
Abstract
Interleukin-6 (IL-6) is known to promote tumour growth and survival. We evaluated IL-6 gene amplification in tumours from 53 glioma patients using fluorescence in situ hybridisation. Amplification events were detected only in glioblastomas (15 out of 36 cases), the most malignant tumours, and were significantly associated with decreased patient survival.
Similar content being viewed by others


Introduction
Interleukin-6 (IL-6) is a pleiotropic cytokine that regulates the immune response, but also plays a role in promoting tumour growth and survival (Trikha et al, 2003; Hodge et al, 2005). In gliomas, the level of IL-6 gene expression increases with the grade of malignancy (Rolhion et al, 2001). In glioblastoma multiforme (GBM), the most malignant glioma, amplification/overexpression of the IL-6 gene appears to be a common feature (Tchirkov et al, 2001). Recent genomic array studies have reported that the number of IL-6 gene copies was increased in 40–50% of GBM (Suzuki et al, 2004; Saigusa et al, 2005). It is however unknown whether this alteration could be found in gliomas of lower malignancy grades. The prognostic significance of IL-6 gene amplification in GBM has not yet been determined. To address these issues, we evaluated here IL-6 gene amplification using interphase fluorescence in situ hybridisation (FISH) in 53 gliomas representative of various histological types and malignancy grades. In GBM, the results were correlated with patient survival.
Materials and methods
Glioma samples were taken from the material of surgical resection during the course of standard diagnostic procedure. Histological diagnosis and grading of tumours was consistent with the World Health Organization (WHO) criteria (World Health Organization, 2000). Nine tumours were classified as low-grade gliomas (grade I–II), including one pilocytic astrocytoma, three astrocytomas, two oligodendrogliomas and three oligoastrocytomas. Eight tumours were anaplastic gliomas (grade III), including six anaplastic oligoastrocytomas and two anaplastic oligodendrogliomas. The remaining 36 tumours were classified as GBM (grade IV). Patients with malignant gliomas (grade III–IV) were treated by surgery followed by either high-dose carmustine followed by radiotherapy in cases with optimal tumour resection or radiotherapy and concomitant temozolomide followed by monthly cycles of adjuvant temozolomide in cases with partial tumour resection or biopsy alone.
An interphase FISH was performed on frozen sections of gliomas mounted on Fisher Superfrost slides. The IL-6 gene probe was designed from the bacterial artificial chromosome clone RP11-240H8 (GenBank Accession Number AC073072) kindly provided by Professor Mariano Rocchi (University of Bari, Italy). The IL-6 probe labelled with SpectrumGreen (Vysis/Abbott, Rungis, France) and chromosome 7 cetromeric probe labelled with SpectrumOrange (Vysis/Abbott) were co-hybridised to evaluate simultaneously the number of IL-6 gene and chromosome 7 copies. A median of 148 nuclei (116–245, interquartile range) was scored using a Metafer4-MetaCyte microscope scanning system (MetaSystems, Le Cannet, France).
The number of IL-6 mRNA transcripts was assessed using quantitative real-time reverse transcriptase-PCR (qRT–PCR) in the LightCycler system (Roche Diagnostics, Meylan, France) with IL-6 specific primers (Tchirkov et al, 2001) and normalised to the expression of a housekeeping gene, ABL (Tchirkov et al, 2003).
Analyses of statistical links between biological and clinical characteristics were performed using standard tests. Overall survival was calculated using the Kaplan–Meier method and survival curves were compared using the log-rank test. A multivariate analysis was performed using the Cox regression model.
Results
Using interphase FISH approach, no IL-6 gene amplification was detected in low-grade or anaplastic tumours (n=17), whereas high-level amplification was found in 15 out of 36 (41.7%) GBM (Figure 1A and B). The percentage of nuclei with amplification events varied between 21 and 77% (33%, median).

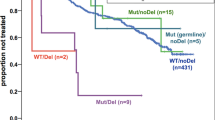
(A and B) Example of FISH analysis of chromosome 7 (red signals) and IL-6 gene (green signals) copy numbers in frozen sections of glioma tumours. A nucleus showing two copies of chromosome 7 and two copies of IL-6 gene (A); a nucleus with two copies of chromosome 7 and a high-level amplification of IL-6 gene (ratio of IL-6 to centromere 7 signals greater than 3) (B). (C) Overall survival as a function of IL-6 gene status in GBM patients. Patients with IL-6 gene amplification had significantly shorter survival than patients without amplification.
Quantification of IL-6 mRNA with qRT–PCR revealed a highly significant increase in the mean IL-6/ABL ratio in GBM (33.3%) as compared with non-GBM (1.5%; Kruskal–Wallis test, P=3.8 × 10−6). The mean IL-6/ABL ratio was >10-fold greater in GBM manifesting IL-6 gene amplification than in GBM without amplification (71.6 vs 6.1%; P=4.3 × 10−7).
GBM patients with amplified IL-6 gene had significantly shorter survival than patients without amplification (log-rank test, P=0.0000073; Figure 1C). Multivariate Cox analysis for overall survival, including IL-6 amplification, extent of tumour resection and age as variables, demonstrated that IL-6 amplification was an independent factor of poor prognosis (relative risk (RR) amplified vs non-amplified 8.07; P=0.000016). The complete tumour resection, equally distributed among patients with and without IL-6 gene amplification, was an independent factor of favourable prognosis (RR complete vs partial 0.31; P=0.013). Age did not influence survival of patients.
Discussion
Glioblastomas are the most devastating primary brain tumours. Despite modern treatments, about 40% of patients with GBM die within 6 months after diagnosis (Reardon et al, 2006). In the present study, we demonstrated that one of the molecular abnormalities associated with the aggressiveness of GBM is the amplification of the IL-6 gene, which was found in 41.7% of patients and significantly correlated with decreased survival.
Amplifications on chromosome 7p in GBM are believed to be driven by the amplification of the epidermal growth factor receptor (EGFR) gene locus (Rossi et al, 2005). This initial amplification event may induce instability along the length of this chromosomal arm, resulting in co-amplification of other genes. Of note, EGFR gene amplification has no clear prognostic value in GBM (Houillier et al, 2006). It may be possible that some of co-amplified (or independently amplified) genes are involved in glioma development and progression and are important for patient prognosis. Novel amplicons on chromosome 7p distinct from EGFR were recently identified using high-resolution genomic analyses and were reported to contain, among other genes, the IL-6 gene that was overexpressed (Rossi et al, 2005).
In gliomas, IL-6 plays a role in promoting tumour growth (Goswami et al, 1998) and angiogenesis (Loeffler et al, 2005). This cytokine also protects cancer cells from apoptotic depletion during chemotherapy and radiotherapy through activation of the Janus kinase/STAT and phosphatidylinositol 3-kinase/AKT pathways (Miyamoto et al, 2001; Trikha et al, 2003; Hodge et al, 2005). In this context, amplification of the IL-6 gene leading to its overexpression is likely one of the major factors contributing to the aggressiveness and poor response to therapies of GBM. It may therefore be suggested that targeting IL-6 and its signalling pathways in GBM would sensitise these otherwise resistant tumours to chemotherapeutic drugs and radiotherapy.
Accession codes
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Goswami S, Gupta A, Sharma SK (1998) Interleukin-6-mediated autocrine growth promotion in human glioblastoma multiforme cell line U87MG. J Neurochem 71: 1837–1845
Hodge DR, Hurt EM, Farrar WL (2005) The role of IL-6 and STAT3 in inflammation and cancer. Eur J Cancer 41: 2502–2512
Houillier C, Lejeune J, Benouaich-Amiel A, Laigle-Donadey F, Criniere E, Mokhtari K, Thillet J, Delattre JY, Hoang-Xuan K, Sanson M (2006) Prognostic impact of molecular markers in a series of 220 primary glioblastomas. Cancer 106: 2218–2223
Loeffler S, Fayard B, Weis J, Weissenberger J (2005) Interleukin-6 induces transcriptional activation of vascular endothelial growth factor (VEGF) in astrocytes in vivo and regulates VEGF promoter activity in glioblastoma cells via direct interaction between STAT3 and Sp1. Int J Cancer 115: 202–213
Miyamoto Y, Hosotani R, Doi R, Wada M, Ida J, Tsuji S, Kawaguchi M, Nakajima S, Kobayashi H, Masui T, Imamura M (2001) Interleukin-6 inhibits radiation induced apoptosis in pancreatic cancer cells. Anticancer Res 21: 2449–2456
Reardon DA, Rich JN, Friedman HS, Bigner DD (2006) Recent advances in the treatment of malignant astrocytoma. J Clin Oncol 24: 1253–1265
Rolhion C, Penault-Llorca F, Kemeny J-L, Lemaire J-J, Jullien C, Labit-Bouvier C, Finat-Duclos F, Verrelle P (2001) Interleukin-6 overexpression as a marker of malignancy in human glioma. J Neurosurg 94: 97–101
Rossi MR, La Duca J, Matsui S, Nowak NJ, Hawthorn L, Cowell JK. (2005) Novel amplicons on the short arm of chromosome 7 identified using high resolution array CGH contain over expressed genes in addition to EGFR in glioblastoma multiforme. Genes Chromosomes Cancer 44: 392–404
Saigusa K, Hashimoto N, Tsuda H, Yokoi S, Maruno M, Yoshimine T, Aoyagi M, Ohno K, Imoto I, Inazawa J (2005) Overexpressed Skp2 within 5p amplification detected by array-based comparative genomic hybridization is associated with poor prognosis of glioblastomas. Cancer Sci 96: 676–683
Suzuki T, Maruno M, Wada K, Kagawa N, Fujimoto Y, Hashimoto N, Izumoto S, Yoshimine T (2004) Genetic analysis of human glioblastomas using a genomic microarray system. Brain Tumor Pathol 21: 27–34
Tchirkov A, Rolhion C, Bertrand S, Doré JF, Dubost JJ, Verrelle P (2001) IL-6 gene amplification and expression in human glioblastoma. Br J Cancer 85: 518–522
Tchirkov A, Rolhion C, Kémény JL, Irthum B, Puget S, Khalil T, Chinot O, Kwiatkowski F, Périssel B, Vago P, Verrelle P (2003) Clinical implications of quantitative real-time RT–PCRanalysis of hTERT gene expression in human gliomas. Br J Cancer 88: 516–520
Trikha M, Corringham R, Klein B, Rossi JF (2003) Targeted anti-interleukin-6 monoclonal antibody therapy for cancer: a review of the rationale and clinical evidence. Clin Cancer Res 9: 4653–4665
World Health Organization (2000) Astrocytic tumors. Oligodendroglial tumours and mixed gliomas. In: Pathology and Genetics of Tumours of the Nervous System Kleihues P, Cavenee WK (eds) pp 6–70. Lyon: IARCPress
Acknowledgements
This work was supported by the Ligue Nationale Contre le Cancer (Comité du Puy de Dôme). We are grateful to Georges Briançon and Farida Godeau for expert technical assistance and Fabrice Kwiatkowski for statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Tchirkov, A., Khalil, T., Chautard, E. et al. Interleukin-6 gene amplification and shortened survival in glioblastoma patients. Br J Cancer 96, 474–476 (2007). https://doi.org/10.1038/sj.bjc.6603586
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6603586
Keywords
This article is cited by
-
Regulatory T cells promote glioma cell stemness through TGF-β–NF-κB–IL6–STAT3 signaling
Cancer Immunology, Immunotherapy (2021)
-
Prognostic role of high sensitivity C-reactive protein and interleukin-6 in glioma and meningioma patients
Journal of Neuro-Oncology (2018)
-
ATM inhibition prevents interleukin-6 from contributing to the proliferation of glioblastoma cells after ionizing radiation
Journal of Neuro-Oncology (2018)
-
NFAT1-regulated IL6 signalling contributes to aggressive phenotypes of glioma
Cell Communication and Signaling (2017)
-
Radiotherapy induces an immediate inflammatory reaction in malignant glioma: a clinical microdialysis study
Journal of Neuro-Oncology (2017)
