Percentage of intratumoral T cells by TCR sequencing. n, Intratumoral TCR repertoire diversity. o, TCR clonality in the peripheral blood. p, Percentage of T cells by TCR sequencing in the peripheral blood. q, TCR repertoire diversity in the peripheral blood. r, Non-synonymous tumor mutational burden (TMB). s, Predicted neo-epitopes.
Extended Data Fig. 3 Baseline PD-L1 expression.
a, PFS and PD-L1 expression on tumor cells. The Kaplan–Meier curve displays the proportion of patients free of progression, stratified by PD-L1 expression on tumor cells. A cut-off of 1% is used. The table lists the number of patients at risk. b, Overall survival and PD-L1 expression on tumor cells. The Kaplan–Meier curve displays overall survival, stratified by PD-L1 expression on tumor cells. A cut-off of 1% is used. c, PFS and PD-L1 expression on tumor-infiltrating immune cells. The Kaplan–Meier curve displays the proportion of patients free of progression, stratified by PD-L1 expression on tumor-infiltrating immune cells. A cut-off of 1% is used. d, Overall survival and PD-L1 expression on tumor-infiltrating immune cells. The Kaplan–Meier curve displays overall survival, stratified by PD-L1 expression on tumor-infiltrating immune cells. A cut-off of 1% is used. e, PFS and PD-L1 expression on tumor-infiltrating immune cells. The Kaplan–Meier curve displays the proportion of patients free of progression, stratified by PD-L1 expression on tumor-infiltrating immune cells. A cut-off of 5% is used. f, Overall survival and PD-L1 expression on tumor-infiltrating immune cells. The Kaplan–Meier curve displays overall survival, stratified by PD-L1 expression on tumor-infiltrating immune cells. A cut-off of 5% is used. g, PD-L1 expression on tumor-infiltrating immune cells and site of metastasis. PD-L1 expression per biopsy site at baseline is shown. Dots reflect the medians and whiskers reflect the interquartile ranges. IC, tumor-infiltrating immune cells; TC, tumor cells.
Extended Data Fig. 4 Baseline serum cytokine levels.
Cytokine levels were determined by a validated bead-based assay. Dots and whiskers represent medians and interquartile ranges, respectively. The dashed lines indicate the detection limit. a, IL-2 levels. IL-2 levels were detectable in five patients with clinical benefit and seven patients with progressive disease. b, IL-4 levels. IL-4 levels were detectable in 5 patients with clinical benefit and 11 patients with progressive disease. c, IL-6 levels. IL-6 levels were detectable in 13 patients with clinical benefit and 49 patients with progressive disease. d, IL-10 levels. IL-10 levels were detectable in 11 patients with clinical benefit and 41 patients with progressive disease. e, IL-17A levels. IL-17A levels were detectable in 12 patients with clinical benefit and 46 patients with progressive disease. f, IFN-γ levels. IFN-γ levels were detectable in 13 patients with clinical benefit and 47 patients with progressive disease. g, TNF-α levels. TNF-α levels were detectable in 11 patients with clinical benefit and 45 patients with progressive disease. h, Soluble Fas (sFas) levels. sFas levels were detectable in all tested patients. i, Granzyme A levels. Granzyme A levels were detectable in all tested patients. j, Granzyme B levels. Granzyme B levels were detectable in 5 patients with clinical benefit and 17 patients with progressive disease. k, Perforin levels. Perforin levels were detectable in all tested patients. l, Granulysin levels. Granulysin levels were detectable in all tested patients.
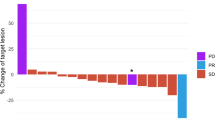
Extended Data Fig. 5 Anti-tumor activity of nivolumab.
a, Changes in target lesions over time, reflecting the depth and duration of response. Every line represents one patient, and every dot is one time point. The colors reflect induction treatment. The y axis was cut-off at 100% for illustration purposes. Dotted black lines indicate the response as described by RECIST1.1. b, Waterfall plot depicting the change in target lesions from baseline to post-induction. Every bar represents one patient and the colors correspond to induction treatment. The y axis was cut-off at 100% for illustration purposes. Dotted black lines indicate the response as described by RECIST1.1. c, ORR per cohort and according to lines of palliative treatment. The bars with no pattern depict the overall response rate in all patients, the bars with a dotted pattern depict the overall response rate in first-line-treated patients and the bars with a lined pattern depict the overall response rate in the second-to-fourth-line-treated patients. The numbers above the bars reflect the number of responding patients (CR + PR) over the total number of patients in that subgroup. d, Proportion of patients free of progression at 24 weeks. Measured from randomization according to RECIST1.1 (primary end point). e, Proportion of patients free of progression at 12 weeks. Measured from nivolumab initiation (including response evaluation performed at 14 weeks from randomization) according to RECIST1.1. f, Proportion of patients free of progression at 12 weeks. Measured from nivolumab initiation (including response evaluation performed at 14 weeks from randomization) according to iRECIST. g, Number of patients free of progression at 12 weeks in the first 10 included patients. Measured from nivolumab initiation (including response evaluation performed at 14 weeks from randomization) according to iRECIST. h, Trial design of TONIC stage 2. Patients are randomized between (1) induction treatment of 2 weeks with doxorubicin followed by anti-PD-1 or (2) start with anti-PD-1 without induction treatment.
Extended Data Fig. 6 TCR repertoire diversity during an ongoing anticancer response on nivolumab and changes observed after induction treatments.
a, TCR repertoire diversity on nivolumab treatment (biopsy three). TCR repertoire size was estimated using the Efron–Thisted method54 and represents the number of unique intratumoral clones. The boxes in boxplots represent the median and interquartile ranges and the whiskers represent the 5th and 95th percentiles. b, Fold change (FC) in the number of unique intratumoral TCR clones (TCR repertoire diversity) after induction treatment versus baseline (biopsy two versus biopsy one). Every dot represents one patient. Patients with clinical benefit are highlighted with a red dot. The dotted black line indicates no change. TCR repertoire size was estimated using the Efron–Thisted method54. The boxes in the boxplots represent the median and interquartile ranges and the whiskers represent the full range. Statistical significance was tested with a Kruskal–Wallis test for all groups. c, FC in the number of unique intratumoral TCR clones (TCR repertoire diversity) after nivolumab treatment versus baseline (biopsy three versus biopsy one). Every dot represents one patient. Patients with clinical benefit are highlighted with a red dot. The dotted black line indicates no change. TCR repertoire size was computed using the Efron–Thisted method54. The boxes in the boxplots represent the median and interquartile ranges and the whiskers represent the full range. Statistical significance was tested with a Kruskal–Wallis test for all groups followed by Dunn’s tests between the induction treatment groups and the control group (P values are adjusted).
Extended Data Fig. 7 Histological characteristics of tumors during an ongoing anticancer response on nivolumab and changes observed after induction treatments.
a, sTILs in on-nivolumab biopsies (biopsy three), as determined according to guidelines of the TIL working group on a H&E staining. The boxes in the boxplots represent the median and interquartile ranges, and the whiskers represent the 5th and 95th percentiles. Statistical significance was tested with a two-tailed Mann–Whitney U-test (unadjusted P value). b, CD8 cell count per mm2 in on-nivolumab biopsies (biopsy three). The boxes in the boxplots represent medians with interquartile ranges, and the whiskers span the 5th to 95th percentiles. Statistical significance was tested with a two-tailed Mann–Whitney U-test (unadjusted P value). c, sTILs per cohort. The boxes in the boxplots represent medians with interquartile ranges, and the whiskers span the 5th to 95th percentiles. Statistical significance was tested on paired biopsies with the Wilcoxon signed-rank test (two-tailed and unadjusted P value). d, CD8 cell count per mm2 per cohort. The boxes in the boxplots represent medians with interquartile ranges, and the whiskers span the 5th to 95th percentiles. Statistical significance was tested on paired biopsies with the Wilcoxon signed-rank test (two-tailed and unadjusted P value). e, Stromal CD4 per cohort. The percentage of CD4 of the total stromal area was assessed. The boxes in the boxplots represent medians with interquartile ranges, and the whiskers span the 5th to 95th percentiles. Statistical significance was tested on paired biopsies with the Wilcoxon signed-rank test (two-tailed and unadjusted P value). f, Stromal FOXP3 per cohort. The percentage of FOXP3 of the total stromal area was assessed. The boxes in the boxplots represent medians with interquartile ranges, and the whiskers span the 5th to 95th percentiles. Statistical significance was tested on paired biopsies with the Wilcoxon signed-rank test (two-tailed and unadjusted P value).
Extended Data Fig. 8 Bayesian hierarchical regression analysis of inflammation-related gene set FCs to investigate differences in upregulation between induction arms.
a, Plate model representation of the hierarchical model describing the FCs between baseline and post-induction. White-colored variables are inferred from the data using the model, and blue-colored variables are incorporated in extensions of the basic model. The boxes reflect repetition of the variables, Narms = 5 and Npatients varies between arms. Data were available for 38 patients. b, Distributions of posterior parameter estimates for the basic hierarchical regression model. The percentages in the vertical labels represent probabilities of exceeding the control arm (the proportion of the distribution above zero). c, Effect of the baseline inflammation score on the observed FC in the inflammation score. Shown in red is the conditional mean (linear regression) with the 95% confidence interval shaded gray. The intercept of this line is not explicitly included in the model as it is already implicitly modelled by the μ. d, Association between clinical response and the observed FC in the inflammation score. Red dots indicate the means. The boxes in the boxplots represent medians and interquartile ranges, and the whiskers span 1.5 times the interquartile range. e, Association between previous lines of palliative treatment and the observed FC in the inflammation score. Boxplots are as in d. f, Association between lymph node-only metastasis and the observed FC in the inflammation score. Boxplots are as in d. g, Distributions of posterior parameter estimates for the full hierarchical regression model including all considered covariates. Format as in b. The points indicate the medians, the red lines indicate the 10–90% percentiles and the black lines indicate the 2.5–97.5% percentiles. h, Robustness of coefficients with inclusion of extra covariates. Shown are the medians of the posterior parameter distributions with the 10th and 90th percentiles for 7 different models, including and excluding combinations of the non-induction arm covariates.
Extended Data Fig. 9 Treatment-induced changes in myeloid cell-related and CD4 cell-related gene signatures.
a, Heatmap of post-induction FCs in gene expression signatures23,26 (NanoString gene expression data) in post-induction samples (biopsy two) compared to baseline (biopsy one). Depicted is the log2 FC in the median gene expression of paired biopsies. Statistical significance (two-sided Wilcoxon signed-rank test; unadjusted P value) is highlighted with a black dot. b, Heatmap of on-nivolumab FCs in gene expression signatures23,26 (NanoString gene expression data) in samples taken on nivolumab (biopsy three) compared to baseline (biopsy one). Depicted is the log2 FC in the median gene expression of paired biopsies. Statistical significance (two-sided Wilcoxon signed-rank test; unadjusted P value) is highlighted with a black dot. c, GSEA of selected gene sets related to myeloid cells and CD4 T cells25,27, performed on whole-transcriptome RNA sequencing of pre-induction and post-induction samples (biopsy two compared to biopsy one). Cells are colored according to normalized enrichment scores, and Benjamini–Hochberg (false discovery rate (FDR))-corrected P values equaling or below 0.25 are highlighted with black dots. CD4FH, follicular helper CD4 T cells; CD4TIL, tumor-infiltrating CD4 T cells; MO MDSC, monocytic MDSC; PMN MDSC, polymorphonuclear MDSC.
Supplementary information
Supplementary Information
Supplementary Note and Supplementary Tables 1–6
Rights and permissions
About this article

Cite this article
Voorwerk, L., Slagter, M., Horlings, H.M. et al. Immune induction strategies in metastatic triple-negative breast cancer to enhance the sensitivity to PD-1 blockade: the TONIC trial. Nat Med 25, 920–928 (2019). https://doi.org/10.1038/s41591-019-0432-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41591-019-0432-4
This article is cited by
-
The promise and challenges of combination therapies with antibody-drug conjugates in solid tumors
Journal of Hematology & Oncology (2024)
-
Drug conjugates for the treatment of lung cancer: from drug discovery to clinical practice
Experimental Hematology & Oncology (2024)
-
Characterization of immunomodulating agents from Staphylococcus aureus for priming immunotherapy in triple-negative breast cancers
Scientific Reports (2024)
-
Neoadjuvant chemo-immunotherapy with camrelizumab plus nab-paclitaxel and cisplatin in resectable locally advanced squamous cell carcinoma of the head and neck: a pilot phase II trial
Nature Communications (2024)
-
Targeting immunogenic cell stress and death for cancer therapy
Nature Reviews Drug Discovery (2024)
