Article Text

Abstract
Introduction The transfer of patient care between the intensive care unit (ICU) and the hospital ward is associated with increased risk of medical error and adverse events. This study will describe patient transfer from ICU to hospital ward by documenting (1) patient, family and provider experiences related to ICU transfer, (2) communication between stakeholders involved in ICU transfer, (3) adverse events that follow ICU transfer and (4) opportunities to improve ICU to hospital ward transfer.
Methods This is a mixed methods prospective observational study of ICU to hospital ward transfer practices in 10 ICUs across Canada. We will recruit 50 patients at each site (n=500) who are transferred from ICU to hospital ward, and distribute surveys to enrolled patients, family members, and healthcare providers (ICU and ward physicians and nurses) after patient transfer. A random sample of 6 consenting study participants (patients, family members, healthcare providers) from each study site (n=60) will be offered an opportunity to participate in interviews to further describe stakeholders’ experience with ICU to hospital ward transfer. We will abstract information from patient health records to identify clinical data and use of transfer tools, and identify adverse events that are related to the transfer.
Ethics and Dissemination Research ethics board approval has been obtained at the coordinating study centre (UofC REB13-0021) and 5 study sites (UofA Pro00050646; UBC-PHC H14-01667; Sunnybrook 336-2014; QCH 14-07; Sherbrooke 14-172). Dissemination of the findings will provide a comprehensive description of transfer from ICU to hospital ward in Canada including the uptake of validated or local transfer tools, a conceptual framework of the experiences and needs of stakeholders in the ICU transfer process, a summary of adverse events experienced by patients after transfer from ICU to hospital ward, and opportunities to guide quality improvement efforts.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Data will be collected from 10 sites (7 cities, 4 provinces) across Canada.
Data will be collected from a variety of stakeholders (patients, family members, physicians and nurses) to give a broad perspective on the transfer process.
Data collection instruments are both qualitative and quantitative.
Data collected will inform the development of a tool that will improve the ICU to hospital ward transfer process.
Results will not be generalisable to all hospitals in Canada.
Introduction
The transfer between intensive care unit (ICU) and hospital ward is a vulnerable period in healthcare delivery. Risk for adverse events may increase as a result of the vulnerability of this patient population requiring complex care,1–3 the reduction in monitoring capacity outside the ICU,4 ,5 the necessary participation of multiple professionals with different cultural norms and practices,5–9 frequent communication failures that are associated with medical errors,5 ,6 ,10–12 longer hospital stays,13 increased costs,14 stress,2 ,6 ,15 ,16 and poor quality of care.5 ,17
Communication breakdown
Communication breakdown during patient transfer is common9 ,12 ,18–22 and leads to: decisions based on inaccurate or incomplete information;19 patients who are exposed to unnecessary tests and treatments;13 ,18 ,23 medication errors;6 ,18 ,24–27 and patients/family members who are confused and disappointed by what they perceive as conflicting decision-making and lower quality of care.5 ,6 ,17 Poor communication causes misunderstandings about care plans,28–30 patient conditions,24 ,31 code status,24 ,32 ,33 and test results.13 ,24 ,33 ,34 Communication problems are implicated in up to 70% of adverse events or near misses in US hospitals.8
Verbal face-to-face communication between ICU and ward providers is an effective way to improve patient safety during transfers from ICU to hospital ward.21 ,35 Verbal face-to-face communication allows for the transmission of judgements about how care is perceived to be progressing,8 and creates opportunities for healthcare providers to highlight subtle yet important information36–38 which is often not formally documented.8 Unfortunately, verbal face-to-face communication is rare and often incomplete.5 ,39 ,40 One reason may be that there is often no consensus about what should be communicated, who should communicate, and how communication should occur during patient transfer.6 There are also differences between what is considered essential knowledge that requires attention at the time of transfer.6 ,8 ,9 ,40 ,41
Patients and family members indicate that lack of information before ICU to hospital ward transfer causes them to feel anxious about the unknown, and confused and dissatisfied with their care.5 ,6 ,15 Providing information to patients and families about the transfer improves patient safety, increases understanding of differences in clinical management between the ICU and hospital ward, and improves quality of care.6 ,42
Multiprofessional transfer
The multiprofessional nature of ICU care implies that transfer from ICU to hospital ward requires handing over of relevant information among many professionals (eg, physicians, nurses, respiratory therapists, clinical nutritionists, physiotherapists, occupational therapists, social workers, psychologists and pharmacists).2 ,35 These complementary areas often operate under different patient management models where the responsibilities of professionals may vary. For example, assistance to help patients mobilise, an important step of rehabilitation, may be under the responsibility of nurses in the ICU and then shift to physiotherapists once a patient is transferred to the ward. In addition, there may be perceived and real imbalances between healthcare professionals’ roles and responsibilities that limits involvement in the transfer process,8 ,17 ,28 ,35 differences in scientific or professional jargon used,8 ,43 and variation in the content44 and structure45 ,46 of health records between ICU and hospital ward. To date, most efforts to measure and improve transfer of care have focused on transfers within professions despite the multiprofessional nature of care.
Drop in intensity of care
ICUs are specialised units where multiprofessional teams of healthcare providers collaborate to provide continuous patient care.14 ,17 On average, ICU nurses look after one or two patients per shift and ICU physicians are responsible for 8–10 patients at any time.4 By contrast, hospital ward nurses will care for 4–8 patients per shift, while hospital ward physicians might be responsible for as many as 65 patients at some points in the day.47 For patients, the transfer to the hospital ward may be experienced as abandonment42 because healthcare providers have less time and resources to focus on patients.48 ,49 Additionally, family members report feeling confused and stressed over the reduced level of care after transfer from ICU,6 and an increased responsibility to provide bedside care.42 Ward nurses report feeling stressed when receiving a patient from the ICU if they feel inadequately prepared or time constrained to care for patients who have high needs.46 ,50 Reduced intensity of care after transfer from ICU is associated with increased adverse events.3 ,4
Resource limitations
ICU patients represent the smallest hospital population, yet they absorb the largest percentage of hospital expenditure.2 ,14 Limited resources are an incentive for efficient discharge out of the ICU. Furthermore, bed availability for patients outside of the ICU may put pressure on discharging less sick patients. Hospitals must balance heightened efficiency with the risks posed by discharging patients too early.2 ,14 ,39 Premature patient transfer out of ICU increases morbidity and mortality,6 ,10 raises healthcare costs,14 and reduces patient satisfaction.2
Evidence on patient transfer highlights the relevance of standardised handover protocols to avoid communication failure,5 ,51 reduce adverse events,30 reduce cost, and improve patient safety.8 ,20 ,46 Because most ICU patients are transferred to a hospital ward, the ICU to hospital ward transfer is crucial for creating safe and seamless transfers of care for these vulnerable patients.8 ,15 ,41
We propose a mixed methods multicentre observational study to document the experiences of relevant stakeholders with ICU to hospital ward transfer. We will collect information that describes stakeholders’ transfer experiences, communication during transfer, and adverse events that result from the transfer. Collected data will identify opportunities to improve the transfer process and aid in the development of an ICU transfer toolkit.
Objectives
Overarching objective
To describe patient transfer from ICU to hospital ward.
Specific objectives
Describe patient, family member and healthcare provider experiences and needs related to transfer from ICU to hospital ward.
Describe current communication content and structure during transfer from ICU to hospital ward.
Describe adverse events experienced by patients after transfer from ICU to hospital ward.
Discover opportunities to improve transfer from ICU to hospital ward.
Methods/design
Study design
We propose to conduct a mixed methods prospective observational study of transfer practices in 10 ICUs located in seven cities (four different provinces) in Canada (box 1). We will coordinate data sources (patients, family members, healthcare providers) and methods (surveys, interviews, health record review) to provide a comprehensive description of ICU transfer practices across Canada, and create a conceptual framework of stakeholder transfer needs. Data from this study will inform a future phase of the study that will develop an evidence-informed ICU transfer toolkit.
Study sites for data collection
St Paul's Hospital, Vancouver, British Columbia
University of Alberta Hospital, Edmonton, Alberta
Foothills Hospital, Calgary, Alberta
Rockyview General Hospital, Calgary, Alberta
Peter Lougheed Centre, Calgary, Alberta
South Calgary Health Campus, Calgary, Alberta
Queensway Carleton Hospital, Ottawa Ontario
Sunnybrook Health Sciences Centre, Toronto, Ontario
CHU de Quebec (Hôpital de l'Enfant-Jésus), Quebec City, Quebec
Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, Quebec
Study population
We will target a population of patients who are identified as ready to transfer from the ICU to a hospital ward located in the same hospital. We will also target a corresponding family member and the healthcare providers. A family member will be defined as the most significant caregiver who visited the patient at least once in the ICU within the 3 days before the transfer, and at least once within the 3 days after the transfer. Targeted healthcare providers are the clinicians most involved with enrolled patients’ transfer from the ICU to hospital ward. We will identify ICU nurses who care for enrolled patients on the day of transfer, and ICU physicians (attending or resident) who are involved in preparing the patients’ summary documents immediately before the transfer. On the ward, we will identify ward nurses who conduct the first head-to-toe examination of the patient, and ward physicians (attending or resident) who assume responsibility for the patients’ care directly after the transfer from the ICU.
Criteria for patients enrolled in this study are (1) of age to give consent or older, (2) admitted to a general (medical-surgical) ICU for at least 24 h, (3) identified as ready to transfer to a hospital ward within the same facility, (4) able to provide consent or has a surrogate willing to provide consent and (5) patient and/or surrogate is able to speak either English or French.
Patients will be excluded from the study if they are admitted to a subspecialised ICU (eg, cardiovascular ICU, neuroscience ICU), or transferred to a location other than a hospital ward within the same facility (eg, other ICU, home, long-term care facility, etc).
Consent
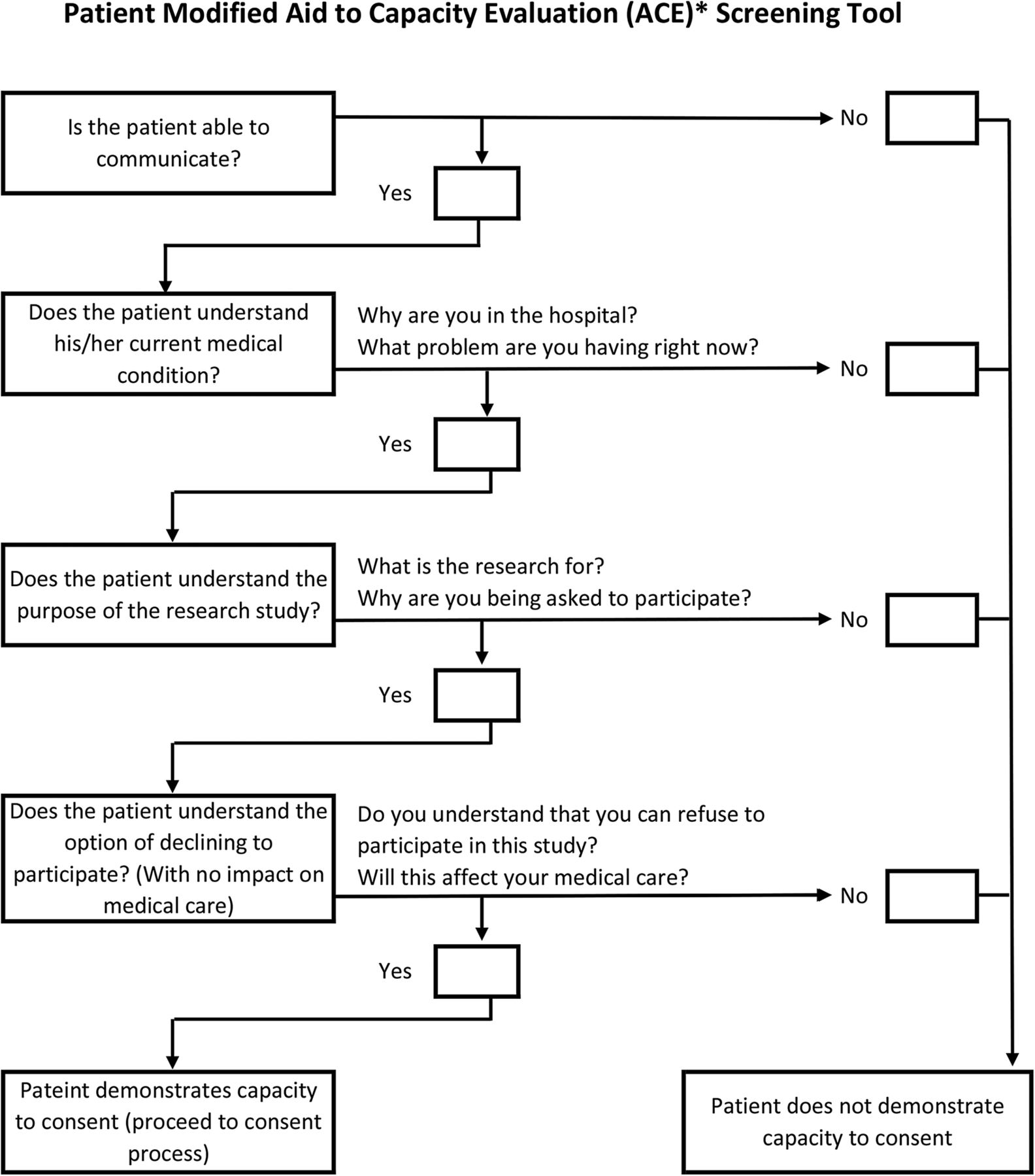
The patients’ capacity to provide informed consent will be determined by a modified Aid to Capacity to Evaluation tool52 (figure 1). If the patient does not demonstrate capacity to consent, we will attempt to identify a suitable surrogate to provide informed consent. Healthcare provider's consent will be gathered from implied or written consent depending on the study location. Implied consent will be explained on the cover sheet of healthcare provider surveys.

{kind=link}
ACE Capacity to Consent Screening Tool.
Sampling
We will enrol 50 consecutive patients identified as ready for transfer from the ICU to a hospital ward at each study site that satisfies the inclusion criteria and consent to participate (n=500). For each enrolled patient we will attempt to also collect survey data from one family member and four healthcare providers (ICU physician, ICU nurse, ward physician, ward nurse) for a maximum of 3000 survey participants. At each study site we will conduct six telephone interviews to further explore patient transfer from ICU to hospital ward. Table 1 summarises the anticipated sample size for this study.
Anticipated sample for prospective cohort study
Data collection
Surveys
Patient, family, surrogate and healthcare provider surveys
Patients (or surrogates), family members, ICU physicians, ICU nurses, ward physicians and ward nurses will be approached to complete surveys (paper or electronic, depending on study site and participant preference) that will ask about communication, level of involvement, workload, use of transfer tools, and adverse events related to the transfer from ICU to hospital ward. A research coordinator will identify relevant participants through direct communication with the patient, surrogate, bedside nurses and unit clerks.
Surveys will be distributed up to 3 days after patient transfer from the ICU. Altogether, we have developed seven survey instruments. These are:
Patient survey (see online supplementary appendix A)
Family/surrogate survey (see online supplementary appendices B and C)
ICU physician survey (see online supplementary appendix D)
ICU nurse survey (see online supplementary appendix E)
Ward physician survey (see online supplementary appendix F)
Ward nurse survey (see online supplementary appendix G)
Hospital survey (see online supplementary appendix H).
Patient, surrogate, family and healthcare provider survey instruments were developed based on data obtained from a scoping review carried out by our team.53 Revision of data collection tools took place in four rounds that included initial editing by our team, clinical sensibility testing based on interviews with stakeholders (patients, family members and healthcare providers), incorporation of additional feedback from our multidisciplinary national advisory committee, and final editing by our team to ensure consistency and logical flow. All tools were subsequently translated into French by a skilled translator and then checked for accuracy by a second skilled translator and healthcare professional.
Hospital survey
A hospital survey will be administered to each study ICU's manager (n=10) and will collect information about the hospital (eg, number of acute care beds) and ICU structure (eg, type and size of ICU), policies (eg, transfer programme), and procedures (eg, transfer criteria) related to patient transfer from ICU.
Interviews
The qualitative component of this project (interviews) will be drawn from a random sample (using a random number generator) of consenting participants from each study site who agree to participate in semistructured telephone interviews. These participants (one patient, one family member, one ward physician, one ward nurse, one ICU physician, and one ICU nurse from each study site) will provide an in-depth perspective of stakeholders’ experience with transfer from ICU to hospital ward. We plan to sample six participants per study site, but if necessary, will continue to sample participants until we reach data saturation. We have developed two draft interview guides (see online appendices I and J). Additional domains of inquiry may be added to our interview guides based on results gathered from the stakeholder surveys.
Patient health record review
Case report form
From patient health records, we will abstract (1) demographic information, (2) clinical data (ie, patient characteristics, illness severity scores (SOFA54 APACHE II55), (3) clinical diagnosis, (4) the use of local or standardised ICU transfer tools, (5) comorbidities, (6) procedures done in the ICU, (7) time spent in ICU and on the ward, (8) ICU readmission and (9) final transfer location. These will be collected on a Case Report Form (see online supplementary appendix K).
Textual analysis of health records
We will obtain a copy of all clinical notes recorded in each patient's health record during the final 2 days of their stay in the ICU, the day of transfer from the ICU, and the first 7 days of their stay on the ward that accepted care from the ICU for a total of 10 calendar-days. Patient data that are photocopied will be deidentified and assigned a unique identifier. We will focus on clinical notes and ICU transfer tools documented during this period. We define clinical notes as health record entries that include an interpretation of clinical data or a patient management plan. We expect to identify different types of healthcare provider clinical notes from multiple professions and specialties including interdisciplinary progress notes, consultation notes, transfer notes and admission notes. A detailed list of all local and standardised transfer tools located in patient health records will be created and used to inform a future phase of the study that will evaluate and develop an evidence-informed transfer toolkit.
Adverse events
Two clinical investigators, practising physicians with expertise in acute care hospital-based medicine, will independently review each clinical note to identify adverse events using standard methods adapted from the Harvard Medical Practice Study.56 For each adverse event identified they will independently grade the severity of any injury (on a 6-point scale ranging from single day of symptoms to death) and rate their confidence in the preventability of the adverse event (on a 6-point scale ranging from no evidence to virtual certain evidence of preventability).57 A third reviewer will resolve discrepancies.
Analytical plan
Data analysis for this study will be descriptive using a combination of qualitative and quantitative methods to triangulate findings.58
Surveys
We will present global data to describe opportunities to improve ICU transfer (eg, goals of care reconciliation). We will present detailed tabulations of responses by participant (patient vs family member vs healthcare provider), patient (medical vs surgical) and hospital (university-affiliated vs community) characteristics. The significance of observed differences will be evaluated using χ2 tests.
Interviews
All interviews will be audio taped, transcribed verbatim, assigned a unique identifier and imported into NVivo V.10, a computer programme for qualitative data management. Two investigators will independently read each transcript and code the raw data, line by line, using a process of open, axial and selective coding.59 ,60 The investigators will sequentially collapse the codes to form abstract and then advanced concepts until core variables emerge along with supporting categories that explain stakeholder experiences with ICU transfer.61 Axial coding will examine the context, intervening conditions and consequences of core variables (eg, what contextual factors influence identification of exemplary cases of high-quality care during ICU transfer.62 Selective coding is the final stage of analysis in which a story of ICU transfers will be built. The result will be a framework describing ICU transfer, stakeholder needs and opportunities for improvement (facilitators and barriers to high-quality ICU transfer). Credibility of the core variables will be determined by the frequency with which they are recorded within transcripts. Written memos will be used to provide a record of the analytic process.59 ,60 All interview participants will be provided with a copy of the study report for review and comment as a form of member-checking.63
Patient health record review
Patient characteristics (eg, severity of illness), processes of care (eg, ICU transfer tools) and outcomes of care (eg, readmission to ICU) abstracted from the medical record (case report form), will be summarised using descriptive statistics (ie, means, medians, proportions). We will present detailed tabulations by patient (medical vs surgical), and hospital (university-affiliated vs community) characteristics.
To provide a description of written communication, qualitative textual analysis64–67 will be done to describe and compare the structure of written communication within participants’ medical charts before, during and after ICU transfer. Analysis will involve coding each clinical note for order, organisation and legibility. Patient characteristics, including medical or surgical classification and experiences of adverse events will be given particular consideration. The coding of raw data will then be used to construct a protocol to analyse textual documentation of clinical notes written in the ICU and hospital wards across all sites, with the goal of creating a shared communication structure.
We will develop a comprehensive list of adverse events and present global data to describe the proportion of ICU transfers that are complicated by an adverse event along with binomial 95% CIs.
Relevance of findings
Transfers of patient care are highly vulnerable moments that require communication of crucial information between healthcare providers from different locations,12 and sometimes a shift of care responsibilities directly to patients and family members.68 To be effective, seamless and safe, transfers of care must be supported by focused communication, dedicated and informed healthcare providers, and engaged patients and families.6
Next steps
This study will (1) provide a comprehensive description of the process of transfer from ICU to hospital ward in Canada. This will include the application of transfer tools, developing a conceptual framework of the experiences and needs of stakeholders who are involved in transfer from ICU to hospital ward, providing a summary of adverse events experienced by patients after transfer from ICU to hospital ward, and identifying opportunities for improvement. Key deliverables developed from this study will be made available in English and French.
Data collected from this study will inform the next phase of our programme of work, which is to develop an evidence-informed ICU toolkit for ICU to hospital ward transfer. We will amalgamate data from this study with an analysis of existing tools used to facilitate ICU to hospital ward transfers.53 ,69
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online Appendix A
- Data supplement 2 - Online Appendix B
- Data supplement 3 - Online Appendix C
- Data supplement 4 - Online Appendix D
- Data supplement 5 - Online Appendix E
- Data supplement 6 - Online Appendix F
- Data supplement 7 - Online Appendix G
- Data supplement 8 - Online Appendix H
- Data supplement 9 - Online Appendix I
- Data supplement 10 - Online Appendix J
- Data supplement 11 - Online Appendix K
Footnotes
Contributors All authors contributed to the conception (HTS) or design (DB, SB, PD, AF, RF, FL, AT, MP, HTS) of the work; and drafting (DB, HTS) or revising (DB, SB, PD, AF, RF, FL, AT, MP, HTS) the work for important intellectual content; and provide final approval of the manuscript and agree to be accountable for the accuracy and integrity of the work.
Funding Technology Evaluation in the Elderly Network (TVN) (CORE 2013-12A).
Competing interests None declared.
Ethics approval University of Calgary Conjoint Health Research Ethics Board (UofC REB13-0021).
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.
Data sharing statement No additional data are available.