Food incentives to improve completion of tuberculosis treatment: randomised controlled trial in Dili, Timor-Leste
BMJ 2009; 339 doi: https://doi.org/10.1136/bmj.b4248 (Published 26 October 2009) Cite this as: BMJ 2009;339:b4248
- Nelson Martins, honorable minister for health1234,
- Peter Morris, project leader, head, ear and respiratory program125,
- Paul M Kelly, director, master of applied epidemiology program16
- 1Menzies School of Health Research, Darwin, NT, Australia
- 2Institute of Advanced Studies, Charles Darwin University, Darwin
- 3Faculdade Saude Publica, Universidade Da Paz, Dili, Timor-Leste
- 4Ministry of Health, Dili, Timor-Leste
- 5Northern Territory Clinical School, Flinders University, Darwin
- 6National Centre for Epidemiology and Population Health, Australian National, University College of Medicine, Biology and Environment, Canberra, ACT, Australia
- Correspondence to: P M Kelly, National Centre for Epidemiology and Population Health, College of Medicine, Biology and Environment, Australian National University, Building 62, Corner Mills and Eggleston Rds, Acton, Canberra, ACT 0200, Australia paul.kelly{at}anu.edu.au
- Accepted 14 August 2009
Abstract
Objective To determine the effectiveness of the provision of whole food to enhance completion of treatment for tuberculosis.
Design Parallel group randomised controlled trial.
Setting Three primary care clinics in Dili, Timor-Leste.
Participants 270 adults aged ≥18 with previously untreated newly diagnosed pulmonary tuberculosis.
Main outcome measures Completion of treatment (including cure). Secondary outcomes included adherence to treatment, weight gain, and clearance of sputum smears. Outcomes were assessed remotely, blinded to allocation status.
Interventions Participants started standard tuberculosis treatment and were randomly assigned to intervention (nutritious, culturally appropriate daily meal (weeks 1-8) and food package (weeks 9-32) (n=137) or control (nutritional advice, n=133) groups. Randomisation sequence was computer generated with allocation concealment by sequentially numbered, opaque, sealed envelopes.
Results Most patients with tuberculosis were poor, malnourished men living close to the clinics; 265/270 (98%) contributed to the analysis. The intervention had no significant beneficial or harmful impact on the outcome of treatment (76% v 78% completion, P=0.7) or adherence (93% for both groups, P=0.7) but did lead to improved weight gain at the end of treatment (10.1% v 7.5% improvement, P=0.04). Itch was more common in the intervention group (21% v 9%, P<0.01). In a subgroup analysis of patients with positive results on sputum smears, there were clinically important improvements in one month sputum clearance (85% v 67%, P=0.13) and completion of treatment (78% v 68%, P=0.3).
Conclusion Provision of food did not improve outcomes with tuberculosis treatment in these patients in Timor-Leste. Further studies in different settings and measuring different outcomes are required.
Trial registration Clinical Trials NCT0019256.
Introduction
Tuberculosis remains a considerable global public health concern with over nine million cases and 1.7 million deaths notified to the World Health Organization in 2006.1 Considerable progress has been made towards achieving the millennium development goals for tuberculosis by 2015, with incidence rates declining in the past two years.1 Central to the recommended treatment strategy is the use of directly observed treatment to ensure adherence. Intermittent or incomplete treatment has been associated with adverse outcomes for patients (severe disease and long term disability, low cure rate, disease relapse, or even death) and for public health (prolonged infectiousness and transmissibility and the development of drug resistance).
A series of Cochrane reviews are examining various methods of enhancing adherence to tuberculosis treatment. One review concluded that randomised trials provide no evidence that directly observed treatment improves cure or rates of completion of treatment in low and middle income countries compared with self administered treatment.2 Reminder systems and late patient tracers are effective in various settings, although most trials have been conducted in high income countries.3 The provision of monetary and other incentives to improve treatment adherence, including the provision of cash payments and food vouchers, has been found to be effective in some settings.4
Food incentives are attractive because of the well described link between malnutrition and tuberculosis; malnourished adults are more likely to develop tuberculosis and tuberculosis causes weight loss.5 The extent of malnutrition at diagnosis is strongly associated with severity of lung disease, increased relapse rates, and mortality in adults with pulmonary tuberculosis.6 7 8 Specifically, Khan and colleagues have shown that patients with tuberculosis who are underweight at diagnosis and achieve a weight gain of less than 5% during the intensive phase of treatment are at higher risk of disease relapse during the following two years.8
Various nutritional supplements are being used in tuberculosis programmes in many settings and have been advocated by the World Food Program.9 Nutritional supplements are popular with patients,10 but a recent Cochrane review showed unconvincing evidence of a direct benefit of food supplements on a range of clinical outcomes.11
We investigated whether nutritional supplementation with culturally appropriate food is an effective adjunctive therapy to enhance completion of tuberculosis treatment in Timor-Leste.
Methods
Setting
Timor-Leste is a small, newly independent Asian country with a population of around a million and a gross domestic product of $364 (£229, €244) per person per annum.12 It has a high incidence of tuberculosis but low rates of HIV and drug resistance.13 There is a well functioning National TB Control Program (NTP), which uses the WHO strategy known as DOTS (directly observed treatment).14 The study was conducted in three community clinics in the capital city, Dili. The clinics were government, private, and church operated (one of each) and covered geographically distinct zones within the city. Enrolment started on 16 March and was completed on 9 November 2005, with follow-up of all patients completed by July 2006. A political crisis starting on 28 April 2006 led to civil conflict in Dili for several months, including disruption to delivery of health services and the displacement of an estimated 70% of Dili’s population to camps within the city or to the rural districts.15
Participants and procedures
The study sample consisted of patients with newly diagnosed pulmonary tuberculosis (positive and negative results on sputum smear tests). A nurse or physician examined all outpatients and referred those with possible tuberculosis to the tuberculosis nurse for further examination, including sputum collection (spot/morning/spot). Trained laboratory technicians examined sputum by using the standard Ziehl-Neelsen method on direct smears. The diagnosis of tuberculosis in patients with negative smear results conformed to the NTP guidelines (no clinical response to 14 days’ treatment with broad spectrum antibiotics and chest x ray picture suggestive of active tuberculosis). The WHO reference laboratory in Adelaide, Australia, provided quality control of the tuberculosis laboratories. All participants received routine care, including drugs, default tracing, and clinical monitoring according to the NTP guidelines. Patients with tuberculosis were eligible for inclusion if they were aged ≥18 and agreed to receive tuberculosis treatment at the diagnosing clinic for eight months. Exclusion criteria were pregnancy and previous treatment for tuberculosis for more than one month.
Patients were asked to attend the clinic according to routine practice (five or six mornings a week) to receive directly observed treatment (intensive phase with daily rifampicin, isoniazid, pyrazinamide, and ethambutol daily for two months, followed by a continuation phase with isoniazid and ethambutol daily for six months) in appropriate doses (see table A on bmj.com). Treatment was administered fortnightly in the continuation phase.
Randomisation and blinding
At each study site a research assistant randomly allocated study participants to the intervention group (supplementary food) or control group (nutritional advice). An independent statistician computer generated a random allocation sequence with randomly varying block sizes in Stata (version 8). The sequence was concealed from all investigators with sequentially numbered opaque sealed envelopes prepared distant from the study site. Allocation was stratified by community health clinic and by diagnosis of tuberculosis (smear positive and smear negative). Both participants and treatment providers were aware of an individual’s allocation status after randomisation. An independent observer (PM, based in Darwin), who was blinded to the intervention received by the patients, however, determined the primary outcome (treatment completion).
Study intervention
At enrolment, the research assistant gave patients randomised to nutritional advice (control group) verbal and written advice concerning the types of locally available food that would constitute a balanced diet likely to assist cure of tuberculosis. These patients received routine care and were asked to attend the clinic at the usual time (early morning).
Patients in the intervention group were asked to attend the clinic at mid-day. In addition to usual treatment for tuberculosis, they received food every time they attended the clinic. In the intensive phase, each day they were provided with one bowl of feijuada, a locally popular meat, red kidney beans, and vegetable stew with rice, at the clinic (table 1⇓ and table B on bmj.com). This meal was rich in energy, protein, and micronutrients.16 The ingredients were obtained from local suppliers with fresh produce bought on the day of consumption and other produce bought in bulk. In the intensive phase of treatment a research assistant directly observed food intake. During the continuation phase of treatment, patients were given a food parcel containing unprepared food to take home (red kidney beans, rice, and oil). The quantities were calculated to provide one meal a day for one adult. At random intervals during the study period two authors (NM and PMK) checked the quality and quantity of produce. An independent assessment was carried out to ensure the safe preparation and administration of the intensive phase intervention.
Estimated nutritional value of average serving size for daily meal consumed by patients in intervention group in intensive phase of treatment
Outcome measures
We used standard Timorese NTP definitions of treatment outcome (see table C on bmj.com). The primary outcome measure was completion of treatment (clearance of acid fast bacilli from the sputum after treatment or the completion of eight months of treatment, or both). Secondary outcome measures were adherence to treatment, clinical improvement, and adverse events. Adherence was measured by recording clinic attendance and directly observed treatment (daily in the intensive phase and fortnightly in the continuation phase) and through interview and pill counts (in the continuation phase). All other measurements were performed weekly during the intensive phase and fortnightly during the continuation phase of treatment. Clinical improvement was measured by recorded clinical symptoms and weight gain. Percentage of weight change was calculated as the difference in weight at two times (for example, diagnosis and eight weeks) divided by the weight at the earlier time, multiplied by 100. Adverse events were actively recorded with a standardised questionnaire.
Sample size
Based on existing default rates of 13%, we calculated that we needed to enrol 270 patients to detect a reduction in the primary outcome (default rate) to an acceptable 3%, with 80% power and an α of 0.05.
Statistical analysis
Analysis was by intention to treat. We used independent t tests and Kruskal-Wallis tests to compare the difference in continuous variables between groups and Pearson’s χ2 test to compare the association between treatment group and categorical variables. Relative risks with 95% confidence intervals were calculated with standard methods. Rates of completion of treatment and clinical outcomes were also analysed with logistic regression with adjustment for prespecified confounding factors. Kaplan-Meier survival estimates were used to examine the relation between the intervention and time to default. Significance was based on a two tailed P<0.05. Analysis of secondary outcomes was regarded as “hypothesis generating.” No adjustment was made for multiple comparisons. All statistical analyses were performed with Stata (version 9.1).
Results
During the study enrolment period tuberculosis was diagnosed in 833 patients at the three clinics in Dili. Of these, 270 patients were recruited into the study (fig 1⇓). All participants received the allocated intervention, and only five (1.9%) were transferred to other clinics and did not contribute a primary outcome.

Fig 1 Flow of participants through study. Original sample included all diagnoses of tuberculosis in three clinics during study period, March 2005 to July 2006. Ineligible patients included 62 (25%) previously treated for tuberculosis, 176 (72%) aged <18, and 7 (3%) pregnant women. Others excluded, according to selection criteria, included 211 (79%) transferred out before enrolment, 42 (16%) community directly observed treatment (clinician’s decision), 7 (3%) unable to agree to complete treatment, 5 (2%) default before enrolment, 1 (0.5%) died before enrolment. Refusals: 43 (83%) unwilling to attend for midday meal; 9 (17%) chose community DOT (unable to attend clinic, self assessed disease severity). Loss to follow-up means transferred out to another clinic during treatment
After randomisation, the two groups of patients had similar demographic characteristics (table 2⇓). Most enrolled patients were young (mean age 33.3), male (175/270, 65%), poor (209/261 (80%) had no formal income), and lived close to the clinic (mean distance 2.4 km). Enrolled patients had had symptoms of tuberculosis for a mean of eight weeks before their diagnosis. There were no significant differences in the nature, duration, or frequency of tuberculosis symptoms or healthcare seeking behaviour between the two groups. Most patients (213/268, 80%) were malnourished, with almost one in three in WHO’s severely malnourished range (body mass index (BMI) <16.0).17 A relatively small proportion (79/270, 29%) of patients had positive results on sputum smear tests; this was similar in both groups and consistent with previous studies in Timor-Leste.14
Baseline characteristics of study participants. Figures are numbers (percentages) unless stated otherwise*
For the primary outcome of completion of treatment, there was no significant difference between the intervention (100/129, 76%) and control (103/136, 78%) groups (relative risk 0.98, 95% confidence interval 0.86 to 1.11) (table 3⇓). This is equivalent to a risk difference of −2% (−11% to 9%). In patients with positive smear results, there was a non-significant difference in completion of treatment (31/40, 78% for the intervention group v 25/37, 68% for controls, 1.15, 0.87 to 1.52; see table 4⇓). The civil conflict dramatically increased the default rate of those patients (68, 25%) still receiving treatment after 28 April 2006 and led to a significant decrease in treatment completion (168/199 (84%) before conflict v 35/66 (53%) after conflict; 1.58, 1.26 to 2.01; P<0.001).
Primary and secondary outcomes and adverse events by intention to treat analysis in all patients*. Figures are numbers (percentages) unless stated otherwise
Primary and secondary outcomes and adverse events by intention to treat analysis in patients with positive sputum smear results*. Figures are numbers (percentages) unless stated otherwise
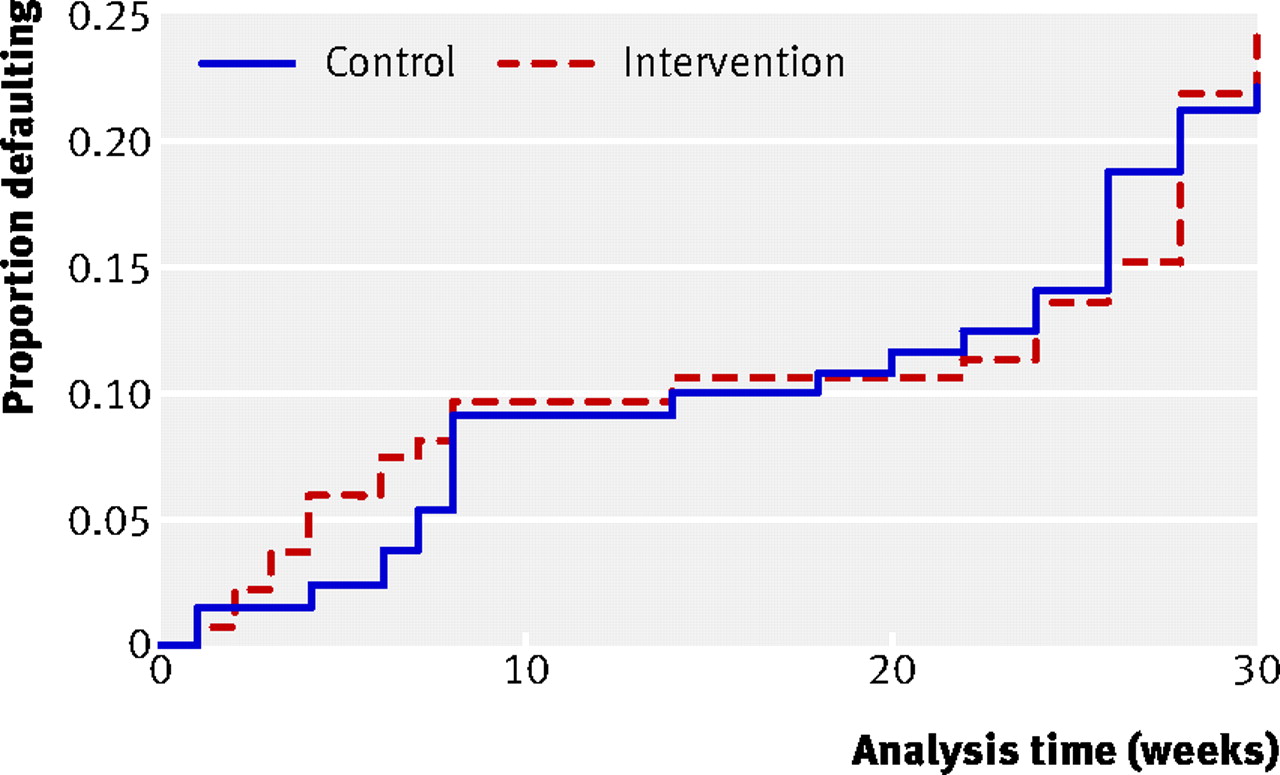
Secondary outcomes included adherence to treatment, weight gain, symptomatic improvement in all patients, and sputum smear clearance in the subgroup with positive smear test results. Almost all non-completion was because of default from treatment: there was only one death and one treatment failure during the study (see table C on bmj.com for definitions). While the default rate was higher than expected, most of this occurred in the final weeks of treatment. Early default was rare (fig 2⇓). Over half of the defaults were associated with the civil conflict (31/60). The intervention had no significant effect on default rates or time to default. While participants were receiving treatment, adherence was high, particularly in the continuation phase (98%). In the intensive phase, adherence was significantly lower in the intervention group (86.7%) than in the control groups (91.4%, P=0.02).

Fig 2 Kaplan-Meier plot showing time to default by group. Hazard ratio for time to default 1.10 (0.66 to 1.82), P=0.7. Not significantly influenced by age, sex, or result of smear test
The provision of tuberculosis treatment rapidly alleviated or considerably reduced most of the baseline symptoms. Haemoptysis and fever virtually disappeared during the first two months of treatment. Cough remained in most patients after four weeks and in a significant minority after eight weeks of treatment (table 3 and fig 3⇑ ⇓). The food intervention did not significantly hasten improvement in symptoms. Weight gain was significantly greater in the intervention group, both at the end of the intensive phase (5.2% increase for intervention v 3.5% for controls, P=0.04) and at the end of treatment (10.1% v 7.5%, P=0.04) (table 3⇑ and fig 4⇓). This relation was less strong in the subgroup with positive sputum smear results. In a post hoc analysis of those who were underweight at baseline (BMI <18.5, n=209 with 18 missing values), the food intervention led to a significant likelihood of adequate weight gain (that is, more than 5%) at two months compared with the control group (66/110 (60%) for the intervention group v 31/82 (38%) for controls; crude odds ratio 2.47, 1.37 to 4.44; P=0.003). After adjustment for age, sex, height, and smear result, the adjusted odds ratio was 2.69 (1.44 to 5.00; P=0.002). The result was even more striking in the subgroup who were severely underweight (BMI <16.0: 22/39 (56%) in intervention group v 10/38 (26%) controls), in whom the crude odds ratio was 3.62 (1.39 to 9.47; P=0.009) and the adjusted odds ratio was 3.37 (1.25 to 9.10; P=0.02).

Fig 3 Cough clearance in patients with tuberculosis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
In patients with positive sputum smear results, there was a non-significant improvement in sputum clearance at one month (18% absolute improvement, P=0.13). For this analysis, there was a substantial number of missing values because of default, refusal, inability to cough, or laboratory error. Patients with missing data, however, were similar at baseline when compared with those who were included in the analysis.
Over half the participants reported at least one adverse event potentially attributable to tuberculosis treatment. These were minor adverse events that occurred mostly during the first week of treatment and resolved with symptomatic treatment. None of the patients had to stop treatment. The main complaints were influenza syndrome, itch, and nausea. Itch with or without rash was more than twice as likely to occur in the intervention group (table 3).⇑ In patients with positive sputum smear results, the association was even more striking (relative risk 11.1, 1.51 to 81.5).
Multivariate analyses with adjustment for sputum smear result, clinic type, sex, education, occupation, income, and distance from the clinic did not change the results for outcome measures or adverse events.
Discussion
In this randomised controlled trial to examine the use of food as an incentive to improve outcome with tuberculosis treatment we found that food incentives led to modestly higher weight gain but did not result in a significant improvement in adherence to treatment or successful completion of treatment. Substantial improvement in completion of treatment (≥10%) is unlikely in this setting. Smaller beneficial (or harmful) effects cannot be excluded.
Our participants adhered well to treatment, and food, though expensive, was readily available at the urban study site during most of the study period. In other settings—for example, in sub-Saharan Africa where treatment completion rates are generally lower1 and food insecurity is widespread18—the result might be different.
Conflicting evidence of effectiveness in previous trials
The influence of macronutrient or micronutrient supplementation on outcomes of tuberculosis treatment has been inconclusive in the limited number of trials reported to date and has been summarised in a recent Cochrane review11 and in table 5⇓. Reported outcome measures have included sputum smear clearance, symptomatic improvement, weight gain during treatment, cure, recurrence of tuberculosis, and death. Our study provides the most comprehensive report on relevant outcomes to date and reports on adverse events. Given the potential for benefit of nutritional intervention, further studies on the role of whole food are warranted.
Summary of randomised controlled trials of nutritional interventions and tuberculosis (TB) by year of publication (adapted from Abba11) in community based adult patients unless stated otherwise
In this study, the only outcome significantly associated with the intervention was weight gain. Similar findings have been noted in studies in Singapore19 and in Tanzania20 but not in others21 22 23 24 25. Specifically, patients who were underweight at baseline were significantly more likely to gain more than 5% during the intensive phase of treatment, an important indicator of improved long term treatment outcome.8 This suggests that, although a food intervention seems to have little or no effect on treatment adherence and completion rates, this intervention might still be worth considering in patients with tuberculosis who are malnourished at diagnosis. This represents an important incremental step in knowledge and contributes to policy relevant evidence.
Symptoms improve with tuberculosis treatment, and all but one study24 have failed to show a significant additional improvement with adjunctive nutrition.21 26 Early sputum clearance contributes to a decreased period of infectiousness and can have a major influence on tuberculosis control. Our study showed encouraging trends in sputum smear clearance and cure rates in patients with positive sputum smears but was underpowered to examine these outcomes in the subgroup analysis. The findings from other studies are conflicting for this outcome, with one Mexican and two Indonesian studies showing more rapid22 or more complete27 28 sputum smear conversion in the intensive phase, a finding that has so far not been replicated elsewhere.20 25 29 30 Mortality during tuberculosis treatment is rare in Timor-Leste, and so it is unsurprising that we were unable to show any influence of the intervention on this outcome. Even in areas with high HIV prevalence, where death is more common, no effect has been found.25 26 29 31
Study limitations
For ethical reasons, we were required to differentiate between patients in the control and intervention groups by spacing their attendance at the clinic: control group in the morning and intervention group at lunchtime. Qualitative data derived from participants in the intervention group suggest that, despite the overwhelming acceptability of the meal, some people expressed shyness about eating at the clinic, while others complained about time inflexibility relating to clinic attendance. This might have been an unanticipated barrier to effective treatment, counteracting any positive effect of food provision and might explain the lower than expected adherence to treatment in the intensive phase. A cluster randomised trial, with a much larger sample size, might have been a more appropriate study design.
The conflict in Dili in the later part of the study clearly affected adherence to treatment in a substantial minority of patients. This led to a lower than expected overall rate of treatment completion. There was, however, no significant difference in the intervention or control groups during this period, so this is unlikely to have explained the negative result.
The randomised controlled trial design minimises confounding and maximises study validity. Our study shows that high quality intervention studies can be conducted successfully even in the most challenging setting. The strict selection of participants, however, might have excluded patients most likely to benefit. Our findings might have been different if we included, for example, those patients who were admitted to albuergues (hostels) for the intensive phase. In Dili, albuergues were designed to accommodate patients with certain characteristics, including high risk of non-adherence. It is also arguable that the true impact of food on treatment outcome and adherence should be measured differently. We lacked the necessary funding and equipment on site to measure potential immunological or biological parameters. Additionally, rather than concentrate on individual treatment outcome or adherence, the impact of a food incentive could be measured in the context of management of a tuberculosis programme. Perhaps the wider influence on the reputation of the clinics might lead to a greater willingness to come for both diagnosis and remain taking treatment.
An expensive intervention
Food provision is an expensive and logistically complex intervention. In this study, the introduction of food incentives involved building works, storage costs, purchase of equipment and consumables, transport, and salary costs, in addition to the actual food provided. When the true costs of these items are taken into account, we estimated the intensive phase costs at $2-3 (£1.2-1.8, €1.3-1.95) a meal, with a similar weekly cost for the food parcels in the continuation phase. This effectively doubles the cost per patient of tuberculosis treatment. There would need to be substantially stronger evidence of effectiveness of food to make this a cost effective intervention.
Conclusion
This randomised control trial of food incentive to improve treatment outcome was successfully conducted in Timor-Leste. In this setting food supplementation did not significantly improve treatment adherence or treatment outcome. Further studies with a larger sample size and a wider selection of patients in different settings will be required to confirm or refute this finding. Assessment of the impact of food supplementation as a strategy to improve management of tuberculosis programmes more widely and on the biological and immunological determinants of treatment response is also appropriate.
What is already known on this topic
Tuberculosis remains an important global public health concern
Adequate adherence to treatment is central to tuberculosis control; food incentives are attractive because of the well described link between malnutrition and tuberculosis
Nutritional supplements are being used in tuberculosis programmes in many settings and are popular with patients, though there is unconvincing evidence of direct benefit on a range of clinical outcomes
What this study adds
In Timor-Leste, food incentives led to modestly higher weight gain in patients with tuberculosis but did not result in a significant improvement in treatment adherence or successful completion of treatment.
Notes
Cite this as: BMJ 2009;339:b4248
Footnotes
We thank the Minister of Health of the Democratic Republic of Timor-Leste, the NTP Director and staff, and the management and staff of the three clinics in Dili where this study was performed. The research team in Dili (Saturnino Sarmento, Isabel Dos Santos Borromeu, Joana Melanya das Dores, Manuel Maria Martins, Agustinho da Silva, Casilda Viana) are acknowledged for their willingness to learn, their attention to detail and their care for the study participants under often difficult circumstances. We specifically acknowledge the invaluable assistance of Karen Walker (Baker International Diabetes Institute, Melbourne) for assistance with the constitution and analysis of the food supplementation and Mark Clements (ANU, Canberra) for statistical assistance.
Contributors: NM managed the field study while he was a doctoral student at the Charles Darwin University and wrote an earlier version of this report as part of his PhD thesis. PMK was NM’s principal supervisor, conceived the study protocol, and rewrote the report for publication. All authors participated in the study design, contributed to the data analysis, the interpretation of the results and revision of the report, and approved the final version. PMK is guarantor.
Funding: The study was funded by the Unicef/UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases, which also provided a PhD scholarship for NM. Australia’s National Health and Medical Research Council provides salary support for PMK. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests: None declared.
Ethical approval: This study was approved by human research ethics committees at the Charles Darwin University in Darwin, Northern Territory, Australia, and WHO, Geneva, Switzerland. In the absence of a functioning ethics committee, local permission to conduct this study was given by the Minister of Health, Timor-Leste. The funders had no role in the conduct of this study.
Data sharing: No additional data available.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.