
Abstract
Background:
Sleep disturbances are frequent in patients with high spinal cord lesions, and are difficult to diagnose by means of polysomnography (PSG).
Design:
Retrospective cohort study.
Objective:
Examine the feasibility of sleep assessment by actigraph in patients with tetraplegia.
Setting:
A rehabilitation center in Israel.
Subjects:
Twenty-one patients with tetraplegia and 20 healthy persons.
Interventions:
Sleep assessment by actigraphs attached to the head and the wrist.
Main outcome measures:
The actigraphic movement index (MI), total sleep time (TST), sleep efficiency (SE), wake after sleep onset (WASO), sleep latency (SL), and number of awakenings (NOA).
Results:
In the control group actigraphy showed that during sleep the hand moves more than the head but that the movements were highly correlated. In patients with tetraplegia below C5–C7 the hand also moved more than the head, but in patients with tetraplegia below C4, the head moved more (P<0.05). No significant differences were found between patients with C5–C7 tetraplegia and healthy controls in the sleep indices obtained by hand movements, or between patients with C4 tetraplegia and healthy controls in the indices obtained by head movements. Control subjects and patients showed similar subjective assessment of sleep quality.
Conclusions:
These preliminary findings support the validity of wrist actigraphy for sleep assessment in patients with C5–C7 tetraplegia, and suggest that head-mounted actigraphy is a feasible alternative for sleep assessment in patients with tetraplegia below C4. To establish these findings, further investigations are required, with a larger number of patients and comparison with PSG.
Similar content being viewed by others


Introduction
Sleep disturbances are more frequent in patients with spinal cord lesions (SCLs) than in healthy people. Many of these patients (77.3%) report difficulty in falling asleep, early awakenings, and non-satisfactory sleep. They take more sleeping pills, and their snores are prolonged and more frequent than those of healthy persons.1, 2 These sleep disturbances may be caused by spastic muscle contractions, pain, sensory disturbances, or incontinence. Impairment of the sleep–wake cycle, a possible consequence of a cervical SCL, may also contribute to these disturbances. This cycle is modulated in part by melatonin secretion from the pineal body, which is stimulated by neural fibers that pass through the cervical spinal cord. These fibers originate in the lateral hypothalamus and descend through the brainstem and the cervical cord to the intermediolateral cell column in the upper thoracic cord, then return as sympathetic nerves to the pineal body through the upper cervical ganglion and the diencephalon.3, 4 Damage to cervical tracts may decrease the normal nocturnal melatonin secretion and thereby cause sleep abnormalities.5, 6, 7
Other clinical phenomena may also be related to ‘biological clock’ disturbances following cervical SCL. For example, in patients with cervical SCL urinary output may be higher during the night than during the day, in contrast to the diurnal urine output pattern in healthy people.8, 9
To study the relationship of ‘biological clock’ disturbances and clinical aspects of spinal cord injury, sleep cycle and sleep quality need to be monitored. The gold standard of sleep cycle and quality monitoring is polysomnography (PSG), but PSG studies are difficult to be performed in these patients. Usually, patients must sleep in the laboratory, sometimes for more than one night to avoid the ‘first night phenomenon,’ including difficulties falling asleep or maintaining sleep continuity in a new place, which may compromise the reliability of the PSG investigation.10 Moreover, patients with a high SCL sleeping in a laboratory may require equipment or trained staff for transfers, repositionings, or another specific care. Because PSG studies are also expensive and technically complicated, the usefulness of PSG in patients with tetraplegia is limited.11, 12, 13
Actigraphy is a partial alternative to PSG, which sidesteps some of the PSG limitations. The actigraph is a small tool equipped with a highly sensitive accelerometer that can continuously monitor and record movements of body parts. Data obtained from a wrist-mounted detector can distinguish sleep from wakefulness with high accuracy, comparable to that of PSG. This capability is based on the very high correlation between movement and wakefulnes and between lack of movement and sleep. Actigraphy can thus serve as a substitute for PSG under certain situations, and is widely used for sleep–wake cycle estimation in patients suffering from circadian rhythm disturbances, insomnia, or restless legs syndrome.14, 15, 16, 17, 18 The actigraph is usually attached to the non-dominant wrist for sleep–wakefulness investigation.19 Because the device monitors sleep–wakefulness by arm movements, it may not be effective if arm movement is impaired. In a healthy subject, actigraphy may miss wakefulness if the person lies calmly, without moving.14, 18
In patients with tetraplegia who cannot move their arm, a routine actigraphic study, with the actigraph attached to the wrist, may be useless. To overcome this problem, we considered attaching an actigraph to the head of patients with tetraplegia because the head is the only organ that moves normally in these patients. Previous studies showed that in healthy persons the head moves less than the wrists and more than the ankles during sleep.20
The present study was performed to assess the usefulness of actigraphy for sleep investigation in patients with cervical SCL, with the actigraph attached to the head or to the wrist. This preliminary study did not compare actigraphic and PSG findings directly because of the technical difficulty in performing PSG in patients with tetraplegia. Instead, it examined the feasibility of actigraphy in tetraplegia by testing the ability of a head-mounted actigraph to assess sleep in healthy subjects and comparing the actigraphic findings of patients with tetraplegia with those of healthy subjects.
Patients and methods
Forty-one persons participated in this study: 21 with tetraplegia and 20 healthy control subjects. The control group included eight men and 12 women with no sleep disturbances. Their average age was 42.1 years (SD=12.7). The SCL patients (16 traumatic, five non-traumatic) included 19 men and two women, all without previous sleep disturbances. The average age was 47.9 years (SD=13.5). The age difference between the two groups was not significant. In nine patients the level of the spinal cord injury was C4, in 10 patients it was C5. Among the C4 patients the severity grade of 5 was ASIA A,21 of 1 ASIA B, and of 3 ASIA C. Among the C5 patients the severity grade of 3 was ASIA A, of 5 ASIA B, and of 2 ASIA C. One patient was injured below C6 (ASIA B) and one below C7 (ASIA B). Patients were examined, on average, 125.2 months after injury (range 2–417 months, SD=136 months).
All subjects were asked about subjective sleep disturbances using the Mini Sleep Questionnaire (MSQ).22 An MSQ score of 10–25 indicates good sleep quality, 25–27 indicates sleep disturbance, 28–30 moderate disturbance, and 30 or more severe disturbance. Patients were asked to assess retrospectively their subjective sleep quality before the spinal cord injury and to compare it with the period after the injury.
Participants slept in their usual home or hospital beds. All subjects were examined using two actigraphs simultaneously (Somnitor 32K, Neurim Pharmaceuticals, Tel-Aviv, Israel) during one night. One of the actigraphs was attached to the forehead, and other to the wrist of the non-dominant hand. The actigraphs were activated when the participant went to sleep and shut down upon waking in the morning. The zero-crossing method23 was used to determine activity in the actigraph. The actigraph recordings were processed using the algorithm of Cole et al.24
The following outcome measures were assessed based on the actigraph data: movement index (MI, number of limb motions divided by time in bed), total sleep time (TST), sleep efficiency (SE), wake after sleep onset (WASO), sleep latency (SL), and number of awakenings (NOA). A Pearson correlation test and the paired t-test were used to compare data obtained from the head and wrist actigraphs. Analysis of variance (ANOVA)25 was used to compare patients with tetraplegia and healthy persons. SPSS for Windows (version 11; SPSS Inc., Chicago, IL, USA) was used for statistical data processing.
Results
Actigraphic findings
Control group
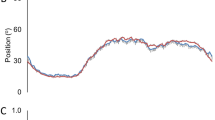
A significant high correlation was found between head-mounted and wrist actigraph measurements, including those of TST, SL, MI, WASO, and SE (Table 1). The correlation between head-mounted and wrist actigraph measurements of NOA was not high (Table 1). All the sleep measures indicated that the hand moves significantly more than the head during sleep (Table 2).
Tetraplegia group
The actigraphic findings were different for patients with injury below the C5–C7 level and those with injury below the C4 level.
Patients with injury below the C5–C7 level: In this subgroup, as in healthy subjects, the hand moved significantly more than the head during sleep. All sleep measures, except SL, showed significant differences between the wrist and the head-mounted actigraphic findings (Table 3).
Patients with injury below the C4 level: As opposed to healthy persons and patients with injury below the C5–C7 level, these patients demonstrated more head movements than hand movements during sleep. Significant differences were found in this group between head and wrist actigraphic findings in all the sleep measures except SL and NOA (Table 4).
Comparison between patients and healthy subjects
In all sleep measures except NOA hand actigraphy did not show a significant difference between the patients with injury below the C5–C7 level and the healthy subjects (Table 5). Head actigraphy did not show a significant difference between patients with injury below the C4 level and healthy subjects (Table 6). The power of similarity of these groups, however, was low (1−β=0.44–0.05).
Subjective sleep quality in SCL patients and healthy subjects
Assessment by MSQ did not show a significant difference in subjective sleep quality between healthy subjects and cervical SCL patients. The average MSQ score was 22.9 (SD=8.0) in patients with tetraplegia and 22.1 (SD=8.4) in healthy subjects. Nevertheless, all the patients claimed worsening of sleep quality after the spinal cord injury and recalled better sleep quality before the injury: average retrospectively estimated MSQ score of all patients was 14.25 (SD=5.4).
Discussion
Actigraphy is a common method for sleep assessment in healthy and sick persons. The agreement between actigraphic and polysomnographic (PSG) data is 82–90%.24 But sleep efficiency and latency may be overestimated by actigraphy as compared with PSG.14, 26, 27 The sensitivity of actigraphy, which is its ability to identify sleep when PSG does so, is 86.6–94%, but its specificity, the ability to identify wakefulness when PSG does so, is only 32–36%.26, 27
Actigraphy may overestimate sleep in patients with limb hypomobility because of various reasons, including Parkinson's disease, joint diseases, or involvement of the nervous system.14 Low specificity and exaggerated sensitivity of actigraphic data are expected in patients with plegia or paresis of the arms. Therefore, in the present study, we examined the feasibility of actigraphy in patients with tetraplegia and to overcome this problem by using a head-mounted actigraph.
Previous studies of healthy persons demonstrated higher mobility of the non-dominant arm than of the head during sleep.19, 20 The present study confirms the finding in healthy persons, and shows a similar finding in patients with SCL below the C5–C7 level and no movement or non-functional movements below the neurological level (ASIA grades A, B, or C). Moreover, most sleep measures obtained by wrist monitoring did not show a significant difference between these SCL patients and the healthy subjects. These findings indicate that an actigraph attached to the wrist may be used to assess sleep in patients with SCL below C5–C7, as it is done in healthy persons.
The similarity in actigraphic findings of hand movements between these SCL patients and healthy subjects is probably related to the preservation of normal activity of the proximal arm muscles in patients with SCL below C5–C7. Lesion severity, measured by ASIA grade, may have affected the actigraphic response in patients, but the effect was probably minimal because of normal arm movements down to the lesion level in this group. The significant difference in the number of awakenings between healthy persons and persons with SCL below C5–C7 may be related to the definition of ‘short awakening’ in the actigraphic analysis algorithm: patients with SCL below C5–C7 may not be able to reach the level of mobility required for identifying awakenings despite being able to move their arms, but this issue needs further investigation. Decreased afferent input from peripheral mechanoreceptor stimulation may also play a role in the decreased arousability in sleep of these patients.
In contrast to C5–C7 SCL patients, patients with complete motor SCL below the C4 level are not able to move their proximal arm muscles and their upper limbs in response to brain neural stimulation. Upper limb movements can be evoked by spinal cord neural activity below the lesion, but such movements are absent in many of these patients, or they are usually weak and irregular. It is not surprising, therefore, that these patients demonstrated more head movement than hand movement during sleep. Patients with ASIA C injuries below the C4 level may benefit more than those with ASIA A or B from wrist actigraphy, but our findings in three such patients are not sufficient to draw conclusions about it. As conventional actigraphy seems to be useless for the assessment of sleep in these patients, we used a head-mounted actigraph. To examine the usefulness of head-mounted actigraphy for these patients, we first tested the validity of head-mounted actigraphy in healthy subjects and compared the findings of C4 SCL patients and of healthy subjects.
The head-mounted actigraphy data reflected sleep and wakefulness adequately in healthy persons. Despite some significant differences between head and wrist actigraphic findings, we found significant high correlations between them in the majority of sleep measures (Table 1). The correlations enable prediction of hand actigraphy sleep measure values based on head actigraphy findings, using the regression equations of their relationships. This predictive ability supports the validity of head actigraphy in healthy people. Validity is better established for TST and SE, because the difference between head and wrist actigraphic findings is only 7% for these measures (Table 2). By contrast, NOA obtained from a head-mounted actigraph is not valid for sleep assessment (Table 1) because it may not reflect the NOA values obtained from the wrist of healthy subjects, owing to the definition of ‘short awakening’ in the actigraphic analysis algorithm.
The lack of significant differences between the sleep measures of healthy persons and C4 SCL patients indicates that in this patient group head movements may reflect sleep and wakefulness with a reasonable accuracy, as in the control group. This means that head actigraphy is a feasible method for assessing sleep in patients with SCL below C4. Head actigraphy could also be a valuable method for evaluating new treatments in C4 SCL patients suffering from insomnia or circadian rhythm disturbances.
The subjective report on sleep quality by MSQ supports the validity of the actigraphic findings. Consistent with wrist or head actigraphic findings, subjective reports by tetraplegic patients indicated a sleep quality similar to that of healthy subjects. If actigraphy missed some sleep disturbances because of sleep overestimation, as described in previous publications,1, 2 the missed sleep disturbances could have been reflected in the subjective report. But this did not happen, suggesting that it is unlikely that suitable actigraphy misses serious sleep disturbances in patients with tetraplegia. But the support lent by the subjective report to the actigraphic examination cannot be generalized to patients with severe disturbances of sleep quality, which were not examined in this study. Without data on objective sleep quality, including that obtained by electroencephalogram (EEG), oximetry, breathing effort, and leg electromyography (EMG) recordings, we cannot state that our patients were entirely free of sleep-related breathing abnormalities13 or periodic limb movement disorders.28
The lack of considerable sleep disturbances in the patients with tetraplegia is probably related to the duration of time from injury. Although newly injured patients, less than 1 year from injury, tended to complain about sleep quality disturbances, and although most SCL patients in this study complained about early awakenings, multiple awakenings during sleep, and difficulties in falling asleep, none of the SCL patients used sleeping pills or sedative drugs 5 years after injury, and all of them reported their sleep as satisfactory. These reports may indicate that spinal cord injured patients can adapt to the disturbances of night catheterizations, repositioning, muscle spasms and pain, and that after adaptation their sleep quality cannot be much different from that of healthy persons. These data may suggest that complaints of insomnia in SCL patients are time-related. But whereas subjective insomnia may decrease in tetraplegia with time after injury, the incidence of sleep disturbances such as sleep apnea syndrome13 may increase with time.
Further support for the use of head actigraphy for sleep/wake identification may be found in the recent suggestion that the ‘high-frequency EEG component’, which probably represents head/neck EMG activity, accurately represents waking.29 The use of neck EMG in patients with tetraplegia may also be useful for direct sleep assessment or for confirmation.
Despite the encouraging findings, and although actigraphy seems to be a good method for assessing sleep and measuring or controling some sleep disorders such as subjective insomnia and circadian rhythm disturbances, this method is not an alternative to PSG in the assessment of some major sleep disturbances.
Additional limitations of this study include the low-power value demonstrated in the statistical analysis for the similarity of actigraphic findings between patients with tetraplegia and healthy subjects, and the small subject sample. A larger sample may improve this power but it may also expose differences between subject groups that were not revealed in this study. Therefore, it is necessary to test additional patients and compare actigraphic data with PSG to validitate actigraphy for patients with tetraplegia.
Another potential study limitation is the use of the zero-crossing method to determine activity in the actigraph, as the available actigraph was not able to use the digital integration method, which allows quantifying the intensity or the amplitude of the movements and is considered to be the best.23 But this limitation is probably minor because all patients and subjects in the control group were evaluated using the same method.
In sum, these preliminary data suggest that wrist actigraphy appears to be as valuable for sleep–wakefulness assessment in C5–C7 SCL patients as in healthy subjects. For patients with SCL below C4, head actigraphy appears to be a feasible alternative for the evaluation of sleep and wakefulness. These findings should be elaborated in studies with a larger number of patients and validated by comparison with PSG.
References
Biering-Sorensen F, Biering Sorensen M . Sleep disturbances in the spinal cord injured: an epidemiological questionnaire investigation including normal population. Spinal Cord 2001; 39: 505–513.
Widerstrom-Noga EG, Felipe-Cuero E, Yeziersky RP . Chronic pain after spinal injury interference with sleep and daily activites. Arch Phys Med Rehabil 2001; 82: 1571–1577.
Hastings MH, Herbert J, Martenz ND, Roberts AS . Melatonin and the brain in photoperiodic mammals. Ciba Found Symp 1985; 117: 57–77.
Moore RY . Neural control of pineal function in mammals and birds. J Neural Transm Suppl 1978; 13: 47–58.
Zeitzer JM, Ayas NT, Shea SA, Brown R, Czeisler CA . Absent of detectable melatonin and preservation of cortisol and thyrotropin rhythms in tetraplegia. J Clin Endocrinol Metab 2000; 85: 2189–2196.
Kneisley LW, Moskowitz MA, Lynch HG . Cervical spinal cord lesions disrupt the rhythm in human melatonin excretion. J Neural Transm Suppl 1978; 13: 311–323.
Li Y, Jiang DH, Wang ML, Jiao DR, Pang SF . Rhythms of serum melatonin in patients with spinal lesions at the cervical, thoracic and lumbar region. Clin Endocrinol (Oxf) 1989; 30: 47–56.
Kooner JS, Frankel HL, Mirando N, Peart WS, Mathias CJ . Haemodynamic, hormonal and urinary responses to postural change in tetroplegic and paraplegic man. Paraplegia 1988; 26: 233–237.
Mathias CJ, Christensen NJ, Corbett JL, Frankel HL, Goodwin TJ, Peart WS . Plasma cathecholamines, plasma renin activity and plasma aldosterone in tetraplegic man, horizontal and tilted. Clin Sci Mol Med 1975; 49: 291–299.
Riedel BW, Winfield CF, Lichstein KL . First night effect and reverse first night effect in older adults with primary insomnia: does anxiety play a role? Sleep Med 2001; 2: 125–133.
Chokroverty S . Diagnosis and treatment of sleep disorders caused by co-morbid disease. Neurology 2000; 54: 8–15.
Bach JR, Wang TG . Pulmonary function and sleep disordered breathing in patients with traumatic teraplegia: a longitudinal study. Arch Phys Med Rehabil 1994; 75: 279–284.
Klefbeck B et al. Obstructive sleep apneas in relation to severity of cervical spine injury. Spinal Cord 1988; 36: 621–628.
Sadeh A et al. The role of actigraphy in the evaluation of sleep disorder. Sleep 1995; 18: 288–302.
Broughton R, Fleming J, Fleetman J . Home assessment of sleep disorders by portable monitoring. J Clin Neurophysiol 1996; 13: 272–284.
Brown AS, Smolensky MH, Dalonzo GE, Redman DP . Actigraphy: a means of assessing circadian pattern in human activity. Chronobiol Int 1990; 7: 125–133.
Jean LG et al. Determination of sleep and wakefulness with the actigraph data analysis software (ADAS). Sleep 1996; 19: 739–743.
Sadeh A, Sharkey KM, Carskadon M . An activity-based sleep- wake identification: an empirical test of methodological issues. Sleep 1994; 17: 201–207.
Van Hilten JJ, Middelkoop HA, Kuiper SL, Kramer CG, Roos RA . Where to record motor activity: an evaluation of commonly used sites of placement for activity monitors. Electroencephal Clin Neurophysiol 1993; 89: 359–362.
Webster JB, Messin S, Mullaney DJ, Kripke DF . Transducer design and placement for activity recording. Med Biol Eng Comput 1982; 20: 741–744.
International Standards for Neurological and Functional Classification of Spinal Cord Injury. American spinal injury association. Spinal Cord 1997; 35: 266–274.
Zomer J, Peled R, Rubin AH . Mini sleep questionnaire (MSQ) for screening population for EDS complains. In: Koella WP, Rudher E, Schulz H (eds). Sleep. Verlag: Stuttgart 1985, pp 470–487.
Spiro SW, Spiro JR . Comparing different methodologies used in wrist actigraphy. Sleep Review 2001; http://www.sleepreviewmag.com/article.php?s=SRM/2001/07&p=4.
Cole RJ, Kripke DF, Gruen W, Mullaney DJ, Gillin JC . Automatic sleep/wake identification from wrist actigraphy. Sleep 1992; 15: 461–469.
Dowson-Saunders B, Trapp RG . Basic and Clinical Biostatistics. Appleton and Lange: Norwalk, CT 1994, pp 162–180.
Blood ML, Sack RL, Percy DS, Pen JC . A comparasion of sleep detection by wrist actygraphy, behavioral response, and polysomnography. Sleep 1997; 20: 388–395.
Pollak CP, Tryon WW, Nagaraja H, Dzwonczyk R . How acurately does wrist actigraphy indefity the states of sleep and wakefulness? Sleep 2001; 24: 957–965.
Mello MT, Silva AC, Rueda AD, Poyares D, Tufik S . Correlation between K complex, periodic leg movements (PLM), and myoclonus during sleep in paraplegic adults before and after an acute physical activity. Spinal Cord 1997; 35: 248–252.
Sing HC et al. High-frequency EEG as measure of cognitive function capacity: a preliminary report. Aviat Space Environ Med 2005; 76 (Suppl 7): C114–135.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Spivak, E., Oksenberg, A. & Catz, A. The feasibility of sleep assessment by actigraph in patients with tetraplegia. Spinal Cord 45, 765–770 (2007). https://doi.org/10.1038/sj.sc.3102040
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3102040
Keywords
This article is cited by
-
Limb accelerations during sleep are related to measures of strength, sensation, and spasticity among individuals with spinal cord injury
Journal of NeuroEngineering and Rehabilitation (2022)
-
Actigraphy-based evaluation of sleep quality and physical activity in individuals with spinal cord injury
Spinal Cord Series and Cases (2019)
-
Actigraphy assessments of circadian sleep-wake cycles in the Vegetative and Minimally Conscious States
BMC Medicine (2013)
