Article Text

Abstract
Objective To assess the impact of the Women's Health CoOp (WHC) on drug abstinence among vulnerable women having HIV counselling and testing (HCT).
Design Randomised trial conducted with multiple follow-ups.
Setting 15 communities in Cape Town, South Africa.
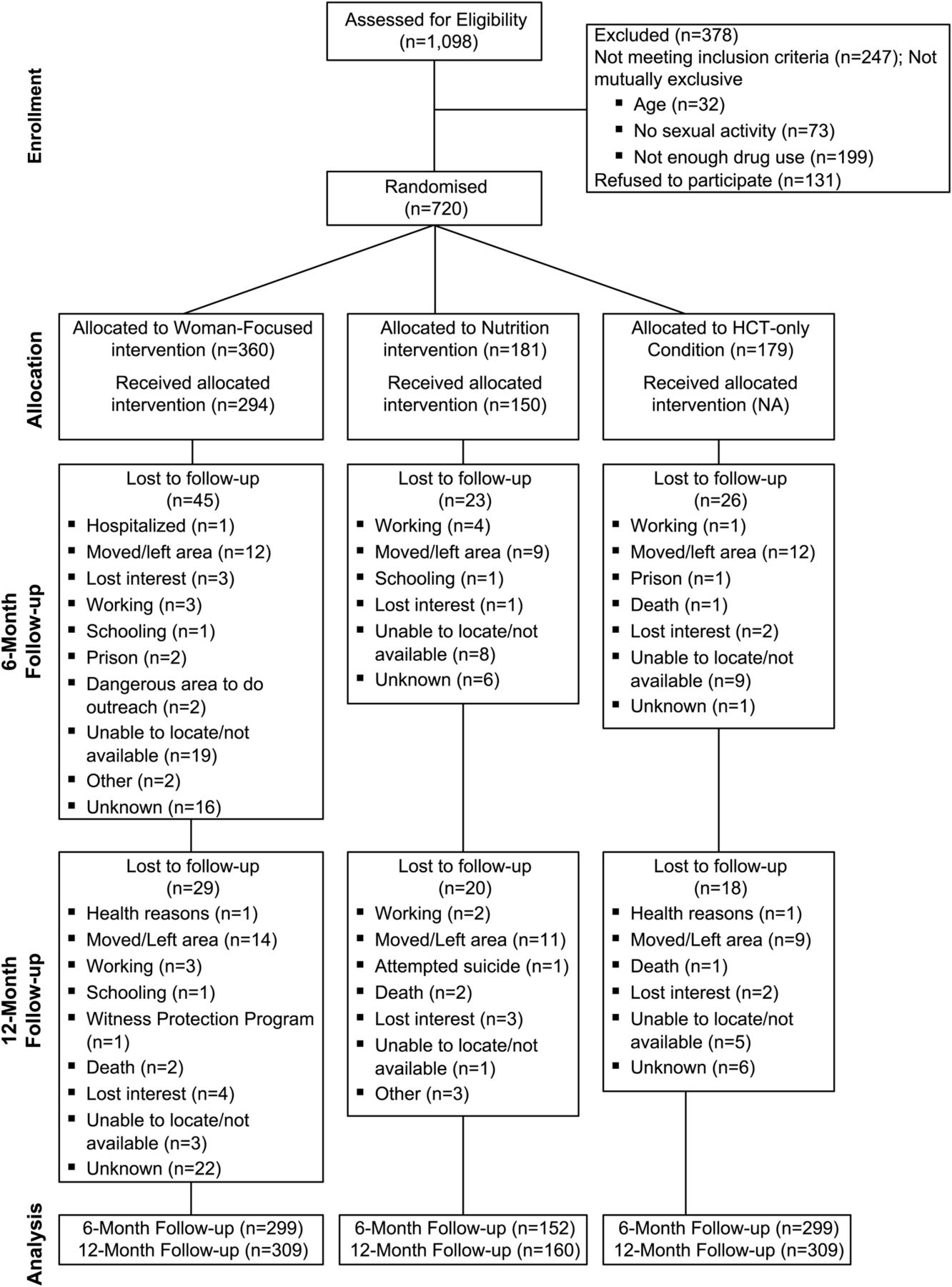
Participants 720 drug-using women aged 18–33, randomised to an intervention (360) or one of two control arms (181 and 179) with 91.9% retained at follow-up.
Interventions The WHC brief peer-facilitated intervention consisted of four modules (two sessions), 2 h addressing knowledge and skills to reduce drug use, sex risk and violence; and included role-playing and rehearsal, an equal attention nutrition intervention, and an HCT-only control.
Primary outcome measures Biologically confirmed drug abstinence measured at 12-month follow-up, sober at last sex act, condom use with main and casual sex partners, and intimate partner violence.
Results At the 12-month endpoint, 26.9% (n=83/309) of the women in the WHC arm were abstinent from drugs, compared with 16.9% (n=27/160) in the Nutrition arm and 20% (n=31/155) in the HCT-only control arm. In the random effects model, this translated to an effect size on the log odds scale with an OR of 1.54 (95% CI 1.07 to 2.22) comparing the WHC arm with the combined control arms. Other 12-month comparison measures between arms were non-significant for sex risk and victimisation outcomes. At 6-month follow-up, women in the WHC arm (65.9%, 197/299) were more likely to be sober at the last sex act (OR1.32 (95% CI 1.02 to 1.84)) than women in the Nutrition arm (54.3%, n=82/152).
Conclusions This is the first trial among drug-using women in South Africa showing that a brief intervention added to HCT results in greater abstinence from drug use at 12 months and a larger percentage of sexual activity not under the influence of substances.
Trial registration number NCT00729391 ClinicalTrials.gov
- Public Health
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
Drug use is a risk factor for risky sex, gender-based violence and HIV among vulnerable South African women.
-
Few brief woman-focused interventions for drug use have been evaluated in randomised trials in Africa.
-
A randomised controlled trial (RCT) was conducted to assess the impact of the evidence-based Women's Health CoOp (WHC) intervention on drug abstinence among vulnerable women in addition to having HIV counselling and testing (HCT) in Cape Town, South Africa.
Key messages
-
The WHC brief intervention was effective in reducing biologically confirmed drug use 12 months later when compared with an HCT-only intervention and an HCT plus equal attention nutrition control intervention.
-
Drug use often disempowers women from protecting themselves from adverse sexual consequences and victimisation. An intervention to reduce drug use in general, and particularly during sex, is an important first step to reducing risk.
-
This brief intervention has been shown to be effective in an RCT in an HCT setting in a low-to-middle-income country and among female drug users with 12-month outcomes. This intervention was implemented among a group of vulnerable women and can be easily translated to other hard-to-reach populations of drug users.
Strengths and limitations of this study
-
A strength is only 8.1% of the sample was lost to follow-up.
-
There were no significant differences in sexual risk and gender-based violence between the groups at follow-up.
-
HCT was carried out in all conditions and may have influenced the trend of increased condom use in all three study arms.
Introduction
Illicit drug use is a major public-health problem in South Africa and it is particularly problematic in the Western Cape Province.1–3 Drug use among poor South African women is of great concern because it places women at elevated risk for adverse-health outcomes such as gender-based violence and HIV infection.4–6 Women involved with drug use are vulnerable to violence and a range of risky sex behaviours, including exchanging sex for drugs or money5 and inconsistent condom use.6–8 In addition, high levels of gender inequity and the disempowerment of women in South Africa have a major impact on women's ability to protect themselves from violence to negotiate condom use with sex partners, and to take control over their drug use.9 ,10
Brief interventions in primary healthcare settings to reduce drug use have been evaluated extensively in high-income countries, with considerable evidence of their effectiveness among men.11 However, owing to insufficient research, the effectiveness of these types of interventions remains unproven in women who use drugs.
The Women's Health CoOp (WHC) intervention was initially developed in the USA as a brief HIV prevention intervention for African-American women who used crack cocaine12 and it is listed as the best-evidence intervention by the Centers for Disease Control and Prevention.13 ,14 Grounded in an empowerment framework and feminist theory, the WHC focuses on increasing women's knowledge (eg, about drug use and sex-risk behaviour) and skills (such as sexual negotiation and condom mastery) to help them reduce their risks for adverse health outcomes.14 ,15 Since its inception, the WHC has been adapted and tested for sex workers and other vulnerable women in Pretoria, South Africa,16 yielding reductions in alcohol use and partner violence and improvements in condom use at 6-month follow-up.14 ,16 However, as alcohol was the predominant substance of abuse among participants in the Pretoria study and because this sample lacked diversity, it is unclear whether findings from this study are generalisable to other vulnerable South African women. As Cape Town has an entrenched illicit drug scene characterised by polysubstance use and an especially high prevalence of methamphetamine use among vulnerable women,17 we conducted initial exploratory and pilot studies to demonstrate feasibility with drug-using women.18 ,19 Findings supported our plans to conduct a large randomised controlled trial (RCT) to test whether the WHC intervention yielded reductions in substance use and partner violence and improvements in sexual risk when applied to a more culturally diverse sample with more illicit drug use.
Methods
Study design and setting
The study design was a three-armed RCT set in Cape Town, South Africa, from September 2008 to January 2012. The necessary sample size for achieving acceptable statistical power was calculated to detect moderate effect sizes between the WHC arm versus the combined control arms ranging from 0.26 to 0.50 for the primary outcome, biologically confirmed drug abstinence. The sample size required was 900, randomly assigned to the three groups (450, 225 and 225). Recruitment took longer than anticipated, because considerable time was needed to build trust and rapport within the selected communities so that drug-using women felt comfortable to participate in the study. Resource constraints also limited the number of women we could enrol while still being able to conduct 12-month follow-up interviews within the project timeframe. Consequently, we enrolled 720 women in the trial, a smaller number of participants than originally intended. The observed power to detect differences with the final sample size and actual effect sizes in the study was 0.84 for abstinence from all drugs at 12 months. There were no interim analyses or stopping guidelines. All statistical tests presented herein are based on a two-tailed test, assuming an overall significance level of α=0.05.
Eligible participants were women of child-bearing age (18–33 years old), who were living in one of the target communities, had used at least two drugs (one of which could be alcohol) at least once a week for the past 3 months, were sexually active with a man in the past month and had not participated in the pilot study.19 To be selected as a target community, areas had to be defined as a disadvantaged community (ie, areas reserved for the use of ‘Black African’* or ‘Coloured’ persons under the Apartheid regime and systematically deprived of access to services and resources) with high levels of health and social issues as well as low income.20 A rigorous sampling plan was developed to ensure a more balanced recruitment of women across all 15 disadvantaged communities. Specifically, we used community population estimates to calculate the desired sampling targets for each community to ensure a more representative sample of women from different disadvantaged areas in Cape Town.
Peer outreach workers recruited participants, distributing marketing materials in areas frequented by potential participants, such as beauty parlours and corner shops/convenience stores. Outreach workers visited these locations regularly to enhance visibility and build rapport with community members. They approached potential participants and requested verbal permission to administer a brief screening instrument to assess study eligibility criteria. If eligible women were interested in the study, they were scheduled for an appointment for an intake interview where they were rescreened and enrolled in the trial after giving informed consent. After consent was obtained, participants took part in a baseline interview, provided biological specimens for testing and received HIV counselling and testing (HCT).These methods have also been described previously.21 ,22
Randomisation
After screening, enrolment and baseline assessment, participants were randomised by computer to the following arms: WHC (Experimental), Nutrition (Attention-Control) or HCT-only control. Project staff had no influence over the allocation process. Randomisation was determined in group blocks of eight to ensure that 50% of the participants were randomised to the WHC arm, 25% to the Nutrition arm and 25% to the HCT-only arm. The study was sufficiently powered to test half the sample in the WHC arm. The system was set up by the data manager based in the state of North Carolina in the USA and tested by key project staff before the start of the project. Staff members who conducted follow-up interviews were not involved in the intervention or baseline assessments; however, they were not blinded to study arm. The drug tests for the primary outcome were also not blinded.
Interventions
The Pretoria WHC intervention14 ,16 was first adapted for drug-using women in the Western Cape on the basis of information obtained during focus groups of drug-using women18 and then piloted in a small trial.19 The WHC intervention is a four-module intervention conducted over two sessions, with each module lasting approximately 1 h. This intervention is delivered by a peer educator who serves as the interventionist to groups of 4–6 women. The interventionist presents health information to improve women's knowledge on key topics, provides participants with information and strategies to build skills to reduce their health risks (eg, condom mastery skills) and gives participants an opportunity to practice these new skills through role-playing and rehearsal.
Specifically, session 1 provides participants with information about drug use and risks (module 1) and how certain sex behaviours can increase HIV risk. This session also teaches women sexual negotiation skills as well as corrects male and female condom use (module 2). Session 2 focuses on relationship power as well as communication and negotiation skills with male partners (module 3), including myths about rape and violence against women and strategies for avoiding potentially violent situations (module 4). Session 2 concludes with developing a personalised risk-reduction plan for each participant that addresses alcohol and other drug use, condom use and violence. Women are also referred for drug abuse treatment and for other health support as needed. The retention rate for the WHC intervention was 81.7% (n=294/360).
The Nutrition intervention was an equal attention-control arm originally sourced from a US curriculum and adapted with available local food sources and to the neighbourhood context.23 This intervention is delivered by a peer interventionist to groups of 4–6 women and teaches them about the basic food groups, healthy food preparation and how to develop a menu while shopping with little money. The intervention also teaches participants about exercise. The retention rate for the Nutrition intervention was 82.9% (150/181).
Both of these adapted interventions were reviewed by an expert panel and a community advisory board in Cape Town prior to being implemented in the field. Participants randomised to the third intervention arm received only HCT comprising standard HIV pretest and post-test counselling in which participants are prepared for the test and the possible results of the test. No additional counselling on other topics is provided to participants during HCT.
Outcome measures
We assessed participants at baseline and at 3, 6, 9 and 12-month postrandomisation. In this article, we present the 6-month and 12-month follow-up outcomes for the primary outcome involving drug use. However, we also present some of the related secondary outcomes, such as impaired sex from drug use. No biological tests were conducted at 3-month and 9-month follow-up appointments as the primary purpose of these appointments was to maintain retention and rapport. The primary outcome was a biologically confirmed abstinence from drug use at 12 months. Participants gave a urine specimen that was tested using the four-panel Reditest drug test (Redwood Toxicology Laboratory) for methamphetamine, cocaine, opiates and THC (marijuana). Urine was also tested for Mandrax (methaqualone) by a drug testing laboratory in Cape Town using standard gas chromatography techniques to test for the presence of methaqualone in urine. A participant testing negative for all substances was classified as abstinent for drugs.
Additional outcomes were self-report measures of sex-risk behaviour and victimisation, assessed using a standard questionnaire administered by study staff using Computer-Assisted Personal Interviewing. The survey asked how often the participants had had sex with their main partner (and casual partners) in the past month and how many sex acts were protected. Responses were coded as having had protected sex with the main partner if all main partner sex acts were protected, and coded as protected sex with a casual partner if all sex acts with casual partners were protected. Participants without a casual partner were coded as missing.
Participants were asked items about intimate partner violence: being slapped, pushed, shoved, kicked, hit with a fist or something else; dragged; or beaten, choked or burned. Any participant experiencing intimate partner violence in the prior 6 months was coded as physically abused.24 To measure impaired sex, participants were asked: “This last time you had sex, did you use drugs (including cannabis) or alcohol just before or during sex?”’
Ethical approval for the study was granted by the Institutional Review Boards at RTI International and Stellenbosch University's Faculty of Health Sciences. The study obtained informed consent, which was signed at each data collection point. Participants were provided with refreshments and a grocery voucher valued at ZAR40 (USD5.71) for their time at baseline, ZAR60 (USD8.57) at 6-month follow-up and ZAR80 (USD14.29) at 12-month follow-up. Health kits with condoms and toiletries were provided to participants at follow-up appointments. Referrals for HIV services were provided as necessary. Any adverse events were reported to the South African Project Director and the Principal Investigator, who advised staff on the appropriate action to take, and to the IRB and the funding agency if necessary. In addition, the appropriate documentation was completed by project staff members and reported, as dictated in the field operations manual and IRB.
Data analysis
Baseline characteristics to ascertain whether there were differences between study conditions and overall drop out by condition were summarised as percentages (or means) and compared between groups, with t tests for continuous variables and χ² tests for categorical variables. SAS V.9.2 was used for all statistical analyses. The primary study statistician (SN) was not blinded to treatment arm assignment. Therefore, a second study statistician (AML) ran parallel verification analyses and was blinded to arm assignment.
The primary analytic strategy used to estimate the impact of treatment on each of the main study outcomes was a generalised-linear mixed model, with repeated measures observed at baseline, months 6 and 12. This resulted in a baseline observation and two follow-up waves from which to examine the effect of the intervention on primary and secondary outcomes. The planned comparisons involved differences at 6 and 12 months between (1) the Control arm versus Nutrition, (2) the WHC arm versus Nutrition and (3) the WHC arm versus the Control arm. We also conducted additional tests between the WHC and the combined control conditions (Control and Nutrition). The intent-to-treat (ITT) analyses are presented here with cases that were not observed because of attrition coded to the negative outcome. As a stability check for attrition, we also examined two alternative methods (Last Observation Carried Forward and All Available Cases).The results were highly stable across methods so the standard ITT approach is presented here.
The models included fixed effects for treatment condition (HCT-only control, Nutrition and WHC arms), time (baseline, 6 months and 12 months) and a treatment-by-time interaction. The covariate race was included in the mixed model because it predicts the probability of missingness and/or dropout and the Full Information Maximum Likelihood estimator uses information about race to remove bias associated with dropout. This approach uses information about the dropout mechanism to adjust for the missing observations of each participant.
The primary statistical tests were the prespecified contrasts between the intervention arms at each time point. As the recruitment of respondents was nested within 15 communities, the mixed model also included a random effect for community. For dichotomous outcomes, a logit link was used for predictors to the binary outcome. The magnitude of the estimated differences between arms within each of the time-specific contrasts was calculated on the log-odds scale and exponentiated to create ORs as a standardised measure of effect size. For the continuously distributed outcome, the mixed model was used with an identify link transformation and planned contrasts.
Results
Figure 1 presents the trial profile. Attendance records showed that 18% of the participants allocated to the WHC arm and 17% of participants allocated to the Nutrition arm did not attend their intervention sessions. The 6-month and 12-month follow-up percentages for women in the WHC, Nutrition and HCT-only arms were all greater than 85%. The follow-up percentages at 12-month follow-up were slightly higher than for the 6-month follow-up, as women could return to the study even if they had missed their 6-month follow-up appointment. Among study participants, six deaths occurred, divided equally across the study arms. All deaths were caused by HIV-related complications or tuberculosis. Among the participants, three were sent to prison (two from the WHC arm and one from the HCT-only control arm). Convictions were for house breaking, armed robbery and possession of an illegal firearm or drugs. None of the deaths or arrests was linked to study participation. There were no serious adverse events related to the study.

Flow diagram for the Western Cape Women's Health CoOp Study.
Participants’ baseline characteristics are shown in table 1. Characteristics were similar across the three intervention arms; except for methamphetamine use, where the Nutrition arm had higher usage than either the WHC arm or the HCT-only control arm (p=0.01; table 1).
Participant demographic characteristics, by treatment condition
The descriptive statistics for the study outcomes by condition are presented in table 2. The estimated treatment effects by study condition and the 95% CIs around the pairwise comparisons between treatment conditions are shown in figure 2. There were differences between the intervention arms for drug abstinence. At the 12-month endpoint, 26.9% of the participants in the WHC arm were abstinent compared with 16.9% in the Nutrition arm and 20% in the HCT-only control arm. In the random effects model (ie, forest plot of effects shown in figure 2), this contrast was translated to an effect size of OR=1.54 (95% CI 1.07 to 2.22; Cohen's d=0.238) for the comparison between the WHC arm and the combined Nutrition arm and HCT-only control arm. There were changes in the proportion of drug use between baseline and the 12-month follow-up in all three arms, but the relative change in the WHC arm was higher than the combined Nutrition and HCT-only control arms. When the WHC arm was compared with the Nutrition arm and HCT-only control arm separately, no differences were found in drug abstinence for the comparison with the HCT-only control arm, but the proportion abstinent was higher in the WHC arm than the Nutrition arm at 12 months (OR 1.73 (95% CI 1.06 to 2.81); Cohen's d=0.302).
Baseline, 6-month and 12-month key outcome measures, by intervention condition

{kind=link}
{kind=link}
Plot of treatment main effects, by study outcomes.
There were differences between the intervention arms on impairment during last sex. At 6 months, the proportion of women in the WHC arm reporting they were not impaired during their last sexual encounter was lower than in the Nutritional arm and HCT-only arm combined. The difference translates to an OR of 1.32 (95% CI 1.02 to 1.84; Cohen's d=0.153). Substantively, 65.9% of participants in the WHC arm reported that they were sober during their last sex encounter compared with 54.4% of participants in the Nutrition arm. There was a pattern of significant changes over the two time points, with an increase in the number of participants reporting sobriety at last sex in the WHC arm (p<0.001). There were no differences by intervention arm or time for other outcomes.
Discussion
Drug use is a major problem in the Western Cape Province of South Africa, with particular concern about escalating methamphetamine use.1 ,7 Although we have shown different patterns of drug use at baseline,17 ,22 the primary outcome of drug use abstinence at 12 months after the brief WHC intervention and the reduced prevalence of self-reported drug-impaired sex at 6 months are important findings. Although it did not reduce other secondary outcomes involving sexual risk taking or the proportion of women experiencing partner violence at 12 months more than the control groups, these reductions in illicit-drug use and drug-impaired sex are important initial steps in addressing these health risks. Women are more vulnerable in this setting, and because drug use exacerbates problems and often further disempowers women to be unable to protect themselves sexually or from victimisation, these findings provide a basis on which to build. Therefore, we can report both strengths and limitations from this brief women's intervention.
Strengths
This study is possibly the first RCT of a brief intervention to reduce women's drug use after 12 months in an HCT field setting in sub-Saharan Africa. The findings are generally supported by those of a 6-month evaluation of the WHC intervention among women in Pretoria who were not sex workers.14 Additionally, the finding that the WHC intervention in this region was efficacious for reducing biologically measured drug use in an impoverished and very violent area is noteworthy. While there was a trend of declining drug-impaired sex at 6 months, which is potentially important for HIV prevention, this trend was neither sustained at 12-month postintervention nor did the interventions impact on violence-related outcomes. Although the original adaptation of the WHC targeted more alcohol-abusing sex workers, who notably have heightened sexual risk and are victimised by numerous partners,5 ,9 the main outcomes showed significant reductions in these risk behaviours. Women within township communities in Cape Town face illicit drug use as a major problem1 ,3 with earlier studies highlighting the high prevalence of methamphetamine as well as polydrug use among vulnerable women from disadvantaged Cape Town communities.17 They also face greater exposure to community violence, particularly traditional male attitudes and gang-related violence.25 These contextual differences between the Pretoria WHC study and the current study could have contributed to our failure to find significant reductions in partner violence victimisation and sustained improvements in drug-impaired sex. In addition, we conducted additional analyses (not presented here) to understand whether our results were robust to differences in the composition of Blacks and Coloured respondents in the intervention. The findings indicated no significant differences by condition, so the intervention appears to affect both racial groups. Future studies might consider testing whether the addition of a booster intervention session after the 6-month follow-up yields sustained reductions in drug-impaired sex. In addition, brief interventions such as the WHC generally focus on individual-level contributors to risky behaviours and as such are unlikely to address structural and contextual determinants of sexual-risk behaviour or violence. As part of addressing the relationship context of sexual-risk behaviours, future studies might incorporate the relationship with male partners into the intervention. Studies should also consider examining structural drivers of behaviour change among high-risk populations, including the role that neighbourhoods and social networks play in hindering and facilitating behaviour change.26 In addition, future iterations of the WHC intervention may need to address structural determinants of partner violence and victimisation;26 particularly because only a gender-focused structural intervention has been effective in reducing partner violence in South Africa with disadvantaged women.27 ,28 Nonetheless, the gender sessions of the WHC intervention may have been of considerable value to women.
Limitations
This RCT has several limitations that might affect the interpretation of the results. First, participants in all three arms received HCT; consequently, it is possible that the trend observed across all arms of greater condom use with a main sex partner could be attributable to HCT. Second, there were more methamphetamine users at baseline in the Nutrition arm than either the WHC arm or the HCT-only control arm, possibly making change more difficult. However, the proportion of participants with any biologically confirmed drug use did not differ and there were no differences in drug use between the Nutrition arm and the HCT-only control arm at 6 or 12 months. Third, the study focused on individual behaviour changes and it is possible that these changes are not sustainable as they do not focus on contextual issues as well. Also, the study was not powered to detect the impact on HIV incidence. Fourth, the follow-up period was for 12 months; consequently, we do not know if the intervention effects were sustained beyond that period. Despite considerable efforts at cohort retention, 8.1% of participants (58 women) failed to contribute any data for the outcome analysis. This compares favourably with other behavioural RCTs. For example, one study lost 15% to follow-up.28 As follow-up rates and intervention attendance rates were similar in the WHC intervention arm and HCT-only control arm, this is unlikely to have biased the results. Finally, the study addressed gender inequality and gender-based violence. However, working only with women and not their sexual partner meant that these issues could not be addressed with men. Future studies should consider working with women and their sex partners so that these issues can be addressed within the context of the relationship.
Implications
The WHC brief intervention was effective in reducing drug use among participants 12 months later when compared with an HCT-only intervention and an HCT plus equal attention control intervention. In high-income countries, brief screening interventions for alcohol abuse have been shown to be effective in primary healthcare settings,11 but such interventions for other drug use have been researched very little.29 To our knowledge, this is the first time a brief intervention has been shown in an RCT to be of use in an HCT setting in a low-to-middle income country and among female drug users a year later. Further, this intervention was implemented among a group of vulnerable women and can be easily translated into other settings with hard-to-reach populations of drug-using women. Consequently, this brief intervention has the potential for broader dissemination among drug-using populations elsewhere. Further, if it is scaled up widely, it may aid efforts for HCT and to reduce drug abuse among vulnerable women from high-risk communities.
Future work
Future studies plan to focus on structural drivers of behaviour change among high-risk populations. This includes plans to address structural and social networks in different neighbourhoods of a community. While all the women in this study can be described as high-risk and vulnerable, a future aim of studies with this group will be to explore the characteristics of the sample in more depth, in order to make conclusions about typologies of women that had successful outcomes.
Acknowledgments
We wish to thank all our project staff and the women participants. We would also like to thank Jeffrey Novey, MPH, for his editorial assistance. Mr Novey is a Senior Editor in RTI International's Knowledge Translation and Strategic Communication division and he was compensated for his time editing the article.
References
Footnotes
-
Contributors WMW designed, planned, took part in all aspects of the study and manuscript and had full access to all the data in the study and maintains the responsibility for the integrity of the data and the accuracy of the data analysis. She was responsible for the final writing of the manuscript and the revised manuscript. RJ was a Co-investigator and took a major role in developing the analyses plans, was a major contributor to writing and reviewed all analyses. SPN and AAML conducted the outcomes analyses. TK was responsible for all instrumentation throughout the study and conducted the preliminary analyses. BM was a Co-investigator and the Project Director, and she was a major contributor to the writing. FAB was the Associate Project Director, was involved in all aspects of the study and contributed to the writing of the manuscript. TC was the Project Manager and managed the data collection, wrote the Methods section, developed the CONSORT model and supported the overall writing. CP was a Co-investigator and helped to finalise the writing of the findings and conclusions. All authors read and approved the final manuscript prior to submission.
-
Funding This research was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), National Institutes of Health, Unites States Department of Health and Human Services (HHS), grant number R01HD058320. The interpretations and conclusions presented here are those of the authors and do not necessarily represent the position of NICHD or HHS. The funding organisation played no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; or preparation, review or approval of the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Institutional Review Boards at RTI International in the United States and Stellenbosch University's Faculty of Health Sciences in South Africa.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.
-
↵* The terms “Black African” and “Coloured” refer to demographic markers that were chosen for their historical significance and their continued relevance in terms of tracking progress in addressing health disparities in South Africa. “Coloured” refers to a grouping of people of mixed race ancestry that self-identify as a particular ethnic and cultural grouping in South Africa.