
Abstract
Study design:
Each participant completed two submaximal, perceptually guided arm crank exercise tests and a graded exercise test (GXT) to volitional exhaustion.
Objective:
To assess the validity of a submaximal, perceptually guided exercise test to predict peak oxygen uptake (V̇O2peak) during arm cranking in paraplegic individuals.
Setting:
University of Jordan, Amman, Jordan.
Participants:
Eleven men with paraplegia as a result of poliomyelitis infection or spinal cord injury completed two submaximal perceptually guided exercise tests and an arm crank GXT to volitional exhaustion.
Main outcome measures:
The prediction of V̇O2peak was calculated by extrapolating the submaximal rating of perceived exertion (RPE) and V̇O2 values by linear regression to RPE20.
Results:
There were no significant differences between measured and predicted V̇O2peak from the three submaximal ranges of the RPE (that is, 9–13, 9–15 and 9–17) when extrapolated to RPE20 during both perceptually guided exercise tests (all P>0.05). However, the second perceptually guided exercise tests provided a more accurate prediction of V̇O2peak as reflected by narrower 95% limits of agreement and higher intraclass correlation coefficients.
Conclusion:
This study has shown that V̇O2peak may be predicted with reasonable accuracy from a perceptually guided exercise test, especially after a full familiarization trial.
Similar content being viewed by others
Introduction
Maximal oxygen uptake (V̇O2max) is the highest rate of oxygen that a person can take up and utilize during exercise involving large muscle groups.1 It is considered by most physiologists as the best indicator of cardiovascular and respiratory fitness.2 It has also been indicated that V̇O2max is an independent predictor of death in patients with heart disease.3 For reasons of cost and time, it is not always feasible to measure the V̇O2max. Therefore, on the basis of the strong linear relationship between heart rate (HR) and V̇O2, submaximal HR values are usually used to predict V̇O2max by extrapolating these values to age-predicted maximal heart rate. However, individuals with high spinal cord injury (spinal cord injury >T6) have an abnormal HR response because of their injury. This may in turn affect the maximal heart rate and consequently the ability to use age-predicted maximal heart rate to predict V̇O2max.
The Borg 6–20 Rating of Perceived Exertion (RPE) Scale4 is a widely accepted means of assessing the sensation of effort during exercise. The normal practice is to ask the person exercising to rate how hard the exercise feels while performing it. This procedure is frequently referred to as estimation, which is a passive process in which the RPE is free to vary. Conversely, the production procedure is an active process in which the RPE is prescribed and the individual produces an exercise intensity equating to a given RPE.
The RPE is a valid method of regulating exercise intensity using estimation-production procedures, whereby the exercise intensity is set according to a given RPE obtained from a previous exercise test in able-bodied and paraplegic individuals.5, 6 Eston et al.7 showed that it is possible to apply the RPE production procedure in the form of a perceptually guided, graded exercise test to estimate the V̇O2max by extrapolation of submaximal V̇O2 values elicited at RPEs of 9, 11, 13, 15 and 17 to RPE20 (that is, maximal RPE) on the Borg 6–20 RPE scale.
The validity of the perceptually guided exercise test to predict V̇O2max has been assessed in healthy low-fit individuals,8 across various exercise durations at each RPE level,9 in low-fit and physically active individuals,10 as well as in continuous and discontinuous protocols.7, 8, 11, 12 The prediction of V̇O2max from submaximal perceptually guided exercise bouts has been shown to be valid and facilitates a safer and more widely applicable means of exercise testing by eliminating higher exercise intensities (RPE >17) compared with the graded exercise test. A further advantage of this procedure is that individuals are given the autonomy to control the intensity of the exercise, and this may be an important factor for exercise adherence.
Individuals with spinal cord injury or spinal cord disease are generally less physically active compared with their able-bodied counterparts.13, 14 Depressive symptoms are often prevalent among these individuals,15 which in turn may lead to a lack of motivation to exercise.16 As such, use of a perceptually guided exercise test to estimate V̇O2peak at the beginning of an exercise program may be helpful from a motivational and self-autonomy perspective.
The aim of the current study was to assess whether V̇O2 values elicited during submaximal, perceptually guided exercise tests would provide an acceptable prediction of V̇O2peak (V̇O2peak is a preferred term for arm cranking ergometry due to the smaller muscle mass activated during this mode of exercise compared with leg cycling and running on a treadmill). We hypothesized that V̇O2 values elicited from submaximal, perceptually guided exercise bouts would provide an acceptable prediction of V̇O2peak when extrapolated to RPE20 during arm cranking in paraplegic persons.
Methods
Participants
Eleven paraplegic men provided written informed consent for the study. Their demographic characteristics and lesions are presented in Table 1. All participants were physically active and participated in sports such as basketball, weight lifting and wheelchair racing at professional and recreational levels. However, arm ergometry was not a familiar mode of exercise training for these individuals. On the first visit, the participants' weight (SECA, Hamburg, Germany) and blood pressure (Accoson, London, England) were measured. This study was conducted with institutional ethics approval from the faculty of physical education at the University of Jordan, where all the exercise tests were performed.
Procedures
Each participant completed two submaximal, perceptually guided exercise tests, separated by 48 h, to predict V̇O2peak. In addition, each participant performed an arm cranking GXT, separated by 48 h from the second perceptually guided exercise test, designed to establish V̇O2peak. In accordance with Morris et al.,11 the perceptually guided exercise tests preceded the GXT, in order to not give the participants a complete familiarization with the full RPE scale, as sedentary and clinical populations may not experience this in real-life situations. All participants were recommended to avoid moderate and vigorous exercise in the days before and between the exercise tests, which were performed on a Lode arm ergometer (Lode, B.V. Medical Technology, Groningen, the Netherlands). The midpoint of the ergometer was set at shoulder level and the distance was set to allow a slight flexion in the elbow when the arm was extended. The resistance on the ergometer was manipulated using the Lode Workload Programmer, accurate to ±1 W, which was independent of pedal cadence. Participants were asked to keep the pedal cadence at 60 r.p.m.
On-line respiratory gas analysis occurred every 10 s throughout each exercise test by means of an automatic gas calibrator system (Cortex Metalyzer II, Biophysik, Leipzig, Germany). Expired air was collected using a facemask to allow the participants to report their RPE during the GXT and to direct the tester to increase or decrease the power output (PO) to satisfy the prescribed RPE levels during the perceptually guided tests. The system was calibrated before each exercise test using a 3-l syringe for volume calibration and ambient air, according to the manufacturer's guidelines. Heart rate was recorded continuously using a wireless chest strap telemetry system (Polar Electro T31, Kempele, Finland). All physiological (that is, HR, oxygen uptake (V̇O2), ventilation (V̇E) and respiratory exchange ratio) and physical (PO and time) variables were kept out of sight during all exercise tests.
Measures
The Borg 6–20 RPE scale
Participants were given standardized instructions on how to report their overall and peripheral feelings of exertion before the GXT and how to use the overall RPE to regulate the exercise intensity during the perceptually guided exercise tests.4 Questions regarding the scale were answered before exercise commenced. Participants reported their overall and peripheral feeling of exertion in the remaining 20 s of each stage during the GXT and at the completion of the exercise test.
Perceptually guided exercise tests
In accordance with previous research,7, 8, 9, 10 participants were asked to exercise for 3 min at exercise intensities equal to 9, 11, 13, 15 and 17 on the Borg 6–20 RPE Scale during the first perceptually guided exercise test. Increments of 10 W were used to increase the work rate between the prescribed RPE levels. If more resistance was needed, 5- and 3-W increments were used until the target RPE level was achieved. Participants were asked to feel free to ask the experimenter to amend the exercise intensity at any point during the 3-min stages to equate to their feeling of exertion at the prescribed RPE during each stage. Procedures for the second perceptually guided exercise were identical and aimed to assess whether the prediction of V̇O2peak would improve with practice.
Graded exercise test
Each participant completed an arm crank GXT to establish V̇O2peak. After a 3-min warm-up at 0 W, the exercise test started at 30 W, and increased by 15 W every 2 min until the participant reached volitional exhaustion or was unable to maintain the required pedal cadence. All participants were verbally encouraged to continue as long as possible. Participants were asked to report their overall and peripheral RPE during the last 20 s of each stage and at the completion of the exercise. If the participant completed 1 min at least during the last stage, it was considered to be the peak PO (POpeak), and the highest mean of V̇O2 recorded during the last 20 s of each stage was considered as the V̇O2peak.
Data analysis
The mean V̇O2 values recorded during the last 20 s of the third minute at RPEs of 9, 11, 13, 15 and 17 during the perceptually guided exercise tests were regressed against the corresponding RPE in a linear regression analysis for each participant. Individual linear regression analyses using the submaximal V̇O2 values elicited in the RPE ranges RPE 9–13, 9–15 and 9–17 were then extrapolated to the theoretical maximal RPE (RPE20) on the Borg 6–20 RPE scale to predict V̇O2peak (Figure 1). A series of paired sample t-tests were used to compare predicted and measured V̇O2peak from the three RPE ranges (that is, 9–13, 9–15 and 9–17). A series of paired sample t-tests were also used to compare %PO and %V̇O2 values observed at RPEs of 9, 11, 13, 15 and 17 between the two perceptually guided tests.

V̇O2 values elicited at RPEs of 9, 11 and 13 extrapolated to RPE20 on the Borg 6–20 RPE scale to predict V̇O2peak for participant number 3.
Bland and Altman17 95% limits of agreement (LoA) analysis quantified the agreement (bias±1.96 × s.d. difference) between measured and predicted V̇O2peak for each RPE range. Data were checked for heteroscedasticity by conducting a Pearson correlation analysis between the difference of measured and predicted V̇O2peak scores and the average of the two measurement scores before applying LoA analysis as recommended.17 Intraclass correlation coefficients were also calculated using a one-way random model to quantify the relationship between predicted and measured values.
Results
Descriptive statistics for peak values observed at the termination of GXT
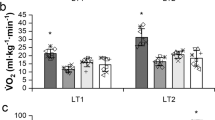
Peak values observed at the termination of the GXT for physiological (that is, V̇O2, HR, ventilation (V̇E) and respiratory exchange ratio), physical (PO) and perceptual (overall RPE (RPEo) and peripheral RPE (RPEp)) variables are reported in Table 1.
Measured vs predicted V̇O2peak
All measured and predicted V̇O2peak values were normally distributed (P>0.05) using Shapiro–Wilk statistics. Measured and predicted V̇O2peak values from the three RPE ranges (that is, 9–13, 9–15 and 9–17) when extrapolated to RPE20 from both perceptually guided exercise tests are reported in Table 2.
There was no significant difference between measured and predicted V̇O2peak from RPEs 9 to 15 (t(10)=0.6, P=0.583) and from RPEs 9 to 17 (t(10)=0.5, P=0.633), but the difference approached significance from RPEs 9 to 13 (t(10)=2.2, P=0.054) during the first perceptually guided test. A similar analysis showed no significant difference between measured and predicted V̇O2peak from RPEs 9 to 13 (t(10)=0.2, P=0.843), RPEs 9 to 15 (t(10)=0.3, P=0.781) and RPEs 9 to 17 (t(10)=0.4, P=0.687) when extrapolated to RPE20 during the second perceptually guided test.
PO and V̇O2 observed at RPEs of 9, 11, 13, 15 and 17
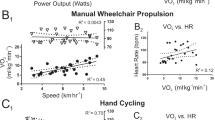
PO increased linearly as a function of RPE during the two perceptually guided tests (Figure 2). The V̇O2 showed a similar pattern during both perceptually guided tests.

PO achieved at RPEs of 9, 11, 13, 15 and 17 during the first perceptually guided test (P1) and the second perceptually guided test (P2). Values are mean±s.d.
There were no significant differences in %PO observed at RPEs of 9, 11, 13, 15 and 17 between the two perceptually guided tests (All P>0.05). However, proportions of PO tended to be higher (∼1 to ∼4%) during the second perceptually guided test. A similar analysis revealed no significant difference in %V̇O2 observed at RPEs of 9, 11, 15 and 17 between the first and second perceptually guided tests. However, the %V̇O2peak observed at RPE 13 was higher during the second perceptually guided test (t(10)=2.6, P=0.028) and tended to be higher at RPEs of 15 and 17 during the second test.
Analysis of the consistency of the predictions of V̇O2peak
LoA and intraclass correlation coefficients between measured and predicted V̇O2peak from the three RPE ranges during both trials are presented in Table 3. Figure 3 shows LoA between measured and predicted V̇O2peak from RPEs 9 to 13 during the second perceptually guided test.

The 95% limits of agreement (bias±1.96 × SDdiff, ml kg−1 min−1) for measured VO2peak and predicted VO2peak from RPEs 9–13 during the second perceptually guided exercise test.
Discussion
This study showed very strong linear relationships between the RPE and V̇O2 values elicited from the GXT for the first and second perceptually guided tests (all R2⩾0.98, when reconverting the mean of Fisher Zr values to their corresponding R2). This finding is in accordance with previous research, which used a perceptually guided exercise test to predict V̇O2max in healthy, able-bodied individuals during leg cycling.7, 8, 9
There were no significant differences between measured and predicted V̇O2peak values from the three RPE ranges (that is, RPEs 9–13, 9–15 and 9–17) when extrapolated to RPE20 from the two perceptually guided exercise tests. These findings are in agreement with previous research by Eston et al.7, 9 The current study shows that the high RPE range (that is, RPE 9–17) may be excluded from the second perceptually guided test without loss of accuracy in predicting V̇O2peak. This is an important application for sedentary individuals and for clinical populations,12, 18 although these observations are not in agreement with previous observations. Eston et al.8 observed lower predicted V̇O2max values from three production trials when an RPE of 17 was excluded. It should be borne in mind that all participants in this study were physically active, with some competing at the national level (for example, participant number 5 was a national level wheelchair racer). It is possible that the participants' familiarity with regular exercise in this study may affect their ability to perceptually regulate specific intensities according to a given, prescribed RPE. In this regard, Faulkner et al.,10 observed that able-bodied, physically active individuals showed less variability in reproducing a given exercise intensity at prescribed RPEs across several trials.
Nevertheless, it should be noted that, despite the nonsignificant differences between predicted and actual V̇O2peak from the three RPE ranges, LoA and intraclass correlation coefficient analysis indicated that the prediction of V̇O2peak was more accurate when estimated from the higher perceptual ranges (that is, RPEs 9–17) during the first perceptually guided test (Table 3). The second perceptually guided test also provided a more accurate prediction of V̇O2peak as reflected by the closer measured and predicted V̇O2peak values, narrower LoA and higher intraclass correlation coefficients (Tables 2 and 3).
This study shows the importance of using LoA to assess the agreement between the two methods of measuring the V̇O2peak. For instance, it seems from using the means and s.d. alone that the prediction of V̇O2peak is very accurate, especially when estimated from the second production trial. However, when LoA was used to assess the accuracy of predicted V̇O2peak against the measured value, there was a margin error of ±6 ml kg−1 min−1 (20%) between measured and predicted V̇O2peak for the three ranges of RPE.
In this study, participants exercised at higher %V̇O2peak at RPEs of 9 (40%) and 11 (50%) compared with previous studies, which utilized a perceptually guided approach.7, 8, 10 This might be attributed to the lower mechanical efficiency during arm cranking compared with leg cycling as a result of recruiting additional muscles for stabilizing the torso and from static work of some muscle groups, which do not contribute to the external work rate.19, 20
In conclusion, this study has shown a very strong linear relationship between the RPE and V̇O2 during perceptually guided exercise tests. The results provide encouraging evidence that V̇O2peak may be estimated with reasonable accuracy from submaximal V̇O2 values elicited during a perceptually guided exercise test, especially after a full familiarization trial. The results also imply that the higher RPE range (that is, RPEs 9–17) can be eliminated with little loss of accuracy in the prediction of V̇O2peak.
References
Åstrand PO, Rodahl K, Dahl HA, StrØmme SB . Textbook of Work Physiology: Physiological Bases of Exercise. 4th edn. Human Kinetics: Champaign, IL, 2003.
American college of sports medicine. ACSM's Guidelines for Exercise Testing and Prescription. 8th edn. Lippincott, Williams & Wilkins: Philadelphia, 2010.
Kavanagh T, Mertens DJ, Hamm LF, Beyene J, Kennedy J, Corey P et al. Prediction of long-term prognosis in 12169 men referred for cardiac rehabilitation. Circulation 2002; 106: 666–671.
Borg G . Borg's Perceived exertion and pain scales. Human Kinetics: Champaign, IL, 1998.
Eston RG, Davies BL, Williams JG . Use of perceived effort ratings to control exercise intensity in young healthy adults. Eur J Appl Physiol 1987; 56: 222–224.
Goosey-Tolfrey V, Lenton J, Goddard J, Oldfield V, Tolfrey K, Eston R . Regulating intensity using perceived exertion in spinal cord-injured participants. Med Sci Sports Exerc 2010; 42: 608–613.
Eston RG, Lamb KL, Parfitt G, King N . The validity of predicting maximal oxygen uptake from a perceptually-regulated graded exercise test. Eur J Appl Physiol 2005; 94: 221–227.
Eston RG, Lambrick D, Sheppard K, Parfitt G . Prediction of maximal oxygen uptake in sedentary males from a perceptually regulated, sub-maximal graded exercise test. J Sports Sci 2008; 26: 131–139.
Eston RG, Faulkner JA, Mason EA, Parfitt G . The validity of predicting maximal oxygen uptake from perceptually regulated graded exercise tests of different durations. Eur J Appl Physiol 2006; 97: 535–541.
Faulkner J, Parfitt G, Eston R . Prediction of maximal oxygen uptake from the ratings of perceived exertion and heart rate during a perceptually-regulated sub-maximal exercise test in active and sedentary participants. Eur J Appl Physiol 2007; 101: 397–407.
Morris M, Lamb K, Cotterrell D, Buckley J . Predicting maximal oxygen uptake via a perceptually regulated exercise test (PRET). J Exerc Sci Fit 2009; 2: 122–128.
Morris M, Lamb KL, Hayton J, Cotterrell D, Buckley J . The validity and reliability of predicting maximal oxygen uptake from a treadmill-based sub-maximal perceptually regulated exercise test. Eur J Appl Physiol 2010; 109: 983–988.
Collins EG, Gater D, Kiratli J, Butler J, Hanson K, Langbein E . Energy cost of physical activities in persons with spinal cord injury. Med Sci Sports Exerc 2010; 42: 691–700.
Owen RR, Jones D . Polio residuals clinic: conditioning exercise program. Orthopedics 1985; 8: 882–883.
Bombardier CH, Richards S, Krause JS, Tulsky D, Tate DG . Symptoms of major depression in people with spinal cord injury: implications for screening. Arch Phys Med Rehabil 2004; 85: 1749–1756.
Birk TJ . Polio and post-polio syndrome. In: Durstine JL, Moore GE, Painter PL. Roberts SO. (eds). ACSM's Exercise Management for Persons with Chronic Diseases and Disabilities, 3rd edn. Human Kinetics: Champaign, IL, 2009, 327–335.
Bland JM, Altman DG . Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: 307–310.
Coquart JBJ, Eston RG, Grosbois J-M, Lemaire C, Dubart A-E, Luttenbacher D-P, et al. Prediction of peak oxygen uptake from age and power output at RPE 15 in obese women. Eur J Appl Physiol 2010; 110: 645–649.
Eston RG, Brodie DA . Responses to arm and leg ergometry. Br J Sport Med 1986; 20: 4–6.
McArdle WD, Katch FI, Katch VL . Exercise physiology energy, nutrition, and human performance. 6th edn. Lippincott Williams & Wilkins: Baltimore, 2007.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Al-Rahamneh, H., Eston, R. The validity of predicting peak oxygen uptake from a perceptually guided graded exercise test during arm exercise in paraplegic individuals. Spinal Cord 49, 430–434 (2011). https://doi.org/10.1038/sc.2010.139
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.139
Keywords
This article is cited by
-
The ability of heart rate or perceived exertion to predict oxygen uptake varies across exercise modes in persons with tetraplegia
Spinal Cord (2021)
-
Submaximal, Perceptually Regulated Exercise Testing Predicts Maximal Oxygen Uptake: A Meta-Analysis Study
Sports Medicine (2016)
-
Validity of a perceptually-regulated step test protocol for assessing cardiorespiratory fitness in healthy adults
European Journal of Applied Physiology (2016)
-
Validity of Submaximal Step Tests to Estimate Maximal Oxygen Uptake in Healthy Adults
Sports Medicine (2016)
-
Prediction of one-repetition maximum from submaximal ratings of perceived exertion in older adults pre- and post-training
Aging Clinical and Experimental Research (2015)
