
Key Points
-
This study shows that women taking oral contraceptives are at increased risk for dry socket and postoperative pain after extraction of a third molar.
-
The higher incidence of dry socket may be related to the fibrinolytic effect of oral contraceptives interfering with blood clotting.
-
As regards the higher incidence of pain, it is possible that oral contraceptives lower the pain threshold for reasons yet unknown.
Abstract
Objective This study investigated whether oral contraceptive use affects the incidence of complications (pain, trismus, dry socket) in women undergoing removal of impacted mandibular third molars.
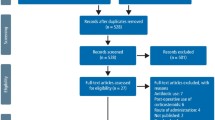
Patients and Method Two hundred and sixty seven women, aged 17 – 45 years, underwent removal of an impacted mandibular third molar. Eighty seven of the women were regular users of oral contraceptives. All patients were evaluated for postoperative pain, trismus and dry socket (localized alveolar osteitis).
Results Mean trismus values (measured as maximum interincisal distance) were similar in the two groups of patients. Postoperative pain was significantly more frequent among women taking contraceptives, both on day 1 (30% of women taking contraceptives used analgesics, versus 11% of women not taking contraceptives, p < 0.001) and on day 5 (14% versus 5%, p = 0.024). Similarly, dry socket occurred more frequently among women taking contraceptives than among women not taking contraceptives (11% versus 4%, p = 0.017).
Conclusions The results of this study support the view that oral contraceptive use favours the appearance of dry socket and postoperative pain after extraction, but has no effect on trismus.
Similar content being viewed by others

Main
The removal of a mandibular third molar typically provokes pain, inflammation and trismus, as well as other complications of varying frequency.1,2,3,4
Numerous studies have indicated that the incidence of complications after molar extraction is higher among women taking oral contraceptives,5,6,7,8,9,10,11,12 although some authors have not detected any association.13,14
The aim of the present study was to investigate the influence of oral contraceptive use on pain, trismus and dry socket (localized alveolar osteitis) after removal of a mandibular third molar.
Materials and Methods
A total of 267 women aged 17 to 45 years, all of whom underwent removal of a mandibular third molar at the University Hospital Complex of Santiago de Compostela (Spain), were included in the study. Patients aged more than 45 years were excluded from the study because of the much lower incidence of oral contraceptive use in this age group. Of the 267 patients, 87 were taking oral contraceptives, the mean age in this group was 25 years (SD 6 years). The remaining 180 patients were not taking contraceptives, the mean age in this group was 26 years (SD 7 years).
All extractions were performed by the same surgeon, under local anaesthesia (2% lidocaine with 1:80,000 epinephrine) and using the same surgical technique, with preliminary closure of the wound using absorbable suture.
After extraction, patients received prophylactic antibiotics (500 mg of amoxicillin every 8 h for 7 days) and anti-inflammatories (20 mg of piroxicam every 12 h for 3 days). Patients were told that in case of pain they could use analgesics, in accordance with its severity.
Maximum interincisal distance (MID) was determined before extraction, and 24 h and 5 days after extraction. At both follow-ups, we questioned the patient about analgesic use, and evaluated dry socket on the basis of clinical findings and reported symptoms (loss or necrosis of the wound clot, exposed alveolar bone, unpleasant odour, persistent severe postoperative pain). All follow-ups were performed by the same observer (PMG), who did not know whether the patient was taking contraceptives.
In the data analysis, a number of factors with potential effects on the risk of postoperative complications were considered, namely age, prior consumption of antibiotics, pre-operative state of the molar (asymptomatic, pain, pericoronitis), and difficulty of extraction (classified as I — extraction with forceps, II — ostectomy, III — ostectomy and coronal section, or IV — complex extraction).
Continuous variables are expressed in the text as means. Means were compared between groups by Student's t tests. For categorical variables, frequencies were compared by Fisher's exact tests. Statistical significance was taken to be indicated by p values of less than 0.05.
Results
Neither age nor any of the clinical factors considered differed significantly between the contraceptives and no-contraceptives groups (Table 1).
The incidence of postoperative trismus did not differ significantly between the two groups: on day 1, mean MID was 31 mm (SD 12 mm) in the contraceptives group and 33 mm (SD 13 mm) in the no-contraceptives group (p = 0.114).
Dry socket developed in 17 (6.4%) of the 267 patients: 10 patients (11.5%) in the contraceptives group and 7 patients (3.9%) in the no-contraceptives group. This difference is statistically significant (p = 0.017), and suggests that the risk of dry socket was three times higher in the contraceptives group. In all cases the dry socket was observed on day 5, as expected, given that processes of this type start 3 – 4 days after extraction. Complications were observed in only two cases, in which a lesion involving the dental nerve was detected.
Postoperative pain was significantly more frequent in the contraceptives group, both on day 1 (26 (29.9%) of patients in the contraceptives group reported use of analgesics, versus 19 (10.6%) in the no-contraceptives group; p < 0.001) and on day 5 (12 (13.8%) versus 9 (5.0%); p = 0.024).
Discussion
The most common postoperative complication of surgical removal of the impacted mandibular third molars is dry socket, due to fibrinolysis of the clot, typically as a result of invasion by oral-cavity bacteria.5
The incidence of post-extraction dry socket among women began to show a marked increase with respect to the incidence among men from the 1960s onwards, when oral contraceptives came into widespread use. In 1974, Schow9 observed post-extraction dry socket in 45% of women taking oral contraceptives, versus 17% of women not taking contraceptives, leading him to suggest that the incidence of dry socket is increased by oral contraceptive use. Similarly, in 1977, Sweet15 observed post-extraction dry socket in 19% of women taking oral contraceptives, versus 17% of women not taking contraceptives.
The higher incidence of dry socket among women taking oral contraceptives has been attributed to the pharmacological activity of the drug, since oral contraceptives induce increased fibrinolysis,16 and since dry socket has been attributed to increased fibrinolytic activity.17,18 Birn19 has suggested that trauma of the alveolar bone may induce transformation of plasminogen into plasmin, favouring fibrinolysis of the clot. Muhonen11 observed that fibrinolytic activity is increased during menstruation, favouring dry socket during this period.
The great majority of more recent studies have supported these hypotheses,3,4,5,6,7,8,9,10,11,12 and have considered oral contraceptive use to be a risk factor for dry socket after third molar removal. Some authors, including Larsen,13 have not detected any association between contraceptive use and dry socket, though it should be noted that this study was based on a relatively small sample.
The results of the present study support the view that oral contraceptive use increases the risk of dry socket: specifically, the incidence of dry socket was about 2 – 3 times higher in the women taking oral contraceptives than in the women not taking oral contraceptives. Our values for the incidence of dry socket (in both the contraceptives group and the no-contraceptives group) are similar to those reported in previous studies that have evaluated the incidence of complications after removal of mandibular third molars.1,2,3,4 By contrast, the studies of Hermesch,5 Catellani8 and Larsen13 obtained much higher control-group values (ranging from 17% – 30%), possibly reflecting methodological problems.
There have been no previous studies of the effects of oral contraceptive use on trismus after removal of mandibular third molars. In the present study, we did not detect any significant between-group difference in mean trismus (as revealed by maximum interincisal distance).
A previous study did not detect any significant effect of oral contraceptive use on the incidence of pain after removal of mandibular third molars.5 However, we found that the incidence of postoperative analgesic use was significantly higher in the contraceptives group than in the no-contraceptives group, particularly on day 1, raising the possibility that oral contraceptive use may affect the pain threshold, for physiological reasons as yet unknown.
References
Chiapasco M, De Cicco L, Marrone G . Side effects and complications associated with third molar surgery. Oral surg Oral Med Oral Pathol 1993; 76: 412– 420.
Goldberg MH, Nemarich AN, Marco WP . Complications after mandibular third molar surgery: a statistical analysis of 500 consecutive procedures in private practice. J Am Dent Assoc 1985; 111: 277– 279.
Osbom TP, Frederickson G, Small IA, Torgerson TS . A prospective study of complications related to mandibular third molar surgery. J Oral Maxillofac Surg 1985; 43: 767– 769.
De Boer M, Raghoebar G, Stegenga B, Schoen PJ, Boering G . Complications after mandibular third molar extraction. Quintessence Int 1995; 26: 779– 784.
Hermesch CB, Hilton TJ, Biesbrock AR et al. Perioperative use of 0.12% chlorhexidine gluconate for the prevention of alveolar osteitis. Efficacy and risk factor analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 85: 381– 387.
Bonine FL, Brighton M . Effect of chlorhexidine rinse on the incidence of dry socket in impacted mandibular third molar extraction sites. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995; 79: 154– 157.
Capuzzi P, Montebugnoli L, Vaccaro MA . Extraction of impacted third molars. A longitudinal prospective study on factors that affect postoperative recovery. Oral Surg Oral Med Oral PathoI 1994; 77: 341– 343.
Catellani JE, Harvey S, Erickson SH, Cherkin D . Effect of oral contraceptive cycle and dry socket (Iocalized alveolar osteitis). J Am Dent Assoc 1980; 101: 777– 780.
Schow SR . Evaluation of postoperative localized osteitis in mandibular third molar surgery. Oral Surg 1974; 38: 352– 358.
Muhonen A, Venta I, Ylipaavalniemi P . Factors predisposing to postoperative complications related to wisdom tooth surgery among university students. J Am Coll Health 1997; 46: 39– 42.
Norderam A, Grave S . Alveolitis sicca dolorosa after removal of impacted mandibular third molars. Int J Oral Surg 1983; 12: 226– 231.
Chapnick P, Diamond LH . A review of dry socket: a double blind study on the effectiveness of clindamycin in reducing the incidence of dry socket. J Can Dent Assoc 1992; 58: 43– 52.
Larsen PE . Alveolar osteitis after surgical removal of impacted mandibular third molar. Identification of the patient at risk. Oral Surg Oral Med Oral Pathol 1992; 73: 393– 397.
Berge TI, Boe OE . Predictor evaluation of postoperative morbidity after surgical removal of mandibular third molars. Acta Odontol Scand 1994; 52: 162– 169.
Sweet JB, Butler DP . Increased incidence of postoperative localized osteitis in mandibular third molar surgery associated with patients using oral contraceptives. Am J Obstet GynecoI 1977; 127: 518– 519.
Norris LA, Bonnar J . Haemostatic changes and the oral contraceptive pill. Ballieres Clin Obstet Gynaecol 1997; 11: 545– 564.
Gersel-Pedersen N . Fibrinolytic activity of blood and saliva before and after oral surgery. Int J Oral Surg 1981; 10: 114– 121.
Masuck R, Klammt J . The role of fibrinolysis in the pathogenesis of alveolitis after tooth extraction. Preliminary report. Dtsch Stomatol 1991; 41: 295– 296.
Birn H . Etiology and pathogenesis of fibrinolytic alveolitis (dry socket). Int J Oral Surg 1973; 2: 211– 263.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Garcia, A., Grana, P., Sampedro, F. et al. Does oral contraceptive use affect the incidence of complications after extraction of a mandibular third molar?. Br Dent J 194, 453–455 (2003). https://doi.org/10.1038/sj.bdj.4810032
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4810032
This article is cited by
-
Radiological risk indicators for persistent postoperative morbidity after third molar removal
Clinical Oral Investigations (2021)
-
Interventions for the prevention of dry socket: an evidence-based update
British Dental Journal (2014)
-
Accidents and complications associated to third molar surgeries performed by dentistry students
Oral and Maxillofacial Surgery (2014)
-
The prevention of 'dry socket' with topical metronidazole in general dental practice
British Dental Journal (2006)
-
Oral contraceptive and complications in third molar surgery
British Dental Journal (2003)
