Article Text

Abstract
Objective People who spend a longer time walking have lower demands for medical care. However, in view of their longer life expectancy, it is unclear whether their lifetime medical expenditure increases or decreases. The present study examined the association between time spent walking, life expectancy and lifetime medical expenditure.
Method The authors followed up 27 738 participants aged 40–79 years and prospectively collected data on their medical expenditure and survival covering a 13-year-period. Participants were classified into those walking <1 and ≥1 h per day. The authors constructed life tables and estimated the life expectancy and lifetime medical expenditure from 40 years of age using estimate of multiadjusted mortality and medical expenditure using a Poisson regression model and linear regression model, respectively.
Results Participants who walked ≥1 h per day have a longer life expectancy from 40 years of age than participants who walked <1 h per day. The multiadjusted life expectancy for those who walked ≥1 h per day was 44.81 years, significantly lower by 1.38 years in men (p=0.0073) in men and 57.78 years in women, non-significantly lower by 1.16 years in women (p=0.2351). In addition to their longer life expectancy, participants who walked ≥1 h per day required a lower lifetime medical expenditure from 40 years of age than participants who walked <1 h per day. The multiadjusted lifetime medical expenditure for those who walked ≥1 h per day was £99 423.6, significantly lower by 7.6% in men (p=0.0048) and £128 161.2, non-significantly lower by 2.7% in women (p=0.2559).
Discussion Increased longevity resulting from a healthier lifestyle does not necessarily translate into an increased amount of medical expenditure throughout life. Encouraging people to walk may extend life expectancy and decrease lifetime medical expenditure, especially for men.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
Medical expenditure per month was reduced when the amount of time spent walking was increased.
Walking is associated with a decreased risk of mortality.
In view of the increased life expectancy of those who walk longer, it is unclear whether lifetime medical expenditure increases or decreases as a result.
Key messages
Lifetime medical expenditure from the age of 40 years for men and women who walked ≥1 h per day was reduced by 7.6% and 2.7%, respectively, in comparison with those who walked <1 h per day.
Years of life added as a result of a healthy lifestyle did not necessarily translate into an increased amount of lifetime medical expenditure.
Strengths and limitations of this study
This is the first study to investigate the association between walking, life expectancy and lifetime medical expenditure.
We assessed walking using a simple questionnaire, in which we asked the participants to report only the time spent walking, and did not ask about walking pace, distance walked or any distinction between walking for exercise and other reasons.
Introduction
Previous studies have agreed that a higher level of physical activity extends life expectancy.1–4 Walking is part of a physically active lifestyle. Previous studies have indicated that a longer time spent walking,5–13 walking pace8 14–16 and a longer distance walked17 18 are significantly associated with a decreased risk of mortality.
We previously reported that medical expenditure per month was significantly reduced among those who spent a longer time walking, based on the same cohort dataset as that used here.19 Similar findings have been reported worldwide.20 21 However, in view of the increased life expectancy of those who walk for a longer time, it is unclear whether lifetime medical expenditure increases or decreases as a result. In other words, the question to be answered here is whether a lifelong healthy lifestyle eventually increases lifetime medical expenditure because of extended life expectancy.
So far, only one study has examined the association between physical activity and lifetime costs.4 This revealed that people with a high physical activity level tended to live longer than people with a lower physical activity level, and that the former had lower lifetime medical costs than the latter. However, that study was only a simulation analysis based on assumed variations in the health and economic effects of active and sedentary lifestyles.
The objective of the present study was to examine the association between walking, life expectancy and lifetime medical expenditure using actual individual data derived from a population-based 13-year prospective observation period. The population comprised 27 738 Japanese adults aged 40–79 years living in the community who were free of any functional limitations or chronic conditions interfering with physical activity, with an accrued total of 285 342 person-years. This cohort study has been monitoring survival and medical care utilisation, and its costs, for all participants.19 22 Using this dataset, we constructed a life table to estimate life expectancy and lifetime medical expenditure according to the time spent walking.24 25
Materials and methods
Study cohort
The present data were derived from the Ohsaki National Health Insurance (NHI) Cohort Study.19 22 25 We conducted a self-administered questionnaire survey of various lifestyle habits between October and December 1994 for all NHI beneficiaries aged 40–79 years who lived in the catchment area of Ohsaki Public Health Center, Miyagi Prefecture, northeastern Japan. Out of 54 996 eligible individuals, 52 029 (95%) responded.
We excluded 776 participants who had withdrawn from the NHI before 1 January 1995 because their cost data were not available. Thus, the remaining 51 253 participants formed the study cohort. The study protocol was approved by the Ethics Committee of Tohoku University School of Medicine. Participants who had returned the self-administered questionnaires and signed them were considered to have consented to participate.
For the present analysis, we excluded participants who had functional limitation or chronic conditions interfering with physical activity. Physical function status was assessed using the six-item measure of the Medical Outcomes Study Short-form General Health Survey.26 Participants were excluded if they stated on the Medical Outcomes Study questionnaire that they were unable to perform moderate or vigorous activities (n=15 916). We excluded participants who reported severe bodily pain (n=949), or any history of stroke (n=474), myocardial infarction (n=585) or arthritis (n=2176). We also excluded those who died within the first year (n=174) or did not provide complete responses in the walking status questionnaire (n=3241). Thus, a total of 27 738 participants (15 521 men and 12 217 women) remained. These participants were apparently healthy enough to walk for as long as they wished.
Time spent walking
The self-administered questionnaire included items on time spent walking. Time spent walking was assessed through the subject's response to the question, ‘About how much time do you walk per day on average?’ The participants were asked to choose one of three answers: ‘1 h or more,’ ‘30 min—1 h’ or ‘30 min or less.’ In Japan, the Ministry of Health, Labour and Welfare recommended to walk ≥1 h per day in Exercise and Physical Activity Reference for Health Promotion 2006. Then, we divided the participants into two groups according to the time spent walking daily: <1 h and ≥1 h. We had previously evaluated and reported the validity of self-reported time spent walking.5 19 27 This validation study had indicated that self-reported walking time was reasonably reproducible and sufficiently valid for studying the health effects of walking.
Health-insurance system in Japan
Details of the Japanese NHI system have been described previously.22 28 29 Briefly, everyone living in Japan is required to enrol in a health-insurance system. The NHI covers 35% of the Japanese population, mainly farmers, self employed or retired people. The NHI covers almost all medical treatment, including diagnostic tests, medication, surgery, supplies and materials, physicians and other personnel costs, inpatient care and most dental treatment. It covers treatment by physicians and nurses but not that by other professionals such as home health aides. Payment to medical providers is made on a fee-for-service basis, where the price of each service is determined by a uniform national fee schedule.
When a participant withdraws from the NHI system because of death, emigration or employment, the withdrawal date and its reason are coded in the NHI withdrawal history files. We recorded any mortality or migration by reviewing the NHI withdrawal history files and collected data on the death of participants by reviewing the death certificates filed at Ohsaki Public Health Center. We thus followed up the participants and prospectively collected data on medical care utilisation and its costs for all individuals in the cohort from 1 January 1995 to 31 December 2007. Study participants (16.3%) were lost to follow-up, so their vital status was unknown.
Statistical analysis
Using the Ohsaki NHI cohort database, we estimated mortality and medical expenditure for individual age groups, and for the categories of time spent walking, for both men and women. We divided age into the following groups: 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84 and ≥85 years. The multiadjusted mortalities for each age category were estimated from a Poisson regression model based on person-years and the number of deaths from 1996 until 2007. The dependent variable was mortality, and the independent variables were age groups, categories of time spent walking and the following covariates: smoking status (current and past smoker, or never smoker), alcohol consumption (current drinker consuming 1–499 g/week, current drinker consuming ≥450 g/week, or never and past drinker), body mass index (BMI: <21 kg/m2, 21–24.9 kg/m2 or ≥25 kg/m2), self-rated health (good or not good), sports and physical activity (≥3 h/week or <3 h/week), history of hypertension disease (presence or absence), history of diabetes mellitus (presence or absence), history of cancer (presence or absence), history of liver disease (presence or absence) and history of kidney disease (presence or absence).19 The data on all covariates were obtained from a self-administered questionnaire. We estimated the mortality of participants aged ≥85 years by multiplying the estimated mortality for the 85–89-year age group by the ratio of mortality for the same age group relative to the mortality for ≥85 years from complete life tables for the year 2000, as there were few person-years for participants aged over 90 years in our dataset.30
Because medical expenditure increases before death, we separately calculated medical expenditure for participants who survived through the index year and for those who died. The multiadjusted medical expenditure per year for survivors and decedents, respectively, was estimated for each of the age groups and the categories of time spent walking using a linear regression model adjusted for the above covariates.
The estimates of multiadjusted mortality and medical expenditure for each age group were used for estimating life expectancy and lifetime medical expenditure from 40 years of age. Life expectancy was calculated using Chiang's analytical method on the basis of the latest published complete life tables of Japan for the year 2000.23 30 Lifetime medical expenditure was estimated from the sum obtained by multiplying the static population in life table by the medical expenditure for survivors and the number of deaths in the life table by the increased medical expenditure owing to death, which was calculated by subtracting the medical expenditure in year of survivors from that in the period of 1 year before death. That is, the life expectancy (
∑ is the sum of y≥x
The 95% CIs were estimated using a Monte Carlo simulation with 100 000 replicates based on a Poisson regression model and linear regression model. All analyses were used the SAS V.9.1 statistical software package.
We used a purchasing-power parity rate (British pounds to Japanese yen) of £1.00=¥140.
Results
After 13 years of follow-up, we observed 2936 deaths (2193 men and 743 women) among the 27 738 participants (15 521 men and 12 217 women). The mean medical expenditure per year for survivors who walked ≥1 h per day was £1714.2 in men and £1621.4 in women, significantly lower than for those who walked <1 h per day (men: £2064.3, p<0.0001; women: £1878.6, p<0.0001). Also, the mean medical expenditure in the year of death for participants who walked ≥1 h per day was £16 878.6 in men and £17 464.3 in women, which was not significantly different from those who walked <1 h per day (men: £16 650.0, p=0.7315; women: £17 742.9, p=0.8330).
Baseline characteristics in terms of categories for time spent walking
Table 1 shows the baseline characteristics of the study participants according to the categories of time spent walking for men and women, respectively.
As compared with those who walked <1 h per day, participants who walked ≥1 h per day were less likely to be smokers and obese. Self-reported histories of hypertension, diabetes mellitus and liver disease were all significantly less prevalent in those who walked ≥1 h per day.
Baseline characteristics by time-spent-walking categories in 27 738 participants
Mortality in terms of categories for time spent walking
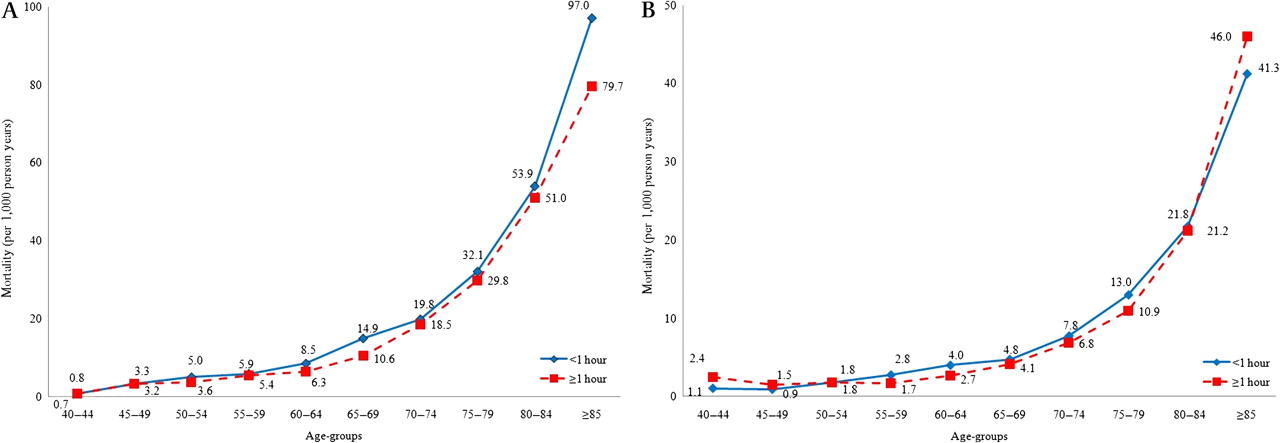
Figure 1A (for men) and Figure 1B (for women) show the multiadjusted mortality (per 1000) in each of the age groups according to the categories of time spent walking.

{kind=link}
Multiadjusted mortality by time-spent-walking categories in each age group in (A) men and (B) women.
In men in each age group, the multiadjusted mortality was lower in participants who walked ≥1 h per day than in those who walked <1 h per day. In women in all age groups except for the aged 40–44 and 45–49 year groups, the multiadjusted mortality was lower in participants who walked ≥1 h per day than in those who walked <1 h per day.
Table 2 shows the mortality ratio with 95% CIs according to the categories of time spent walking. In men, the multiadjusted mortality ratio for participants who walked ≥1 h per day was significantly lower than that for participants who walked <1 h per day (0.90, 95% CI 0.82 to 0.98, p=0.0153). In women, the multiadjusted mortality ratio for participants who walked ≥1 h per day was non-significantly lower than that for participants who walked <1 h per day (0.95, 95% CI 0.82 to 1.10, p=0.4693).
Mortality ratio for time-spent-walking categories in 27 738 participants
Life expectancy and lifetime medical expenditure in terms of time spent walking
Table 3 shows the life expectancy and lifetime medical expenditure from 40 years of age with 95% CIs according to the categories of time spent walking.
Life expectancy and lifetime medical expenditure at age 40 years for time-spent-walking categories in 27 738 participants
In men, the multiadjusted life expectancy of those who walked ≥1 h per day was 44.81 years (95% CI 43.66 to 45.94), which was significantly longer by 1.38 years (p=0.0073) than for those who walked <1 h per day (43.43 years; 95% CI 42.39 to 44.41). In women, the same results were observed, although the differences did not reach statistical significance.
In spite of their longer life expectancy, their lifetime medical expenditure from 40 years of age was significantly lower in men and non-significantly lower in women. The multiadjusted lifetime medical expenditure for participants who walked ≥1 h per day was £99 423.6 (95% CI 92 515.9 to 106 694.7), significantly lower by 7.6% (p=0.0048) than for those who walked <1 h per day (£107 544.2; 95% CI 101 234.0 to 114 044.6). In women, the multiadjusted lifetime medical expenditure for participants who walked ≥1 h per day was £128 161.2 (95% CI 111 335.0 to 148 494.7), non-significantly lower by 2.7% (p=0.2559) than for those who walked <1 h per day (£131 766.8; 95% CI 115 902.4 to 150 714.3).
Discussion
The present results indicate that the multiadjusted lifetime medical expenditure from the age of 40 years for those who walked ≥1 h per day was significantly lower by 7.6% in men and non-significantly lower by 2.7% in women than for those who walked <1 h per day. This decrease in lifetime medical expenditure was observed in spite of a longer life expectancy (1.38 years for men and 1.16 years for women) among those who walked ≥1 h per day. Thus, a healthy lifestyle not only extended longevity but also decreased the amount of lifetime medical expenditure, especially men.
We observed statistically significant differences for men but not for women. Although the differences did not reach statistical significance, the same results were observed for women. The reason why the impact of walking was smaller in women than in men was unknown. In women, other factors such as obesity and postmenopausal change might have a stronger impact on life expectancy and lifetime medical expenditure than walking.
Comparison with other studies
Four studies have addressed the association between physical activity level and life expectancy.1–4 Additionally, studies investigating associations between time spent walking,5–13 or distance walked17 18 and mortality have consistently shown that participants who have a higher physical activity have a longer life expectancy and lower mortality than participants who have a lower physical activity. Only one study has reported the association between physical activity and lifetime medical expenditure.4 In a simulation study, Keeler et al demonstrated that if participants with a sedentary lifestyle had exercised regularly, the additional exercise would have increased their life expectancy by 300 days and saved £1900 in lifetime costs. Even though there is a difference between physical activity and walking, this result is consistent with the present finding that participants who walked ≥1 h per day lived longer and had a lower lifetime medical expenditure.
We previously calculated life expectancy and lifetime medical expenditure in relation to smoking and BMI from age 40 years using the same dataset as that for the present study.24 The results indicated that lifetime medical expenditure was lower for smokers than for non-smokers, reflecting the 3.5-year shorter life expectancy of smokers.24 On the other hand, lifetime medical expenditure was higher for participants who were obese (BMI≥30.0) than for those who were of normal weight (18.5≤BMI<25.0), even though the former lived 2 years less than the latter (Nagai M, Kuriyama S, Kakizaki M, et al. Impact of obesity, overweight and underweight on life expectancy and lifetime medical expenditures. Popul Health Metr, under review). In fact, both smokers and obese participants had a shorter life expectancy than non-smokers and normal-weight participants, whereas their lifetime medical expenditure was conversely increased. These differences could be explained by the impact of these risk factors on quality of life. Using prospective data for 16 176 adult Caucasians in the USA,31 Reuser et al estimated life expectancy and years of life with and without activities of daily-living disability in relation to smoking and BMI, respectively. The results indicated that smoking decreased both life expectancy and years of life with activities of daily-living disability, whereas obesity decreased the former but increased the latter, thus leading to the conclusion that ‘smoking kills, and obesity disables’. Reuser's conclusion is concordant with the impact of walking on life expectancy and lifetime medical expenditure. Physical activity decreases not only mortality but also disability,5–13 17 18 32 leading to lower medical expenditure.33 For instance, walking has been significantly associated with a lower risk of cardiovascular disease,7 stroke,34 coronary heart disease,35 36 type 2 diabetes37 and hypertension.38 Consequently, walking also reduces expenditure on medication needed for these conditions.39
Strengths and limitations
This is the first study to have investigated the association between walking, life expectancy and lifetime medical expenditure. A major strength of this study was that we collected individual data on medical expenditure based on a cohort study of survival and medical-care utilisation, and its cost, for all participants,19 22 24 28 and the NHI covers almost all medical treatment in Japan. Second, we conducted a 13-year prospective observation of 27 738 Japanese adults aged 40–79 years living in the community who were free of any functional limitations or chronic conditions interfering with physical activity, with an accrued total of 285 342 person-years. Third, in order to reduce bias or reverse causation in that people did not walk because of functional limitations that also required medical expenditure, we excluded participants who, at the baseline, reported limited physical function or conditions interfering with physical activity. Additionally, to control for confounders, we also included various covariates in our Poisson regression model and linear regression model.
On the other hand, several limitations should also be considered. First, we assessed walking using a simple questionnaire in which we asked the participants to report only the time spent walking and did not ask about walking pace, distance walked or any distinction between walking for exercise and other reasons. Second, a longer time spent walking may be a reflection of performing more vigorous activity, making it difficult to distinguish the impact of walking from other types of physical activity. However, the present result did not change after multivariate adjustment.
Conclusions and policy implication
In summary, lifetime medical expenditure was shown to be decreased in participants who walked ≥1 h per day, despite the fact that they lived longer. Increased longevity resulting from a healthier lifestyle did not necessarily translate into an increased amount of medical expenditure throughout life. However, in the present study, around 50% of study participants walk <1 h per day. To increase their walking time, the recommendation of walking with a pedometer may be useful.40 An increase in walking time at the population level would bring about a tremendous change in people's health and medical cost. A campaign to encourage people to walk for longer and a program to make walking environments safer and more pleasant should be implemented. This intervention may extend life expectancy without apparently increasing lifetime medical expenditure, especially for men.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
Footnotes
Correction notice The “To cite: …” information and running footer in this article have been updated with the correct volume number (volume 1).
To cite: Nagai M, Kuriyama S, Kakizaki M, et al. Impact of walking on life expectancy and lifetime medical expenditure: the Ohsaki Cohort Study. BMJ Open 2011;1:e000240. doi:10.1136/bmjopen-2011-000240
Funding This study was supported by a Health Sciences Research Grant for Health Services (H21-Choju-Ippan-001, H20-Junkankitou (Seisyu)-Ippan-013, H22- Junkankitou (Seisyu)-Ippan-012, H23- Junkankitou (Seisyu)-Ippan-005), Ministry of Health, Labour and Welfare, Japan. MN is a recipient of a Research Fellowships of the Japan Society for the Promotion of Science for Young Scientists.
Competing interest None.
Patient consent Obtained.
Ethical approval Ethics approval was provided by the Ethics Committee of Tohoku University School of Medicine.
Contributors All authors contributed to the design of the study. MN, SK, MK, KO-M, TS and IT carried out the data collection. MN, SK, AH, MK and SH carried out the data analysis. MN, MK, KO-M, TS, AH, MK and SH wrote the report. SK and IT carried out a critical revision of the manuscript. All authors approved the final version of the report for submission.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.