Article Text

Abstract
Introduction Rotavirus is the most common cause of severe gastroenteritis in infants and young children worldwide. Currently 67 countries include rotavirus vaccine in childhood immunisation programmes, but uptake in Western Europe has been slow. In July 2013, rotavirus vaccine was introduced into the UK's routine childhood immunisation programme. Prior to vaccine introduction in the UK, rotavirus was estimated to result in 750 000 diarrhoea episodes and 80 000 general practice (GP) consultations each year, together with 45% and 20% of hospital admissions and emergency department attendances for acute gastroenteritis, in children under 5 years of age. This paper describes a protocol for an ecological study that will assess rotavirus vaccine impact in the UK, to inform rotavirus immunisation policy in the UK and in other Western European countries.
Methods and analysis In Merseyside, UK, we will conduct an ecological study using a ‘before and after’ approach to examine changes in gastroenteritis and rotavirus incidence following the introduction of rotavirus vaccination. Data will be collected on mortality, hospital admissions, nosocomial infection, emergency department attendances, GP consultations and community health consultations to capture all healthcare providers in the region. We will assess both the direct and indirect effects of the vaccine on the study population. Comparisons of outcome indicator rates will be made in relation to vaccine uptake and socioeconomic status.
Ethics and dissemination The study has been approved by NHS Research Ethics Committee, South Central-Berkshire REC Reference: 14/SC/1140. Study outputs will be disseminated through scientific conferences and peer-reviewed publications. The study will demonstrate the impact of rotavirus vaccination on the burden of disease from a complete health system perspective. It will identify key areas that require improved data collection tools to maximise the usefulness of this surveillance approach and will provide a template for vaccine evaluations using ecological methods in the UK.
- IMMUNOLOGY
- STATISTICS & RESEARCH METHODS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Strengths include use of data from multiple health systems that will allow examination of the relative impact of vaccination on the various health providers and communities rather than the individual. These multiple data sources will provide robustness, enabling easier identification of outliers from overall trends.
-
The study will include all ages for rotavirus and all-cause gastroenteritis incidence for 3 years postvaccination, thereby minimising confounding caused by yearly variance in rotavirus numbers.
-
Additionally the study is powered to measure the indirect (herd) effect on hospital admissions, and while the majority of studies have focused on this, this study will also provide evidence for the indirect effect in emergency departments and community settings.
-
The study will be limited by the ecological before and after design, and the difficulties of ascribing causality to vaccine, as well as the inherent risks of bias and confounding in observational studies particularly due to underlying secular trends.
-
Use of syndromic indicators that are non-specific to rotavirus will limit the study to measuring large effects rather than small variations for emergency departments and community health outcome measures.
Introduction
Rotavirus is the most common cause of severe gastroenteritis in infants and young children, responsible for an estimated annual 453 000 deaths worldwide among children under age 5 years, with over 90% of deaths occurring in the developing countries.1 In the UK, rotavirus gastroenteritis (RVGE) is seasonal and most cases occur between February and April each year. Rotavirus is estimated to result in 750 000 diarrhoea episodes and 80 000 general practice (GP) consultations each year in the UK,2 together with 45% and 20% of hospital admissions and emergency department (ED) attendances for acute gastroenteritis (AGE), respectively, in children under 5 years of age.3 The economic cost of RVGE to the health service is estimated to be approximately £14 million per year in England and Wales.3 At Alder Hey Children's NHS Foundation Trust, Liverpool, UK, rotavirus is a major cause of community-acquired and healthcare-associated diarrhoea; in a 2-year prospective study among hospitalised children, rotavirus was detected by RT-PCR in 43% of community-acquired and in 31% of healthcare-associated gastroenteritis cases.4 AGE hospital admissions are known to have a positive correlation with socioeconomic deprivation5 and globally the burden of severe RVGE is much higher in low-income countries. However, RVGE has not yet been correlated with socioeconomic deprivation in the UK.
In July 2013, the Department of Health introduced a rotavirus vaccine into the UK's routine childhood immunisation programme.6 ,7 The live-attenuated, two-dose oral monovalent vaccine (Rotarix, GlaxoSmithKline Biologicals, Belgium) is administered at 2 and 3 months of age. Clinical trials in Europe and the Americas with both currently licensed rotavirus vaccines (Rotarix and a pentavalent vaccine RotaTeq developed by Merck) led to a WHO recommendation in 2007 to vaccinate children in these regions.8–10 Subsequent trials in Africa and Asia led to an extension of the recommendation to include all children worldwide.10–12 At present more than 60 countries include a rotavirus vaccine in childhood immunisation programmes.13 Introduction of rotavirus vaccination in Western Europe has been slow however, with only Austria, Belgium, Finland, Luxemburg and most recently the UK having rolled out universal rotavirus vaccination programmes to date.14 Based on the uptake of other routine childhood vaccinations in the UK, coverage of over 90% would be expected for rotavirus vaccine;15 initial figures for England indicate 93% uptake for first dose and 88% for the second dose of rotavirus vaccine.16
Clinical trials in middle-income and high-income countries demonstrated high (>85%) efficacy against severe RVGE.10 The introduction of rotavirus vaccines in the immunisation programmes of these countries has demonstrated direct benefits on a par with those observed in clinical trials, with significant reductions in diarrhoea hospitalisations.17 An unanticipated but beneficial consequence of rotavirus vaccination has been the reduction of rotavirus disease in unvaccinated individuals (herd protection), likely due to reduced virus transmission. Such ‘indirect benefits’ include reduced disease in non-vaccinated older children and adults who were not thought to sustain a significant burden of rotavirus disease.18 In the UK, the burden of RVGE in older children and adults is difficult to estimate but admissions for AGE are 2 per 1000 population in 5–14-year-olds and 7 per 1000 in those 15+ years.19 Hence monitoring changes in AGE incidence in non-vaccinated older children and adults is critical to assess indirect impact.
Ecological rotavirus vaccine effectiveness studies have primarily focused on mortality, hospitalisations and laboratory detections as a measure of burden.20–27 Severe cases of rotavirus infection will often end up in hospital and receive full diagnostic evaluation. However, many cases of rotavirus infection, particularly in older children and adults, will not attend hospital but will be seen by primary and community healthcare providers. Therefore, in order to better understand the burden of RVGE and AGE on all ages and the impact of routine immunisation on the health system, it is crucial to examine routine data sources for all health service providers in a defined study area. Taking advantage of a range of regional healthcare facilities in Merseyside, UK, we describe a protocol for an ecological study which will use a ‘before and after’ approach allowing comprehensive evaluation of the direct and indirect vaccine impact following the introduction of the monovalent rotavirus vaccine into the UK's routine childhood immunisation programme. We will investigate the relationship between socioeconomic deprivation, and vaccine uptake and disease burden. These data will provide evidence to support future rotavirus vaccination in the UK and will inform rotavirus immunisation policy in other Western European countries.6
Methods
Study aim
Routine data sources will be used to estimate the direct and indirect effects of monovalent rotavirus vaccination on gastroenteritis indicators in the population of Merseyside, UK, and their relationship to vaccine coverage and sociodemographic indicators. We also hope to identify the key areas that require extended and improved data collection tools to maximise the usefulness of this surveillance approach. The main outcome measures are:
-
Laboratory detections of rotavirus in faecal samples;
-
Admissions to hospital for RVGE or AGE;
-
Attendances to EDs for AGE;
-
Number of nosocomially acquired cases of RVGE;
-
GP and community consultations for diarrhoea and AGE in children less than 5 and in all ages;
-
Routine rotavirus vaccine coverage mapping by small area geography;
-
Relative contribution of direct (those vaccinated) and indirect (not vaccinated) effects to overall vaccine benefit in health system usage for both RVGE and AGE;
-
Relationship between socioeconomic deprivation, vaccine uptake and RVGE/AGE incidence.
Study setting and location
The study will be conducted in the large metropolitan area of Merseyside in North West England which contains the city of Liverpool. Merseyside has a population of nearly 1.4 million people, with approximately 80 000 of its population under 5 years of age. Socioeconomic deprivation within Merseyside is variable but over 60% of its population live in a more socioeconomically deprived area than the England average (figure 1).28 Vaccination uptake for most routine childhood vaccinations is also variable in small areas, but overall Merseyside has uptake above the average for England.15 Healthcare for the population is self-contained with the region and including a specialist paediatric hospital. Further detail of healthcare provision is provided below.

Socioeconomic deprivation in Merseyside. Produced using the English Indices of Deprivation 2010, national quintiles for the Index of Multiple Deprivation.19
Study overview and choice of study designs
The study will employ an ecological design, utilising routine health surveillance data before and after rotavirus vaccine introduction. The evaluation incorporates interrupted time series analyses of outcome indicators across the study population. Comparisons of outcome indicator rates will be made between communities with high vaccine uptake and those with lower vaccine uptake and the relationship with socioeconomic deprivation. The ecological study approach allows population-based rates of outcomes to be compared in space and time using vaccine uptake and community-level socioeconomic deprivation as covariates.
Study data
The National Health Service (NHS) in England and other government service agencies collect a range of administrative and healthcare data which is held at both local service level and centrally. Figure 2 outlines the data sources that will be used for the evaluation and table 1 shows the case definitions.

Schematic of study data sources and outcome measures. Data sources cover a variety of healthcare providers at different levels of the health system. This shows from which data sources outcome measures will be obtained (LSOA, Lower Super Output Area).
Case definitions by health data set
Hospital admission and ED attendance data will be obtained from hospital episode statistics (HES),19 which record all inpatient admissions in NHS hospitals in England. The study will therefore measure hospitalisations and ED attendances for residents of Merseyside receiving care in hospitals throughout England.
The study will obtain GP consultation data for diarrhoea or gastroenteritis from Clinical Commissioning Groups covering Merseyside or from government held sentinel surveillance systems. Community consultations for diarrhoea and gastroenteritis at ‘Walk-in Centres’ will be sourced from NHS Community Health Trusts. Walk-in Centres are primarily nurse-led primary care facilities for illness and injuries without need for prior appointment.
RVGE at Alder Hey Children's NHS Foundation Trust (Alder Hey) in Liverpool is classified as community acquired or nosocomial. Alder Hey's footprint covers the majority of Merseyside's children, so these data will enable evaluation of the effect of rotavirus vaccination on nosocomial rotavirus infection in children across Merseyside.
Laboratory detections of rotavirus from Public Health England Laboratory surveillance covering Merseyside residents will be included in the analysis. Other causative agents of AGE identified through laboratory testing including, for example, norovirus, adenovirus and astrovirus will also be extracted for analysis.
Each data set will cover at least 3 years either side of vaccine introduction. All data will be pseudoanonymised to allow distinction of records but no linking of data sets or identification of individuals will be undertaken. All data will be either geocoded from postcode to small statistical geographical community units termed Lower Super Output Areas (LSOAs) or sourced with this geography. LSOAs consist of approximately 1500 persons and denominator populations will be derived from the Office of National Statistics (ONS) mid-year population estimates by LSOA.29 Indicators of socioeconomic deprivation at LSOA level will be measured using the English Indices of Deprivation. The UK Department for Communities and Local Government produce the English Indices of Deprivation using census and other local administrative data.28 Rotavirus vaccination uptake data will be sourced from the Child Health Information System (CHIS) which is held by community NHS health Trusts in Merseyside. Records of doses of vaccinations given as part of the UK childhood vaccine schedule are recorded in CHIS for each child.
Quality control
Data sources such as HES and laboratory detections will be influenced by testing practices; for instance, testing of some organisms is more likely to occur at certain times of the year. In the hospital admission data set, it is possible that some cases of RVGE will not be coded as rotaviral enteritis (ICD10: A08.0) and may be classified as other unspecified either due to an absence of laboratory confirmation or misclassification/miscoding. In order to attempt to quantify this information bias, the investigator team will perform quality control on hospital admissions and laboratory detections at the lead NHS Trust hospital site (Alder Hey). Using a sample of cases from at least 3 years, those cases with a laboratory confirmation will be checked against clinical records and clinic coding and those coded as ICD10 A08.0 rotaviral enteritis will be cross-matched against laboratory detections. Based on the results of this assessment, it may be necessary to adjust the recorded number of hospital admissions for any ascertainment bias identified.
Ethical considerations
The study has been approved by NHS Research Ethics Committee, South Central-Berkshire REC Reference: 14/SC/1140. Data sharing agreement will be obtained between PHE, participating NHS Trusts and the University of Liverpool. Research governance approval will be sought form all participating NHS Trusts and Clinical Commissioning Groups.
Data analysis
Changes in trends of primary care consultations, community consultations, ED attendances, hospitalisations and rotavirus detections will be explored using interrupted time series analysis. Moving averages will be examined to highlight any long-term trends while smoothing out any short-term fluctuations. Standardised population-based rates for a minimum of a 3-year period prior to vaccination and year on year after vaccination (for 3 years) will be compared. For the regression analysis, Poisson regression will be used. We will first compute monthly population-based rates that are ‘expected’ to occur in the absence of a rotavirus vaccination programme by fitting the model to prevaccine data. We will then adjust for seasonality. The model will be used to estimate ‘expected’ population-based rates after vaccination and we will then compare with ‘observed’ population-based rates. We will then calculate rate ratios and assess the magnitude of decline in rates. Using a Poisson regression model, and including demographic and vaccine uptake indicators, we would be able to predict impact of vaccination on the AGE and RVGE indicators at various services and vaccine uptake levels. Potential data biases will be controlled for by the access and analysis multiple health data sources over a minimum of 6 years.
Environmental factors which may influence rotavirus incidence and seasonality are difficult to identify or indeed quantify. To account for any potential environmental confounders, correlation of laboratory confirmations of viral gastroenteritis-causing organisms (eg, norovirus, astrovirus) with rotavirus laboratory confirmations will be established. If a significant correlation between any other viral gastroenteritis and rotavirus can be identified, the resulting correlation coefficients will be used to estimate relative contribution of vaccination and undefined environmental factors to any changes in rotavirus incidence. Furthermore, we will explore a potential reciprocal increase in other viral agents (eg, norovirus) due to a decrease in circulating rotavirus, and potential increase in susceptible individuals particularly in those under 5 years of age.
Power calculation
Based on hospital admissions for RVGE in 2012 obtained from HES data, the estimated rate of RVGE hospitalisation is approximately 1 per 1000 children under age 5 years in England.19 Assuming high vaccine uptake rates (ie, 95%), similar to uptake of other routine childhood vaccines in Merseyside, we used a one sample comparison of proportions for a two-sided test to calculate the power estimates (table 2). Studies from other high-income countries on the population effects of rotavirus vaccination have shown reductions in hospital admissions of over 50% in children under 5 years of age.14 Assuming a similar reduction in Merseyside, this study has over 90% power to detect a significant change in RVGE hospital admissions.
Predicted power of study for main outcome (hospitalisation rate) in Merseyside and selected subdistricts
The study is also powered for detecting an indirect effect in adults. Using an AGE hospital admission rate of 7 per 1000 population aged 15+ years,19 we would expect power to be at least 0.97 for Merseyside at assumed hospitalisation rate reductions post vaccination of 5%, 8% and 10%. Additionally, for GP consultations for AGE in children under 5, a power of 0.89 and 1 can be achieved, for assumed consultation rate reductions post vaccination of 5% and 10% respectively. No formal power calculations have been undertaken for other end points under study.
Timeline
The study will be conducted over a 3-year period beginning in April 2014. Prior to the start of the study, administrative procedures will be undertaken including data sharing agreements, consultation with data providers, database development for storing all sourced data, data analysis and report writing (including interim yearly, final and peer review papers).
Project governance
A stakeholder group within Merseyside will be established to enable effective achievement of the project objectives and ownership by the professional community. The stakeholder group will include representatives from: Liverpool Health Partners;30 Liverpool Community Health NHS Trust;31 NHS England Merseyside Area Team Screening and Immunisation Team;32 Alder Hey Children's NHS Foundation Trust33 and Public Health England34-Liverpool.
Dissemination of research findings
The findings will be presented at professional and scientific conferences. The results will also be published in peer review publications. Interim and final reports will be submitted to the funders and the stakeholder group.
Discussion
This study will enable demonstration of a complete health system perspective of the impact of rotavirus vaccination on the burden of disease in Merseyside, UK. It aims to study both direct and indirect effects of routine rotavirus vaccination. The study will also enable data on vaccine efficacy to infer the relative contribution of RVGE to AGE primary care, and emergency care consultations. Furthermore as data will be linked to specific geographical units, for which information on socioeconomic deprivation and vaccine uptake is available, we will be able to explore the association of these with disease burden. Quality control procedures contained within the study will provide a means of adjusting analysis for information bias and also enable identification of the key data collection issues that require improvement to maximise the usefulness of this surveillance approach. It is also hoped that this study will provide a learning resource and template for similar ecological approaches to examine effectiveness of other vaccines in the UK in the future.
Strengths
A whole health system approach in a geographically defined area provides a number of strengths. Using data sets from a range of healthcare providers within a health economy will allow us to examine the relative impact of vaccination on the various health providers rather than the individual. The use of multiple data sources to measure independent indicators of vaccination effect will also provide robustness, enabling easier identification of outliers from overall trends.
Since there is annual variability in the number of rotavirus cases, it is imperative to conduct surveillance of rotavirus incidence over a number of years prevaccine and postvaccine introduction. This study will provide a mechanism to do this as it will cover three rotavirus seasons postvaccine introduction. Thus, cofounding caused by yearly variance in rotavirus numbers will be minimised.
There are limited published data describing the indirect effect of routine vaccination on unvaccinated older children and adults and the majority of studies have focused on hospital admissions. As this study will collect data for all ages and cover RVGE and AGE incidence 3 years postvaccination, it will provide sufficient data for measurement of the indirect effect on hospital admissions. Additionally, while the majority of studies into the indirect effect of vaccination have focused on hospital admissions, this study will examine indirect effects in EDs and community settings. This is particularly important as it is perhaps more likely that moderate/severe RVGE in unvaccinated older children and adults will be treated at EDs and through community consultations.
Another potential strength of the study is the ability to conduct analysis at small community (LSOA) level. This will enable small area sociodemographic information such as socioeconomic deprivation to be included in the analyses as a covariate at the lowest possible unit of analyses other than the individual. Thus, allowing the exploration of the association between socioeconomic deprivation, burden of RVGE/AGE and vaccine uptake while limiting the ecological fallacy of analysis.
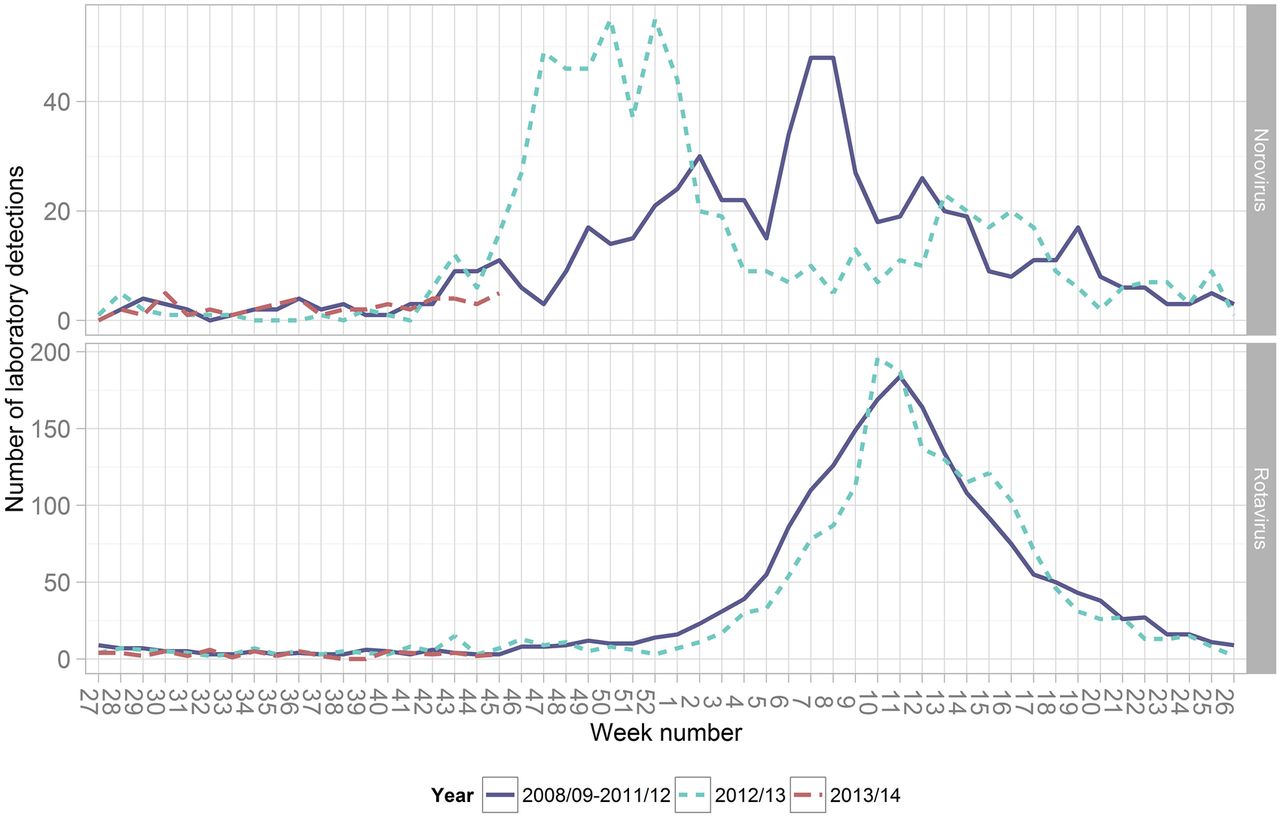
As many of the data sources included in this study do not include specific RVGE classification, we will be using AGE as an outcome measure for most data sets. Laboratory detection data which are organism specific will allow us to adjust these measures based on the seasonal contribution of organisms other than rotavirus such as norovirus. For example, RVGE seasonality is fairly constant but that of norovirus tends to vary over the winter and spring months in the UK. These AGE indicators can therefore be adjusted for changes in norovirus seasonality (figure 3)35 to give a better proxy of the contribution of rotavirus to overall AGE causes and the relative impact of rotavirus vaccination.

{kind=link}
{kind=link}
{kind=link}
Laboratory detections of rotavirus and norovirus in the North West, England, 2009/10–2013–14. Laboratory reports are from LabBase2 system at Public Health England,35 showing variation in the norovirus season as compared to the rotavirus season.
Limitations
The gold standard for measurement of vaccine efficacy is the randomised controlled trial. However, this ecological study will investigate the impact of vaccination on population disease burden within a health system; therefore, an ecological study is appropriate. Conversely it is recognised that an ecological approach cannot show individual-level effects of vaccine and can only infer the impact of the vaccine at the population level without causation. Additionally, a key focus of this study will be to quantify variation in the outcomes measured according to vaccine uptake levels and socioeconomic deprivation. Confounding may be an issue since cases living in areas with low vaccine uptake or high socioeconomic deprivation may also have other characteristics that will affect the risk of RVGE or AGE.
For measures of AGE activity in community settings (eg, GP and Walk-in Centre), we will use syndromic indicators that are non-specific to rotavirus, for example, diarrhoea, vomiting. An inherent issue is that the ability to detect effect on these is likely to be limited to large effects rather than small variations.
A further limitation of the study is that investigators will not collect data directly as all data are secondary, with consequent risk of bias. There is potential for clinical coding to lead to misclassification of disease, and this misclassification may vary by different data sources. We will describe these biases through quality control and subsequently adjust for them at the analysis stage. The use of multiple data sets for outcome indicators limits these issues by improving robustness.
It is likely that there have been changes in data collection methods over the study period, for example, changes to the assay used for rotavirus laboratory testing, leading to testing bias. One way to adjust for this in the analysis is to pool data over a number of years to smooth fluctuations caused by changes in testing methods. The investigators will identify changes through contact with rotavirus testing laboratories and NHS Trusts, so that changes may be described and where possible assist appropriate analytical adjustments. It is also feasible that the introduction of vaccination may also trigger changes in clinician requests for rotavirus and other AGE diagnostic testing, particularly in the vaccination age group. Any possible testing bias will be assessed at the lead NHS Trust via comparisons with prevaccine testing probabilities.
The study currently will not include any economic component. However, previous studies have reported the likely cost-effectiveness of rotavirus vaccination for the population under 5 years of age.36 This study will provide the results and data necessary for economic evaluation based on the direct and indirect impact of rotavirus vaccination.
Acknowledgments
The authors gratefully acknowledge the effort and assistance provided by all the research and development staff, laboratory technicians, data entry staff and support staff at the collaborating sites.
References
Footnotes
-
Contributors DH participated in the design of the study, will oversee the study co-ordination, data collection and analysis, and wrote the manuscript. RV conceived of the study and participated in its design; and will contribute to study co-ordination and analysis. MI-G conceived of the study and participated in its design; and will contribute to study co-ordination. NF conceived of the study and participated in its design; and will oversee study co-ordination and contribute to analyses. NC conceived of the study, participated in its design and will contribute to study co-ordination. All authors were involved in revising the manuscript and read and approved the final manuscript.
-
Funding This study is in part supported (approximately 35% of total cost) by GlaxoSmithKline Biologicals SA. GlaxoSmithKline Biologicals SA was provided the opportunity to review a preliminary version of this manuscript for factual accuracy but the authors are solely responsible for final content and interpretation. The authors received no financial support or other form of compensation related to the development of the manuscript.
-
Competing interests The Rotarix vaccine used in the UK national immunisation programme evaluated by this study is developed and licensed by GlaxoSmithKline Biologicals. NC is in receipt of research grant support from GSK Biologicals (to University of Liverpool) and has received honoraria for participation in GSK Rotavirus Vaccine Advisory Board Meetings.
-
Ethics approval The study has been approved by NHS Research Ethics Committee, South Central-Berkshire REC Reference: 14/SC/1140.
-
Provenance and peer review The protocol was peer reviewed externally and internally prior to sponsor and ethical approval.
-
Data sharing statement Data sharing agreement will be obtained between PHE, participating NHS Trusts and the University of Liverpool. Research governance approval will be sought form all participating NHS Trusts and Clinical Commissioning Groups.