
Abstract
Emergence of New Delhi metallo-β-lactamase-producing Enterobacteriaceae has become a challenging threat to public health. Two carbapenem-resistant Escherichia coli, strain QD28 and QD29, were recovered from the aspirating sputum of a neonate and the urine of an adult in a Chinese hospital in 2013. Molecular typing revealed that both isolates belonged to the sequence type 167, but they were clonally diverse. Both isolates exhibited resistance to carbapenems, cephalosporins, ciprofloxacin, gentamicin, piperacillin-tazobactam and trimethoprim-sulfamethoxazole. In addition, strain QD28 was also resistant to aztreonam and strain QD29 was resistant to amikacin, fosfomycin and minocycline. Antimicrobial resistance gene screening revealed that strain QD28 harbored aac(6′)-Ib, blaCTX-M-14, blaNDM-5, blaTEM-1 and sul1 genes and strain QD29 harbored aac(6′)-Ib, blaCTX-M-3, blaNDM-5, blaTEM-1, rmtB, sul1 and sul2 genes. The blaNDM-5 gene was found to be located on a 46-kb plasmid in two isolates and further sequence analysis showed that this plasmid was highly similar to the previously reported IncX3 plasmid pNDM-MGR194 in India. This is the first identification of blaNDM-5-carrying E. coli in the neonatal infection.
Similar content being viewed by others

Introduction
Carbapenems have been traditionally recognized as a last resort treatment for severe infected diseases caused by multidrug-resistant gram-negative bacilli1. However, due to their increasing usage, a variety of carbapenem-resistant bacteria have emerged and posed a serious public health threat. These bacteria can produce different carbapenemases to inactivate the drugs, of which New Delhi metallo-β-lactamase (NDM) is the recent emerging one of clinical significance. NDM-1 was first identified from a Klebsiella pneumoniae isolate in India in 20082 and has rapidly spread throughout the world. It can efficiently hydrolyze all β-lactams except monobactams. So far, 16 blaNDM gene variants have been discovered and assigned in the Lahey Clinic database and some variants are found to confer elevated carbapenem resistance3,4,5. The rapid evolution and dissemination of NDMs represent a crucial challenge for clinical infection treatments.
NDM-5 was discovered in a multidrug-resistant Escherichia coli isolate in the United Kingdom (UK) in 20113. It has two amino acid substitutions (Val88Leu and Met154Leu) in comparison with NDM-1 and seems to confer increased resistance to extended-spectrum cephalosporins and carbapenems. In the last five years, its encoding gene blaNDM-5 has been identified in clinical isolates in Algeria6, America7, Australia8, China9, Denmark10, India5,11, Japan12, Poland13, Singapore14, South Korea15, Spain16 and the Netherlands17. Different sequence types (STs) of E. coli and K. pneumoniae have been detected as NDM-5 producers. The diversity of these isolates indicates probable horizontal transfer of the blaNDM-5 gene either through plasmids or the transposon-related mobile elements. A number of plasmids belonging to the IncF, IncFII, IncN and IncX3 incompatibility groups are reported to carry blaNDM-5 (Table 1) and some plasmids have been completely sequenced. Unlike the prevalent blaNDM-1 gene, blaNDM-5 has been detected only in sporadic cases nowadays. However, considering its increased resistance phenotypes and global distribution, epidemiological survey of blaNDM-5 should arouse our attention.
In this study, we detected two NDM-5-producing E. coli isolates from the hospitalized patients in a Chinese hospital, of which one strain was isolated from a neonate and resistant to a range of antimicrobials.
Results
Strain features
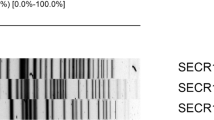
Two carbapenem-resistant E. coli isolates were collected from two hospitalized patients in different wards in a hospital in Shandong Province, China during September to October in 2013. Both patients had no history of foreign travel. Positive results were obtained in the modified Hodge test (MHT) and metallo-β-lactamase (MBL) antimicrobial gradient test, suggesting that they can produce MBLs. Further carbapenemase gene screening revealed that both isolates carried the blaNDM-5 gene. Because NDM-5 producers are infrequently detected worldwide, we performed multilocus sequence typing (MLST) and pulsed field gel electrophoresis (PFGE) experiments to analyze their clonal relatedness. Both isolates belonged to the ST167 epidemic clone, but PFGE revealed that they can be classified into different pulsotypes (Fig. 1), indicating that they were clonally diverse and excluding the possibility of nosocomial cross-transmission.

Dendrogram of patterns generated by pulsed-field gel electrophoresis (PFGE) of strain QD28 and QD29 using the BioNumerics software program
.
Antimicrobial susceptibility testing also showed different resistance profiles of these two E. coli isolates (Table 2). Strain QD28 displayed resistance to aztreonam, carbapenems (ertapenem, imipenem and meropenem), cephalosporins (cefotaxime, ceftazidime, cefepime and cefoxitin), ciprofloxacin, gentamicin, piperacillin-tazobactam and trimethoprim-sulfamethoxazole, intermediate resistance to minocycline and tobramycin and susceptibility to amikacin, fosfomycin, polymyxin B and tigecycline. However, strain QD29 was high level resistant to most tested antimicrobial compounds and only susceptible to aztreonam, polymyxin B and tigecycline.
Antimicrobial resistance gene screening
According to the multidrug resistance phenotypes of two isolates, a variety of antimicrobial resistance genes were screened by PCR in our study. In addition to blaNDM-5, strain QD28 was found to carry the aac(6′)-Ib, blaCTX-M-14, blaTEM-1 and sul1 genes and strain QD29 carried the aac(6′)-Ib, blaCTX-M-3, blaTEM-1, rmtB, sul1 and sul2 genes. The AmpC-type β-lactamase genes, plasmid-mediated fosfomycin resistance (PMFR) genes and plasmid-mediated quinolone resistance (PMQR) genes were not detected. Moreover, both isolates had amino acid substitutions in the quinolone resistance-determining regions (QRDRs), for strain QD28 in GyrA (Ser83Leu and Asp87Asn) and ParC (Ser80Ile) and for strain QD29 in GyrA (Ser83Leu and Asp87Asn), ParC (Ser80Ile) and ParE (Leu416Phe).
blaNDM-5-carrying plasmid analysis
In order to identify the blaNDM-5-carrying plasmids in two E. coli isolates, we carried out gene transfer experiments. The electroporation experiments were successful, but conjugation experiments failed. The E. coli TOP10 electroparants of strain QD28 and QD29 exhibited identical drug susceptibility phenotypes (Table 2). They were resistant to carbapenems, cephalosporins and piperacillin-tazobactam, but susceptible to the other non-β-lactam agents, in comparison with their E. coli donors. In addition, the E. coli electroparants of both isolates were found to contain a single plasmid of the same size. Only blaNDM-5 was identified in this plasmid and the other resistance genes present in strain QD28 and QD29 were not detected. Therefore, we presumed that the blaNDM-5-carrying plasmids in strain QD28 and QD29 might be very similar.
Subsequently, we attempted to obtain the whole plasmid sequences to better characterize these two blaNDM-5-carrying plasmids. The nucleotide sequences of pNDM-QD28 were obtained using Miseq techniques and the potential errors were corrected by PCR mapping. The pNDM-QD29 sequences were obtained by PCR mapping. Sequence analysis showed that these two plasmids with 46 kb in length were almost identical (Fig. 2) and had only four base substitutions. They belonged to the IncX3 group based on PlasmidFinder analysis on Center for Genomic Epidemiology. Further sequence alignments on BLAST revealed that the plasmid sequences showed more than 99% identities with those of the previously described plasmid pNDM-MGR194 of K. pneumoniae MGR-K194 in India11. The blaNDM-5 gene was preceded by ISSwi1, IS3000, ISAba125 and IS5 and followed by bleMBL (encoding resistance to bleomycin), trpF, dsbC and IS26. Other antimicrobial resistance genes were not detected in this plasmid.

Plasmid analysis of pNDM-QD28.
Schematic map of plasmid pNDM-QD28 (a), comparative analysis of four blaNDM-5-carrying IncX3 plasmids (b) and comparative analysis of the genetic contexts of blaNDM-5 in IncFII, IncX3 and IncN plasmids (c). The putative open reading frames are shown as arrowheads or rods (less than 130 amino acids). The gene name is shown near the corresponding arrowhead or rod. The depth of shading is indicative of the percentage BLASTN match, as indicated bottom.
Comparative analysis of the genetic contexts of blaNDM-5 in this IncX3 plasmid and the previously reported IncN12 and IncFII16 plasmids revealed some differences (Fig. 2c). In plasmid pNDM-QD28, the ISAba125 was interrupted by the insertion of IS5, so an ISAba125 remnant was present between IS5 and IS3000. However, this remnant was missing in plasmid pTK1044, suggesting that additional gene deletion and rearrangement may occur in this IncN plasmid. In plasmid pHC105-NDM, the blaNDM-5 module (blaNDM-5-bleMBL-trpF-tat) was surrounded by IS26 and ISCR1 that were associated with the ΔTn3 transposon and class I integron16, respectively, indicating that blaNDM-5 in this IncFII plasmid was mediated by a distinct mobilization mechanism.
Plasmid stability experiments showed that plasmids pNDM-QD28 and pNDM-QD29 were stable in isolate QD28 and QD29. After 10 rounds of subculture in MacConkey agar without antibiotic addition, the randomly selected strains all contained a plasmid identical to pNDM-QD28 and pNDM-QD29 in size and they all harbored the blaNDM-5 gene.
Discussion
Emergence of NDM-producing Enterobacteriaceae has become a crucial issue of global concern. The blaNDM gene not only confers resistance to most β-lactams, but also accompanies with multiple resistance gene determinants of different groups of antimicrobials in the same strain, which enables pathogens to become multidrug resistant. Therefore, NDM producers lead to limited clinical therapeutic options and represent a significant threat to public health. Epidemiological investigation and surveillance of NDMs are of importance to clinical infection control. Our study reported two NDM-5-producing E. coli isolates from Chinese hospitalized patients in 2013.
Strain QD28 was collected from a newborn admitted with neonatal pneumonia, which should be of significant note. NDM-producing Enterobacteriaceae are rarely identified in neonatal infections and only a few cases have been reported so far. In the last five years, some blaNDM-1-positive clinical isolates of Citrobacter sp., E. coli, Enterobacter cloacae and K. pneumoniae have been detected in neonates diagnosed with pneumonia, sepsis and septicaemia in India18,19,20,21 and NDM-1-producing K. pneumoniae isolates have been identified in neonatal units in Colombia22, Turkey23 and UK24. In addition, three NDM-1-producing Acinetobacter baumannii isolates were detected in association with neonatal infections in China25. To the best of our knowledge, our study is the first identification of NDM-5-producing E. coli in the neonatal infection. Other patients in the same ward were also screened for carbapenem-resistant isolates, but no NDM-5 producers were observed. The hospital environments were screened for multidrug resistant isolates each month and no NDM-5 producers were observed. Therefore, the origin of isolate QD28 was unclear.
Aminoglycosides and fluoroquinolones are rarely used for neonates and infants in China. However, strain QD28 displayed resistance to gentamicin and ciprofloxacin. Emergence of the resistance gene aac(6′)-Ib and mutations in QRDRs can be responsible for the resistance to the above two antimicrobial compounds.
The neonates are immunocompromised patients with a high risk of infection. Identification of multidrug-resistant NDM producers in neonatal infections is extremely worrisome, which will be very difficult to treat. Therefore, infection control measures should be reinforced to reduce the hospital-acquired multidrug resistance in the near future, such as implementing strict contact isolation precautions and performing supervised disinfection procedures.
Strain QD29 was recovered from a 47-year-old woman who contacted more complicated environments than neonates. Therefore, it displayed more diverse resistance profiles in comparison with strain QD28. Except aztreonam, polymyxin B and tigecycline, strain QD29 can be resistant to the rest antimicrobials tested in our study. In addition, strain QD29 exhibited higher level resistance to aminoglycosides, which may be explained by carrying the rmtB gene.
MLST analysis revealed that both NDM-5-producing E. coli isolates QD28 and QD29 in our study belonged to ST167, which is an internationally disseminated pathogen of human and animal and associated with numerous resistance mechanisms, especially blaNDM26,27. The blaNDM-1, blaNDM-5 and blaNDM-7 genes have been detected in E. coli ST167 as reported previously7,9,28,29. In particular, the NDM-5 producers hitherto identified in China are E. coli ST167 (8 isolates), ST2608 (1 isolate) and ST5131 (1 isolate)9,30,31, indicating that ST167 is an important reservoir of blaNDM-5 in China.
The blaNDM-5-carrying plasmids pNDM-QD28 and pNDM-QD29 were found to have almost identical nucleotide sequences with the previously reported IncX3 plasmid pNDM-MGR194 in K. pneumoniae in India11. In addition, the blaNDM-5-carrying plasmids, such as pEc1929 and pNDM5_0215, which were detected previously in five isolates from distinct cities in China, also showed high identities with pNDM-MGR194, except some minor differences9,31. Therefore, we presumed that this pNDM-MGR194-like plasmid probably played a significant role in the emergence and dissemination of the blaNDM-5 gene in China.
Furthermore, the blaNDM-5 genes identified in Australia and Denmark were also found to be located in IncX3 plasmids highly similar to pNDM-MGR1948,10. Their E. coli carriers (ST648 and ST1284) were isolated from patients who travelled to India (Table 1), suggesting that these two cases were associated with Indian NDM-5 dissemination. This pNDM-MGR194-like plasmid is consequently an important vehicle for the international dissemination of blaNDM-5. Identification of pNDM-MGR194-like plasmids in K. pneumoniae and E. coli of different STs indicates that this plasmid is able to mediate inter- and intra-species transfer of blaNDM-5, which will facilitate the rapid distribution of blaNDM-5 among enterobacterial species.
Although international travel and multinational medical treatment are reported to contribute greatly to the global distribution of blaNDM genes, all patients carrying NDM-5 producers identified in China had no foreign travel9,30,31. Therefore, these NDM-5-producing isolates are presumed to be autochthonous clones that have acquired the blaNDM-5-positive plasmid. Recent surveys have identified the NDM-5-producing E. coli from mastitic milk samples in India and dog in Algeria32,33, which should be of note, because farm animals and pets are important sources of antimicrobial resistant bacteria34. Although no NDM-5 producers have been reported in the environmental samples or animals in China, some NDM-1-producing Acinetobacter spp. have been identified in Chinese hospital sewages and animal farms35,36. More epidemiological studies are necessary in the future to clarify the mechanisms of emergence, evolution and dissemination of NDM-5 in China.
Methods
Ethics statement
Informed consent was obtained from the patients involved in this study. For the neonatal patient, consent from his parent was obtained. This study methods were reviewed and approved by the Ethics Committee of the Affiliated Hospital of Qingdao University and were carried out in accordance with the approved guidelines.
Bacterial strains
Two carbapenem-resistant gram-negative bacteria were collected from a teaching hospital in Shandong Province, east of China during 2013. Strain QD28 was isolated from the aspirating sputum of a seven-day-old newborn on October 2, 2013. He was a preterm baby, 1.6 kg in weight. Apgar scores of the baby were 9 at 1 minute, 9 at 5 minutes and 10 at 10 minutes. This low birth weight newborn was born in this hospital, admitted for neonatal pneumonia infection and treated with meropenem. Strain QD29 was recovered from the urine sample of a 47-year-old female patient on September 15, 2013. She was diagnosed with urinary tract infection and received ciprofloxacin and piperacillin/tazobactam after hospital admission. Both isolates were considered to be infections. Bacterial identification by using Vitek-2 compact system (BioMérieux, France) revealed that they were both E. coli. The MHT and MBL antimicrobial gradient test were performed for phenotypic identification of these two isolates.
Molecular typing
PFGE was carried out to analyze the clonal relatedness between two E. coli isolates. The genomic DNA was prepared in agarose blocks and digested with XbaI according to the protocol described by the CDC PulseNet program37. The XbaI-digested genomic DNA was subjected to PFGE using a CHEF-Mapper XA PFGE System (Bio-Rad, USA).
MLST was also carried out for molecular typing. Bacterial genomic DNA was extracted from the E. coli isolate. Seven housekeeping genes (adk, fumC, gyrB, icd, mdh, purA and recA) were amplified by PCR38 and the amplicons were submitted for DNA sequencing to analyze the ST.
Antimicrobial susceptibility testing
Antimicrobial susceptibility testing was performed on Mueller-Hinton agar plates using Etest strips (AB-BioMérieux, Solna, Sweden). The antibiotics tested in the study were amikacin, aztreonam, cefepime, cefotaxime, cefoxitin, ceftazidime, ciprofloxacin, ertapenem, fosfomycin, gentamicin, imipenem, meropenem, minocycline, piperacillin-tazobactam, polymyxin B, tigecycline, tobramycin and trimethoprim-sulfamethoxazole. The results were interpreted according to the Clinical and Laboratory Standards Institute guidelines39, except tigecycline and polymyxin B, for which European Committee on Antimicrobial Susceptibility Testing breakpoints were used40. E. coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as the control strains.
Antimicrobial resistance gene screening
A variety of antimicrobial resistance genes were screened by PCR and the positive amplicons were determined by DNA sequencing. These resistance genes included the prevalent extended-spectrum β-lactamase genes (blaCTX-M, blaOXA, blaSHV and blaTEM)41,42, AmpC β-lactamase genes (blaACC, blaACT, blaBIL, blaCMY, blaDHA, blaFOX, blaLAT, blaMIR and blaMOX)43, carbapenemase genes (blaAIM, blaBIC, blaDIM, blaGIM, blaIMP, blaKPC, blaNDM, blaOXA-48, blaSIM, blaSPM and blaVIM)44, 16S rRNA methylase genes (armA, npmA, rmtA, rmtB, rmtC and rmtD)45, PMFR genes (fosA, fosA3 and fosC), PMQR genes [aac(6′)-Ib-cr, qepA, qnrA, qnrB, qnrC, qnrD and qnrS]46 and dihydrofolate reductase genes (sul1, sul2 and sul3)47.
Mutations in the QRDRs
The QRDRs of the gyrA, gyrB, parC and parE genes in the chromosome were amplified by PCR using the primers previously described48,49 and sequenced to analyze the potential mutations.
blaNDM-carrying plasmid analysis
Electroporation and conjugation experiments were carried out to identify the blaNDM-carrying plasmids present in the two E. coli isolates. Plasmids were individually extracted from the E. coli isolates using a Qiagen Plasmid Midi Kit (Qiagen, Germany) and then electroporated to the competent E. coli TOP10 recipient cells. The E. coli electroporants were selected on Luria-Bertani agar plates containing 6 mg L−1 ceftazidime. Conjugation experiments were conducted by liquid mating with E. coli J53AziR as the recipient cells and the transconjugants were selected on tryptic soy agar plates containing 8 mg L−1 ceftazidime and 100 mg L−1 sodium azide. The E. coli electroporants were confirmed as blaNDM-positive by PCR analysis. The blaNDM-carrying plasmid size was evaluated by the S1-PFGE method50.
Plasmid sequencing
The blaNDM-carrying plasmids pNDM-QD28 (present in strain QD28) and pNDM-QD29 (present in strain QD29) were individually extracted from the E. coli electroporants using a Qiagen Plasmid Midi Kit for further DNA sequencing. The whole plasmid sequences of pNDM-QD28 were determined using an Illumina Miseq platform. A DNA library was prepared and subjected to paired end (2 × 300 base run) sequencing at the Sangon Biotech (Shanghai) Co. Ltd in China. The raw sequencing data were pre-processed using Prinseq-lite and subsequently assembled de novo using Velvet. The Gapcloser and Gapfiller programs were used for closing gaps and PrinSeS-G was used for correcting sequence errors. Subsequently, we used the assembled plasmid sequences of pNDM-QD28 as reference, acquired the plasmid sequences of pNDM-QD29 and re-corrected the plasmid sequences of pNDM-QD28 by PCR mapping. The plasmid sequences were annotated by RAST51 and the predicted open reading frames were further compared against the non-redundant protein database using BLAST.
Plasmid stability
Strain QD28 and QD29 was individually streaked out in the MacConkey agar, incubated at 37 °C for 24 h and then transferred to a fresh MacConkey agar. After repeated streaking for 10 days, 10 individual colonies were randomly selected and used to extract their plasmids. Subsequently, PCR was carried out to screen the blaNDM-5 genes.
Nucleotide sequences
The complete nucleotide sequences of plasmid pNDM-QD28 and pNDM-QD29 were submitted to GenBank with the accession numbers KU167608 and KU167609.
Additional Information
Accession Code: The GenBank accession numbers of the reference sequences are as follows: the IncX3 plasmid pNDM-MGR194, KF220657; the IncX3 plasmid pEc1929, KT824791; the IncFII plasmid pHC105-NDM, KM598665; the IncN plasmid pTK1044, LC000627.
How to cite this article: Zhu, Y.-q. et al. Identification of an NDM-5-producing Escherichia coli Sequence Type 167 in a Neonatal Patient in China. Sci. Rep. 6, 29934; doi: 10.1038/srep29934 (2016).
References
Citorik, R. J., Mimee, M. & Lu, T. K. Sequence-specific antimicrobials using efficiently delivered RNA-guided nucleases. Nat Biotechnol. 32, 1141–1145 (2014).
Yong, D. et al. Characterization of a new metallo-β-lactamase gene, blaNDM-1 and a novel erythromycin esterase gene carried on a unique genetic structure in Klebsiella pneumoniae sequence type 14 from India. Antimicrob Agents Chemother. 53, 5046–5054 (2009).
Hornsey, M., Phee, L. & Wareham, D. W. A novel variant, NDM-5, of the New Delhi metallo-β-lactamase in a multidrug-resistant Escherichia coli ST648 isolate recovered from a patient in the United Kingdom. Antimicrob Agents Chemother. 55, 5952–5954 (2011).
Gottig, S., Hamprecht, A. G., Christ, S., Kempf, V. A. & Wichelhaus, T. A. Detection of NDM-7 in Germany, a new variant of the New Delhi metallo-β-lactamase with increased carbapenemase activity. J Antimicrob Chemother. 68, 1737–1740 (2013).
Rahman, M. et al. Prevalence and molecular characterisation of New Delhi metallo-β-lactamases NDM-1, NDM-5, NDM-6 and NDM-7 in multidrug-resistant Enterobacteriaceae from India. Int J Antimicrob Agents. 44, 30–37 (2014).
Sassi, A. et al. NDM-5 carbapenemase-encoding gene in multidrug-resistant clinical isolates of Escherichia coli from Algeria. Antimicrob Agents Chemother. 58, 5606–5608 (2014).
de Man, T. J. B., Perry, K. A., Avillan, J. J., Rasheed, J. K. & Limbago, B. M. Draft genome sequence of a New Delhi metallo-β-lactamase-5 (NDM-5)-producing multidrug-resistant Escherichia coli isolate. Genome Announc. 3, e00017–15 (2015).
Wailan, A. M., Paterson, D. L., Caffery, M., Sowden, D. & Sidjabat, H. E. Draft genome sequence of NDM-5-producing Escherichia coli sequence type 648 and genetic context of blaNDM-5 in Australia. Genome Announc. 3, e00194–15 (2015).
Yang, P., Xie, Y., Feng, P. & Zong, Z. blaNDM-5 carried by an IncX3 plasmid in Escherichia coli sequence type 167. Antimicrob Agents Chemother. 58, 7548–7552 (2014).
Hammerum, A. M., Littauer, P. & Hansen, F. Detection of Klebsiella pneumoniae co-producing NDM-7 and OXA-181, Escherichia coli producing NDM-5 and Acinetobacter baumannii producing OXA-23 in a single patient. Int J Antimicrob Agents. 46, 597–598 (2015).
Krishnaraju, M. et al. Complete sequencing of an IncX3 plasmid carrying blaNDM-5 allele reveals an early stage in the dissemination of the blaNDM gene. Indian J Med Microbiol. 33, 30–38 (2015).
Nakano, R. et al. First report of metallo-β-lactamase NDM-5-producing Escherichia coli in Japan. Antimicrob Agents Chemother. 58, 7611–7612 (2014).
Baraniak, A. et al. NDM-producing Enterobacteriaceae in Poland, 2012-14: inter-regional outbreak of Klebsiella pneumoniae ST11 and sporadic cases. J Antimicrob Chemother. 71, 85–91 (2016).
Balm, M. N. et al. Emergence of Klebsiella pneumoniae co-producing NDM-type and OXA-181 carbapenemases. Clin Microbiol Infect. 19, E421–423 (2013).
Cho, S. Y. et al. Klebsiella pneumoniae co-producing NDM-5 and OXA-181 carbapenemases, South Korea. Emerg Infect Dis. 21, 1088–1089 (2015).
Pitart, C. et al. Molecular characterization of blaNDM-5 carried on an IncFII plasmid in an Escherichia coli isolate from a nontraveler patient in Spain. Antimicrob Agents Chemother. 59, 659–662 (2015).
Bathoorn, E., Rossen, J. W., Lokate, M., Friedrich, A. W. & Hammerum, A. M. Isolation of an NDM-5-producing ST16 Klebsiella pneumoniae from a Dutch patient without travel history abroad, August. Euro Surveill. 20, doi: 10.2807/1560-7917.ES.2015.20.41.30040 (2015).
Datta, S., Mitra, S., Viswanathan, R., Saha, A. & Basu, S. Characterization of novel plasmid-mediated β-lactamases (SHV-167 and ACT-16) associated with New Delhi metallo-β-lactamase-1 harbouring isolates from neonates in India. J Med Microbiol. 63, 480–482 (2014).
Datta, S. et al. A five-year experience of carbapenem resistance in Enterobacteriaceae causing neonatal septicaemia: predominance of NDM-1. PLoS One. 9, e112101 (2014).
Seema, K., Sen, M. R., Upadhyay, S. & Bhattacharjee, A. Dissemination of the New Delhi metallo-β-lactamase-1 (NDM-1) among Enterobacteriaceae in a tertiary referral hospital in north India. J Antimicrob Chemother. 66, 1646–1647 (2011).
Roy, S., Singh, A. K., Viswanathan, R., Nandy, R. K. & Basu, S. Transmission of imipenem resistance determinants during the course of an outbreak of NDM-1 Escherichia coli in a sick newborn care unit. J Antimicrob Chemother. 66, 2773–2780 (2011).
Escobar Perez, J. A. et al. Outbreak of NDM-1-producing Klebsiella pneumoniae in a neonatal unit in Colombia. Antimicrob Agents Chemother. 57, 1957–1960 (2013).
Poirel, L. et al. Spread of NDM-1-producing Enterobacteriaceae in a neonatal intensive care unit in Istanbul, Turkey. Antimicrob Agents Chemother. 58, 2929–2933 (2014).
Drew, R. J. et al. Emergence of carbapenem-resistant Enterobacteriaceae in a UK paediatric hospital. J Hosp Infect. 84, 300–304 (2013).
Chen, Y., Zhou, Z., Jiang, Y. & Yu, Y. Emergence of NDM-1-producing Acinetobacter baumannii in China. J Antimicrob Chemother. 66, 1255–1259 (2011).
Oteo, J. et al. Extended-spectrum β-lactamase-producing Escherichia coli in Spain belong to a large variety of multilocus sequence typing types, including ST10 complex/A, ST23 complex/A and ST131/B2. Int J Antimicrob Agents. 34, 173–176 (2009).
Schink, A. K., Kadlec, K., Kaspar, H., Mankertz, J. & Schwarz, S. Analysis of extended-spectrum-β-lactamase-producing Escherichia coli isolates collected in the GERM-Vet monitoring programme. J Antimicrob Chemother. 68, 1741–1749 (2013).
Cuzon, G., Bonnin, R. A. & Nordmann, P. First identification of novel NDM carbapenemase, NDM-7, in Escherichia coli in France. PLoS One. 8, e61322 (2013).
Zhao, J. Y. et al. Coexistence of SFO-1 and NDM-1 β-lactamase genes and fosfomycin resistance gene fosA3 in an Escherichia coli clinical isolate. FEMS Microbiol Lett. 362, 1–7 (2015).
Zhang, L. P., Xue, W. C. & Meng, D. Y. First report of New Delhi metallo-β-lactamase 5 (NDM-5)-producing Escherichia coli from blood cultures of three leukemia patients. Int J Infect Dis. 42, 45–46 (2016).
Chen, D. et al. Infection by and dissemination of NDM-5-producing Escherichia coli in China. J Antimicrob Chemother. 71, 563–565 (2016).
Ghatak, S. et al. Detection of New Delhi metallo-beta-lactamase and extended-spectrum beta-lactamase genes in Escherichia coli isolated from mastitic milk samples. Transbound Emerg Dis. 60, 385–389 (2013).
Yousfi, M. et al. First report of NDM-5-producing Escherichia coli ST1284 isolated from dog in Bejaia, Algeria. New Microbes New Infect. 8, 17–18 (2015).
Guerra, B., Fischer, J. & Helmuth, R. An emerging public health problem: acquired carbapenemase-producing microorganisms are present in food-producing animals, their environment, companion animals and wild birds. Vet Microbiol. 171, 290–297 (2014).
Zhang, C. et al. Higher isolation of NDM-1 producing Acinetobacter baumannii from the sewage of the hospitals in Beijing. PLoS One. 8, e64857 (2013).
Wang, Y. et al. Identification of New Delhi metallo-β-lactamase 1 in Acinetobacter lwoffii of food animal origin. PLoS One. 7, e37152 (2012).
Centers for Disease Control and Prevention. Standard operating procedure for PulseNet PFGE of Escherichia coli O157:H7, Escherichia coli non-O157 (STEC), Salmonella serotypes, Shigella sonnei and Shigella flexneri. Available at: http://www.cdc.gov/pulsenet/PDF/ecoli-shigella-salmonella-pfge-protocol-508c.pdf (Accessed: 26th November 2015) (2013).
Wirth, T. et al. Sex and virulence in Escherichia coli: an evolutionary perspective. Mol Microbiol. 60, 1136–1151 (2006).
Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Fifth Informational Supplement. CLSI document M100-S25. (eds Patel, J. B. et al.) 44–50 (Wayne, 2015).
European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 5.0. Availabe at: http://www.eucast.org/clinical_breakpoints/ (Accessed: 26th November 2015) (2015).
Woodford, N., Fagan, E. J. & Ellington, M. J. Multiplex PCR for rapid detection of genes encoding CTX-M extended-spectrum β-lactamases. Journal of Antimicrobial Chemotherapy. 57, 154–155 (2006).
Colom, K. et al. Simple and reliable multiplex PCR assay for detection of blaTEM, blaSHV and blaOXA-1 genes in Enterobacteriaceae. FEMS Microbiol Lett. 223, 147–151 (2003).
Perez-Perez, F. J. & Hanson, N. D. Detection of plasmid-mediated AmpC β-lactamase genes in clinical isolates by using multiplex PCR. J Clin Microbiol. 40, 2153–2162 (2002).
Poirel, L., Walsh, T. R., Cuvillier, V. & Nordmann, P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn Microbiol Infect Dis. 70, 119–123 (2011).
Bercot, B., Poirel, L. & Nordmann, P. Updated multiplex polymerase chain reaction for detection of 16S rRNA methylases: high prevalence among NDM-1 producers. Diagn Microbiol Infect Dis. 71, 442–445 (2011).
Zhao, J. Y. & Dang, H. Coastal seawater bacteria harbor a large reservoir of plasmid-mediated quinolone resistance determinants in Jiaozhou Bay, China. Microb Ecol. 64, 187–199 (2012).
Bibbal, D., Dupouy, V., Prere, M. F., Toutain, P. L. & Bousquet-Melou, A. Relatedness of Escherichia coli strains with different susceptibility phenotypes isolated from swine feces during ampicillin treatment. Appl Environ Microbiol. 75, 2999–3006 (2009).
Weigel, L. M., Steward, C. D. & Tenover, F. C. gyrA mutations associated with fluoroquinolone resistance in eight species of Enterobacteriaceae. Antimicrob Agents Chemother. 42, 2661–2667 (1998).
Zurfluh, K., Abgottspon, H., Hächler, H., Nüesch-Inderbinen, M. & Stephan, R. Quinolone resistance mechanisms among extended-spectrum beta-lactamase (ESBL) producing Escherichia coli isolated from rivers and lakes in Switzerland. PLoS One 9, e95864 (2014).
Barton, B. M., Harding, G. P. & Zuccarelli, A. J. A general method for detecting and sizing large plasmids. Anal Biochem. 226, 235–240 (1995).
Overbeek, R. et al. The SEED and the Rapid Annotation of microbial genomes using Subsystems Technology (RAST). Nucleic Acids Res. 42, D206–214 (2014).
Acknowledgements
This work was financially supported by grant 31100059 from the National Natural Science Foundation of China, grant 16CX02043A from the Fundamental Research Funds for the Central Universities and grant 2013-1-82 from the Key Programs of the Development of Science and Technology Bureau of Qingdao Economic & Technological Development Area.
Author information
Authors and Affiliations
Contributions
All authors contributed to the manuscript. Y.-q.Z. carried out bacteria characterization and antimicrobial susceptibility testing. J.-y.Z. carried out plasmid sequencing, data analysis and figures drawing. C.X., H.Z. and N.J. carried out PCR, gene transfer and molecular typing. Y.-q.Z. and J.-y.Z. wrote the manuscript. Y.-n.L. supervised the project and revised the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Zhu, Yq., Zhao, Jy., Xu, C. et al. Identification of an NDM-5-producing Escherichia coli Sequence Type 167 in a Neonatal Patient in China. Sci Rep 6, 29934 (2016). https://doi.org/10.1038/srep29934
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep29934
This article is cited by
-
Characterization of an NDM-5 carbapenemase-producing Escherichia coli ST156 isolate from a poultry farm in Zhejiang, China
BMC Microbiology (2019)
-
Dissemination of blaNDM-5 gene via an IncX3-type plasmid among non-clonal Escherichia coli in China
Antimicrobial Resistance & Infection Control (2018)
-
Salmonella enterica serovar Typhimurium ST34 co-expressing bla NDM-5 and bla CTX-M-55 isolated in China
Emerging Microbes & Infections (2017)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
