
Key Points
-
Flumazenil does not completely reverse all aspects of conscious sedation at clinical doses.
-
Patients who have been reversed should not be prematurely released into an unmonitored environment or discharged home early.
-
Because of its shorter half-life, patients may show some residual sedation, after flumazenil administration
-
Patients and their escorts still need full verbal and written post-operative instructions in the same manner as those patients who have not been reversed.
Abstract
Objective: To study the post-operative cognitive and psychomotor recovery from midazolam conscious sedation, after reversal with the benzodiazepine antagonist flumazenil over a prolonged recovery period.
Design: A prospective, double-blind, randomised, crossover trial.
Setting: Out-patient Sedation Department, Newcastle Dental Hospital and School
Method: Eighteen patients, ASA I or II, received midazolam on two separate occasions to undergo equivalent dental treatment. Following treatment patients were reversed with intravenous flumazenil or saline (placebo) at alternate appointments. Assessment of mood and cognitive function was undertaken using a highly sensitive and specific computerised battery of cognitive tests administered by telephone. Cognitive and psychomotor tests were administered prior to sedation and every hour for 6 hours post reversal.
Results: Results indicated no significant effect of flumazenil on simple reaction time and choice reaction time but did show a trend of reversing the effects of midazolam on numeric working memory and word recognition.
Conclusion: The cognitive and psychomotor effects of the sedation were not fully reversed by flumazenil. Cognitive impairments were still present up to 6 hours post-reversal, despite patients appearing clinically more alert. This has important implications for treatment protocols and discharge instructions.
Similar content being viewed by others

Main
Midazolam forms the mainstay of intravenous sedation for dental procedures in the UK. It is an effective and safe sedative if used by trained personnel, in proper facilities, on carefully selected patients.1
The effect of midazolam on cognitive and psychomotor function is well established.2 More recently Thompson et al.3 concluded that midazolam administration produces severe cognitive impairments, not only in the ability to both detect and process information but also in recalling specific aspects of information. The consequence of this is that patients will not recall information given during treatment. This may be good as patients will not recall the dental treatment itself but could be detrimental if they cannot recall specific instructions given to them.
The safety of midazolam sedation has been significantly improved by the availability of the benzodiazepine antagonist flumazenil. Flumazenil is not totally devoid of intrinsic actions but its main effect is to reverse benzodiazepine induced states.4 Its principle use in dentistry is for the emergency reversal of benzodiazepine induced conscious sedation. The usual dose is 0.2 mg administered in 15 seconds followed by increments of 0.1 mg every minute until full consciousness and normal cardio-respiratory function is regained.5 The drug inhibits the central effects of benzodiazepine agonists by competing at the benzodiazepine receptor. Reversal of the effects of midazolam does not appear to increase midazolam plasma levels.6 Various studies have demonstrated the rapidity of flumazenil reversal of midazolam sedation.7,8
Because of the differences in the plasma half-lives of midazolam and flumazenil (2.4 hours ± 0.8 and 51.3 minutes ± 0.85 respectively) there is a theoretical risk that following administration of flumazenil that the effects of midazolam may re-emerge several hours later. This is a potential problem if patients have been discharged home or have been transferred to an unmonitored environment. There is also a concern that the routine use of flumazenil may encourage a less rigorous control of the level of sedation, with a reliance on flumazenil to reverse any over sedation that may occur.9
Many studies have been published which have investigated the affects of flumazenil on the psychomotor recovery of patients and volunteers following use of benzodiazepines.8,10,11,12 However, most of these previous studies have been time limited and only tested for a few hours post sedation. Few studies investigating the effects of flumazenil on cognitive and psychomotor function have involved testing over a prolonged period. Most patients undergoing outpatient benzodiazepine sedation are discharged home within one to two hours of the end of sedation. It is therefore important, when considering the effects of a reversal agent, to assess recovery during the period when the patient is most at risk ie following discharge home.
The aim of this study therefore was to assess cognitive and psychomotor recovery over a prolonged recovery period, up to 6 hours post reversal with flumazenil. The study utilised a novel and highly discriminative computerised battery of cognitive and psychomotor tests, which were administered by telephone. This enabled the recovery of patients to be evaluated at home over a prolonged period after discharge. The ClinPhone.cdr® computerised assessment system has been specifically designed to evaluate the effects of novel compounds on the quality of cognitive functioning in volunteers and patients in all phases of clinical development. It has become the most widely used computerised assessment system in any area of clinical cognitive research.13 The system has been used worldwide in more than 300 trials to evaluate a diverse range of compounds but has never been used to test recovery after the reversal of midazolam sedation.
Contentment
There was an increase in self-rated contentment in both groups from baseline (Fig. 6). Although the flumazenil group was always ahead of the placebo group, only at the 6-hour time point did this become statistically significant.

Self-rated contentment. Mean (± SE) changes from baseline. *P < 0.05
Calmness
The results show a significant increase in calmness for both groups throughout the study (Fig. 7Table 1>). At no time was there any significant difference between the two groups.

Self-rated calmness. Mean (± SE) changes from baseline
Materials and methods
Study design
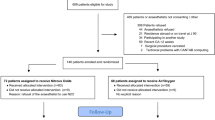
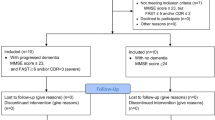
Eighteen subjects ASA I or II, aged between 18 and 60-years-old were recruited for the study. Any patients receiving any psychoactive medication were excluded. They required routine and equivalent dental treatment over two visits and had to have access to a touch-tone telephone at home to allow completion of the cognitive and psychomotor tests. The study was designed as a double blind, randomised, within subjects crossover trial. All patients recruited were those who require routine dental treatment under intravenous sedation because of a disproportionate level of dental anxiety.
Ethical approval was granted from the Joint Ethics Committee of the Newcastle and North Tyneside Health Authority, the University of Newcastle upon Tyne and the University of Northumbria.
Clinical technique
Each patient was allocated a patient identification number and an access code. They were given two treatment appointments, at least two weeks apart. At each appointment they were sedated with midazolam, administered by an indwelling venous cannula. At the first visit the patient was sedated to a level where dental treatment could be undertaken but during which verbal contact was maintained at all times. It is normal clinical practice to titrate the midazolam to the patient's response. This may vary within patients at different appointments. For the design and subsequent analysis of the study, at the second visit the patient was sedated with the same dose of midazolam as the first visit. At no time did this result in clinical under or over sedation.
At each visit the patient had an equivalent amount of restorative dental treatment with respect to duration, degree of complexity and local anaesthetic dose. The same clinician (KJF) performed the sedation and treatment on all patients to ensure equivalence. Monitoring of arterial oxygen saturation, respiration rate and pulse was undertaken continuously. Blood pressure was recorded every 10 minutes.
Upon completion of treatment (45 minutes after the last increment of midazolam), the sedation was reversed with either 4 ml of 0.9% saline (as placebo) or 4 ml of 0.1 mg/ml of flumazenil (total dose 0.4 mg). Doses of between 0.2 mg and 0.5 mg have been recommended for the reversal of sedation in patients receiving therapeutic doses of midazolam.14 A dose of 0.4 mg was selected, as this has been considered sufficient to reverse conscious sedation and represents a typical clinical dose used to reverse a patient.15,16 The 0.4 mg dose also approximates to the dose required in the receptor occupancy model, to reverse sedation without affecting the anticonvulsant and anxiolytic effects of the midazolam.14
The allocation of flumazenil or placebo was randomised using a computer generated random number list. A clinician independent of the operator, who had sole access to the unlock code, gave the agent (a clear colourless liquid in a 5 ml syringe) so as to maintain the blind nature of the study. The agent was titrated at 2 ml over 15 seconds followed by 1 ml every minute until a total of 4 ml was administered.
Cognitive and psychomotor test schedule
The CDR test battery was administered at the following time points:
-
1
Pre-sedation, immediately prior to the sedation session.
-
2
1 and 2 hours after the last increment of midazolam, prior to discharge, in a quiet enclosed recovery area with a touch tone telephone
-
3
At 3, 4, 5, 6 hours post sedation at the patients' home.
At the second appointment the dental procedure was matched as closely in degree and complexity as the procedure in the first appointment. Upon completion the patient was administered the alternate test agent to the one given in the previous session.
Cognitive tests administered via the telephone
The ClinPhone.cdr® system requires the patient to dial a free-phone number. A computer controlled recorded operator identifies the patient by asking them to enter their access code and PIN number which was supplied on a personalised patient information leaflet. The computer operator then administers a series of seven tests automatically. Each test is preceded by a full set of instructions. The clinician also advised the patient on the best way to position the telephone. This is important when the patient has to respond as quickly as possible.
This telephone system includes a number of measures specific to particular aspects of attention, working memory and long-term memory.
Cognitive and psychomotor test battery
The following tests were measured:
Mood Assessment. The first stage of the test was to assess the patients' self reported assessment of their mood in relation to alertness, contentment and calmness. The test was based on the visual analogue scale.17
Word presentation. At this stage a list of 15 words were read out to the participant, one word every second. The words were a mix of one, two and three syllables, and were matched for frequency, concreteness and imagery between sessions.
Attention and Memory. The second stage of the investigation was to assess attention and memory. The need for quick, accurate responses was stressed to the participants.
Simple Reaction Time (SRT). The subjects had to push the number 9 key as quickly as possible when they heard the word 'Yes'. The subjects were informed that speed was of importance. The word 'Yes' was stated 30 times. The reaction time was measured in milliseconds (ms).
Choice Reaction Time (CRT). The subjects had to push either the number 7 button to record a 'No' response or the number 9 key to record a 'Yes' response. The words 'Yes' and 'No' were stated 30 times in random order. The reaction time in milliseconds (ms) and accuracy of response in percentage terms was measured.
Numeric Working Memory (NWM). This test assessed the subjects ability to remember 5 digits. Five digits were presented singly at the rate of one every second for the participant to remember. A series of 30 digits were then presented. For each the participant had to press the number 9 key for 'Yes' or the number 7 key for 'No', according to whether the digit was thought to be one of the five presented initially. Fifteen stimuli required a 'Yes' response and fifteen required a 'No' response. Reaction time and accuracy were recorded.
Word recognition. To test long-term memory, 15 words were presented for the word recall. They were presented again in random order interspersed with 15 new words. The subjects were again reminded that speed and accuracy were important. Pressing the number 9 key recorded a 'Yes' response or the number 7 key recorded a 'No' response, to signal whether or not the word was from the original list. Reaction time and accuracy were recorded.
Data analysis
Data from the cognitive and psychomotor tests were entered into Minitab® software. Blind analysis of the raw data, was undertaken by Clinphone Ltd, prior to the unlocking of the condition code. Drug induced performance changes, in all variables under test, were derived by subtracting the pre-dose (baseline) scores for each subject for the subsequent post-dose (test) scores. Differences between the flumazenil and placebo groups, at each time point, were then analysed using ANOVA.
Results
Eighteen subjects entered the study at the baseline time point (7 female, 11 male). All subjects completed two trial appointments at the 0–4 hour telephone tests. However, incomplete data was available from 3 subjects at the later time points (5 and 6 hours).
Test of attention
Simple Reaction Time (SRT)
The effect of the midazolam administration was to slow SRT (Fig. 1). The two groups began to speed up at the 2-hour time point but after this there was another slowing of reaction time. At no time point did the flumazenil group significantly react faster than the placebo group. The 6-hour time point results demonstrate that both the flumazenil and placebo groups have failed to reach or even approach the baseline reading.

Simple reaction time. Mean (± SE) changes from baseline
Choice Reaction Time (CRT)
CRT was significantly slower in both conditions to the 1-hour time point (Fig. 2). Both groups begin to recover at the 2-hour point. The flumazenil group was ahead of the placebo group from the 3 to 5-hour time points. At the 6-hour point the CRT of both groups were equal but still well below the baseline readings.

Choice reaction time. Mean (± SE) changes from baseline
Combined Numeric and Word Speed Scores
Combined speed scores represent the sum of numerical and word recognition speed (Fig. 3). The flumazenil group was always quicker than the placebo group although there is no statistically significant difference at any time points. Neither group attained the baseline speed scores.

Combined numeric and word speed scores. Mean (± SE) changes from baseline
Combined Numeric and Word Accuracy Scores
Combined accuracy scores again represent the sum of numerical and word recognition (Fig. 4). The flumazenil group was always more accurate than the placebo group although this proved not to be statistically significant.

Combined numeric and word accuracy scores. Mean (± SE) changes from baseline
Mood
Self rated alertness
Both groups became significantly less alert at the 1-hour time point (Fig. 5). Alertness gradually recovered throughout the period; the flumazenil scores were always above the placebo scores. The difference between the two treatments was manifest at the 2 and 6-hour time points (P < 0.05).

Self-rated alertness. Mean (± SE) changes from baseline. *pP < 0.05
Physiological measures
Analysis of heart rate, oxygen saturation and blood pressure failed to show any period effect or treatment period interaction. Statistical analysis also showed no significant difference between either treatment groups at 1 or 2 hours. Vital signs were not monitored after the patient was discharged home.
Discussion
This study demonstrates the severe impairment of cognitive and psychomotor function as a result of midazolam administration. This is evidenced by the increase in reaction times and the decrease in attention of patients when assessed using the measures of cognitive function – simple reaction time, choice reaction time, numeric and word recognition speeds and accuracy. In all of these measures the subjects display slower response times and increased cognitive decision times. In addition the self-reported measure of alertness clearly displays a decrease in alertness to baseline. This supports earlier work12,18 and confirms the evidence that midazolam impairs the patients' ability to recall information imparted during or immediately after the administration of the sedative.
Surprisingly, the administration of flumazenil does not appear to reverse the effects of midazolam sedation in terms of simple reaction time or in choice reaction time. Simple reaction time is the simplest test of cognitive function and is broadly related to power of concentration. Choice reaction time has components of attention and stimulus discrimination requiring the subject to make some level of assessment. Results suggest that flumazenil is not effective in reversing the cognitive impairment. It is also apparent that at no time point do the SRT and CRT reach baseline values. Indeed at the end of the test period, reaction times are no different from those seen when midazolam sedation is not reversed. The lack of effect could be because of artificially high baseline SRT and CRT speeds, possibly because of increased circulating catecholamine levels in the blood stream of the anxious patients prior to dental treatment. It may also be explained for the period 3 hours after reversal, by the fact that the reversal agent has worn off. However this would not explain the lack of effect immediately after reversal and 1- and 2- hour time points.
The effect of flumazenil reversal on numeric working and word recognition speed and accuracy appears to demonstrate an improvement in reaction times and accuracy when compared with the placebo. An interesting phenomenon of these tests is the apparent convergence of the flumazenil and placebo curves toward the 6-hour time point. This demonstrates the reduction in effect as the flumazenil is metabolized and becomes less active.
These results show that even after reversal with flumazenil, patients still have significant cognitive impairment in terms of speed of information processing. Patients discharged during this period may still have problems with cognitive tasks.
Other workers have demonstrated this variation in return of psychomotor function following flumazenil reversal. Several studies describe the rapid reversal of midazolam sedation with flumazenil in terms of CRT (at variance with this study) but to a lesser extent when the critical flicker fusion test was used.10,11 Claffey et al. recorded little difference in psychomotor scores between placebo and flumazenil groups.19
There is a decrease in alertness with the induction of sedation as would be expected. Interestingly, after receiving flumazenil, the self reported assessment of alertness implies that the patients themselves feel that they have regained their pre-sedation baseline scores, which is reflected in their clinical appearance. These findings seriously question the complete reliance on subjective assessment when assessing patients for discharge following sedation. Although they appear and feel alert, their underlying psychomotor function is still severely impaired.
The calmness and contentment increased gradually throughout the period of the study when measured against baseline. This is probably a reflection of the increase in 'well being' that the patients felt as their treatment came to a close. The effect of flumazenil on calmness and contentment was negligible.
Conclusion
Flumazenil does not appear to reverse the effects of midazolam sedation on psychomotor performance or attention. The attentional and stimulus discrimination handicaps of midazolam sedation are therefore still present. Flumazenil administration only partially reverses the effects of midazolam sedation on memory.
The suggestion based on the comparative pharmacology of midazolam and flumazenil, that re-sedation (ie sedation returns to a level that was present just prior to reversal) occurs with flumazenil is not supported by this study. Residual sedation (ie sedation returns to the level it would have been at if no reversal had been used) effects are present when flumazenil is used as a reversal agent. These results indicate that patients reversed with flumazenil should not be discharged early.
Although subjectively patients may appear clinically recovered after flumazenil reversal, their psychomotor ability and memory are in fact still severely impaired. Hence these patients and their escorts should receive the same postoperative instructions as if they had not been reversed.
References
Nadin G, Coulthard P Memory and midazolam conscious sedation. Br Dent J 1997; 183: 399–407.
Curran H V Tranquillising memories: a review of the effects of benzodiazepines on human memory. Biol Psychol 1986; 23: 179–213.
Thompson JM, Neave N, Moss MC, Scholey AB, Wesnes K, Girdler NM Cognitive properties of sedation agents: comparison of the effects of nitrous oxide and midazolam on memory and mood. Br Dent J 1999; 187: 557–562.
Neave N, Reid C, Scholey AB et al. Dose-dependent effects of flumazenil on cognition, mood, and cardio- respiratory physiology in healthy volunteers. Br Dent J 2000; 189: 668–674.
McCloy RF Reversal of conscious sedation by flumazenil: current status and future prospects. Acta Anaesthesiol Scand Suppl 1995; 108: 35–42.
Klotz U, Ziegler G, Ludwig L, Reimann IW Pharmacodynamic interaction between midazolam and a specific benzodiazepine antagonist in humans. J Clin Pharmacol 1985; 25: 400–406.
Klotz U, Kanto J Pharmacokinetics and clinical use of flumazenil (Ro 15-1788). Clin Pharmacokinet 1988; 14: 1–12.
Lauven PM, Schwilden H, Stoeckel H, Greenblatt DJ The effects of a benzodiazepine antagonist Ro 15-1788 in the presence of stable concentrations of midazolam. Anesthesiol 1985; 63: 61–64.
Whitwam JG Resedation. Acta Anaesthesiol Scand Suppl 1990; 92: 70–74.
Davies CA, Sealey CM, Lawson JI, Grant IS Reversal of midazolam sedation with flumazenil following conservative dentistry. J Dent 1990; 18: 113–118.
Hunter KM, Zacharias M, Parkinson R, Luyk NH Effect of flumazenil on the recovery from intravenous midazolam. N Z Dent J 1994; 90: 9–12.
Curran HV, Birch B Differentiating the sedative, psychomotor and amnesic effects of benzodiazepines: a study with midazolam and the benzodiazepine antagonist, flumazenil. Psychopharmacol 1991; 103: 519–523.
Wesnes KW, Ayre G, Pincock C Validity and utility of the Cognitive Drug Research (CDR) computerised assessment system: A review following fifteen years of usage. Eur Neuropschopharmacol 1999; 9: s3668.
Whitwam JG, Amrein R Pharmacology of flumazenil. Acta Anaesthesiol Scand Suppl 1995; 108: 3–14.
Rosenbaum NL, Hooper PA The effects of flumazenil, a new benzodiazepine antagonist, on the reversal of midazolam sedation and amnesia in dental patients. Br Dent J 1988; 165: 400–402.
Jensen S, Knudsen L, Kirkegaard L, Kruse A, Knudsen EB Flumazenil used for antagonizing the central effects of midazolam and diazepam in outpatients. Acta Anaesthesiol Scand 1989; 33: 26–28.
Bond AL, Lader MH The use of analogue scales in rating subjective feelings. Br J Med Psychol 1974; 47: 211–218.
Coulthard P, Sano K, Thomson PJ, Macfarlane TV The effects of midazolam and flumazenil on psychomotor function and alertness in human volunteers. Br Dent J 2000; 188: 325–328.
Claffey L, Plourde G, Morris J, Trahan M, Dean DM Sedation with midazolam during regional anaesthesia: is there a role for flumazenil? Can J Anaesth 1994; 41: 1084–1090.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Girdler, N., Fairbrother, K., Lyne, J. et al. A randomised crossover trial of post-operative cognitive and psychomotor recovery from benzodiazepine sedation: effects of reversal with flumazenil over a prolonged recovery period. Br Dent J 192, 335–339 (2002). https://doi.org/10.1038/sj.bdj.4801369
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4801369
This article is cited by
-
Significant and Safe Shortening of the Recovery Time After Flumazenil-Reversed Midazolam Sedation
Digestive Diseases and Sciences (2014)
-
A Quantitative System Pharmacology Computer Model for Cognitive Deficits in Schizophrenia
CPT: Pharmacometrics & Systems Pharmacology (2013)
-
The use of flumazenil after midazolam-induced conscious sedation
British Dental Journal (2010)
-
The effect of transmucosal 0.2 mg/kg midazolam premedication on dental anxiety, anaesthetic induction and psychological morbidity in children undergoing general anaesthesia for tooth extraction
British Dental Journal (2009)
-
Sedation reversal with flumazenil?
British Dental Journal (2002)
