Article Text

Abstract
Objective To investigate how functional, social and personal factors are associated with self-perceived level of disability in the chronic phase of stroke in a Latvian stroke population. The consequences of stroke can vary greatly and often leads to long-term disability that, according to the WHO definitions, depends on the interaction between the person and his/her context.
Design Cross-sectional study with retrospective data gathering.
Setting Community-dwelling persons who received specialised in-patient rehabilitation after stroke in Latvia.
Participants Of 600 persons after stroke who were identified through hospital register and selected for the study, 255 were included in the analysis.
Primary and secondary outcome measures The medical information and discharge data of the Functional Independence Measure (FIM) was extracted from medical records. Participants filled out a questionnaire on sociodemographic information and the WHO Disability Assessment Schedule 2.0 (WHODAS 2.0), either in Latvian or Russian, depending on their wish when contacted for their oral agreement to participate. Stepwise multiple regression analysis was conducted to find a model that best explains the variance in WHODAS 2.0 scores.
Results The models explained 23–43.5% of variance in outcomes. The best explained WHODAS 2.0 domains were ‘mobility’ and ‘self-care’. The significant factors were level of independence in ‘self-care’, ‘locomotion’ and ‘communication’ according to FIM, as well as working status, time since rehabilitation, age, gender, living alone or in family and preferred language.
Conclusions Functional, social and personal factors are of similar importance when explaining self-perceived disability in the chronic phase of stroke. Some, but not all, of the factors are modifiable by the healthcare system. Therefore, a complex approach and involvement of medical, social and political systems is needed.
- Outcome
- Functional factors
- Social factors
- Personal factors
- Perceived disability
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
In this study, a wide range of factors from functional, social and personal perspectives are used for explanation of the self-perceived disability in the chronic phase of stroke using regression analysis.
The role of the healthcare system (including rehabilitation medicine) as well as social aspects of functioning has been evaluated.
Participants of this study could choose between two languages (Latvian and Russian) to fulfil the questionnaire; therefore, a realistic picture of the poststroke population living in Latvia could be captured; however, a bias of results cannot be excluded.
The level of independence at discharge was assessed by multiple clinicians.
Introduction
Disability is a unique, individual experience that is, or becomes, part of the human condition. In general, it is perceived as reduced functioning in any aspect of a person and his/her life.1 According to the suggested model from the WHO, these aspects can be divided into ‘body functions and structures’ and ‘activity and participation’.2 However, functioning depends on the underlying health problem/s, as well as on the external (environmental factors) and internal (personal factors) background of the person.2 Disability is therefore composed of an interaction between two dimensions—functional limitation due to the underlying health condition and contextual factors.1 Another aspect is that disability varies over time, which makes it even more complex to assess and reduce with interventions.3
Currently stroke is one of the most prominent non-communicable health problems,4 especially in European countries,5 ,6 due to the level of mortality, as well as the remaining impairments in the survivors after stroke.6–8 A wide variety of motor, sensory and cognitive impairments9 can influence the capacity and performance of everyday life activities.10 Moreover, stroke often results in reduced independence.11
Individual limitations and restrictions from a stroke depend on the context, such as access to support and the environment (both individual and social), as well as on these persons' subjective views and roles in society.1 ,2 Increased needs for health and social care, as well as loss of working ability for those of working age, are only a few of the many essential aspects of the burden of stroke.1 ,12
The overall aim of rehabilitation is to maximally reduce these consequences and thereby reduce the disability, within the framework of a biopsychosocial approach.13 Both time and the quality of rehabilitation are reported as essential in reducing disability.14–16 Acute and postacute rehabilitation mainly focus on impairment reduction and improvement of independence in the activities of daily living.14 ,17 Later, when the person returns to his/her usual environment, the focus may need to shift from a medical to a social one.18 Disability due to stroke causes complex and long-term emotional and financial burdens for the person, their family and the community.5 ,6 ,19 ,20 Therefore, it is important to also acknowledge and assess disability from a societal perspective. This will lead to identifying needs, matching treatments and interventions, measuring outcomes and effectiveness, setting priorities and appropriately allocating resources.21
As in most European countries, stroke along with other cardiovascular diseases is one of the leading causes of mortality in Latvia.22 Moreover, it has been estimated that, although decreasing, mortality after stroke in Latvia remains one of the highest in the European Union.23 ,24 Stroke is also the main reason for the officially approved disability status in Latvia.25 However, there is little information available on the outcomes for persons after stroke in Latvia. In 2003, ∼10 years after the restoration of independence in Latvia, McKevitt et al26 described experiences of persons after stroke in Riga, emphasising the cultural and social aspects as the determinants of disability experiences.
The aim of the study was to investigate how functional, social and personal factors explain the self-perceived level of disability in the chronic phase of stroke in persons living in Latvia.
Methods and materials
Study design
Cross-sectional study with retrospective data gathering.
Data collection and study population
A sample of convenience was used. Persons who had received specialised in-patient rehabilitation in the postacute phase of stroke at the Department of Neurorehabilitation in National Rehabilitation Centre (NRC) ‘Vaivari’, Latvia, from 1 January 2011 to 31 December 2013 were identified through the computerised hospital register. Prespecified data were gathered from the charts and entered into a file. This included the Functional Independence Measure (FIM) at discharge, diagnosis and date of stroke. Those living in the community were asked to participate in the study by telephone. After consent, the correspondence address was obtained and a set of questions that included current sociodemographic information, as well as WHO Disability Assessment Schedule 2.0 (WHODAS 2.0),21 were sent by mail or email. During the phone conversation, the preferred responding language (Latvian or Russian) was asked for. This was done because 37% of population in Latvia use Russian as their primary language.27 If the person could not fill out the questionnaire themselves, it could be performed by their next of kin.
Inclusion criteria were: first-time diagnosis of stroke (International Classification of Diseases (ICD)-10 codes I60-I6728) clinically determined by the attending physician in acute care according to the WHO criteria29 and confirmed by CT; age of at least 18 years, and at least 9 months poststroke.
Out of the 600 persons who were selected for the study, 49 refused to participate, 50 were deceased and 119 were not reachable. Out of the 382 persons who agreed to participate in the study, 255 completed the questionnaire and sent it back. The flow chart of the study population is shown in figure 1.

Study flow chart.
Outcome variables
Dependent variables
The WHODAS 2.0 36-item self-assessment questionnaire was used for evaluation of the disability level. It is directly linked to the ‘activity and participation’ component of International Classification of Functioning, Disability and Health and has shown good psychometric properties (validity, reliability, sensitivity to changes and item–response characteristics).21 WHODAS 2.0 consists of 36 items in six domains. Each item is scored on a five-level scale (1=‘no difficulties', 5=‘extreme difficulties or cannot do’). Recoded scores were summed and converted into a metric ranging from 0 (no disability) to 100 (full disability)21 for the following outcomes:
Domain 1: ‘cognition’ (understanding and communicating)—six items;
Domain 2: ‘mobility’ (moving and getting around)—five items;
Domain 3: ‘self-care’ (attending to one's hygiene, dressing, eating and staying alone)—four items;
Domain 4: ‘getting along’ (interacting with other people)—five items;
Domain 5, part 1: ‘household activities’ (domestic responsibilities)—four items;
Domain 5, part 2: ‘work or school activities’—four items;
Domain 6: ‘participation’ (joining in community activities, participating in society)—eight items;
Total WHODAS 2.0 score.
For the WHODAS 2.0 data set, the simple approach to missing data and the complex scoring method were used (the scores of each item were recoded according to the suggested algorithm).21 The simple approach to the missing data means that if responses in one or two items were missing, the mean raw score of the corresponding domain replaced the missing response. In a case where more than two responses were missing in the data set, the response remained missing and the mean score was not used. Complex scoring is based on the ‘item–response theory’ and each item's level of difficulty is taken into account and weighted accordingly.21
Independent variables
FIM was used to define the levels of independence at discharge from rehabilitation.30 It is used as a routine clinical assessment tool in NRC ‘Vaivari’. The evaluation is conducted by members of the rehabilitation team. FIM consists of 18 items, each scored on a seven-point scale (1–7). Grades 7 and 6 are used to describe complete and modified independence, respectively. Grades 5–1 are used to describe different levels of dependence, which are supervision, minimal assistance, moderate assistance, maximal assistance and total assistance, respectively. For this study, the data from FIM at discharge from rehabilitation were used and the items were grouped under six domains—‘self-care’, ‘sphincter’, ‘transfer’, ‘locomotion’, ‘communication’, ‘social cognition’. The overall results for each domain were presented in a trichotomised way. The domains were coded as ‘1’ or ‘totally dependent’ if any of the items in the domain was scored as ‘1’ or ‘2’, ‘2’ or ‘partially dependent’ if any of items in the domain was scored as ‘3’, ‘4’ or ‘5’, but none as ‘1’ or ‘2’ and 3, or ‘independent’ if all items were scored as ‘6’ and ‘7’.
Further independent variables that were included in the questionnaire were status of employment (working or not after stroke), time after discharge from rehabilitation (months). ‘Working’ was defined as persons who had paid or unpaid work, were self-employed, studied or were performing household duties.
Personal factors, such as age, gender, preferred language (Latvian or Russian), education, place of living (city or countryside) and living situation (alone or in a family), were used as secondary explanatory variables. Time (weeks) from stroke onset until start of rehabilitation, length of rehabilitation (days) and type of diagnosis according to ICD-10 were seen as potential cofounding variables.
Data analysis
Demographic and clinical characteristics of the population were described using frequencies, means and medians. Stepwise multiple linear regression analysis31 was used to predict the summary scores for each of the seven domains and the total score of WHODAS 2.0. The initial model for regression analysis is illustrated in figure 2.
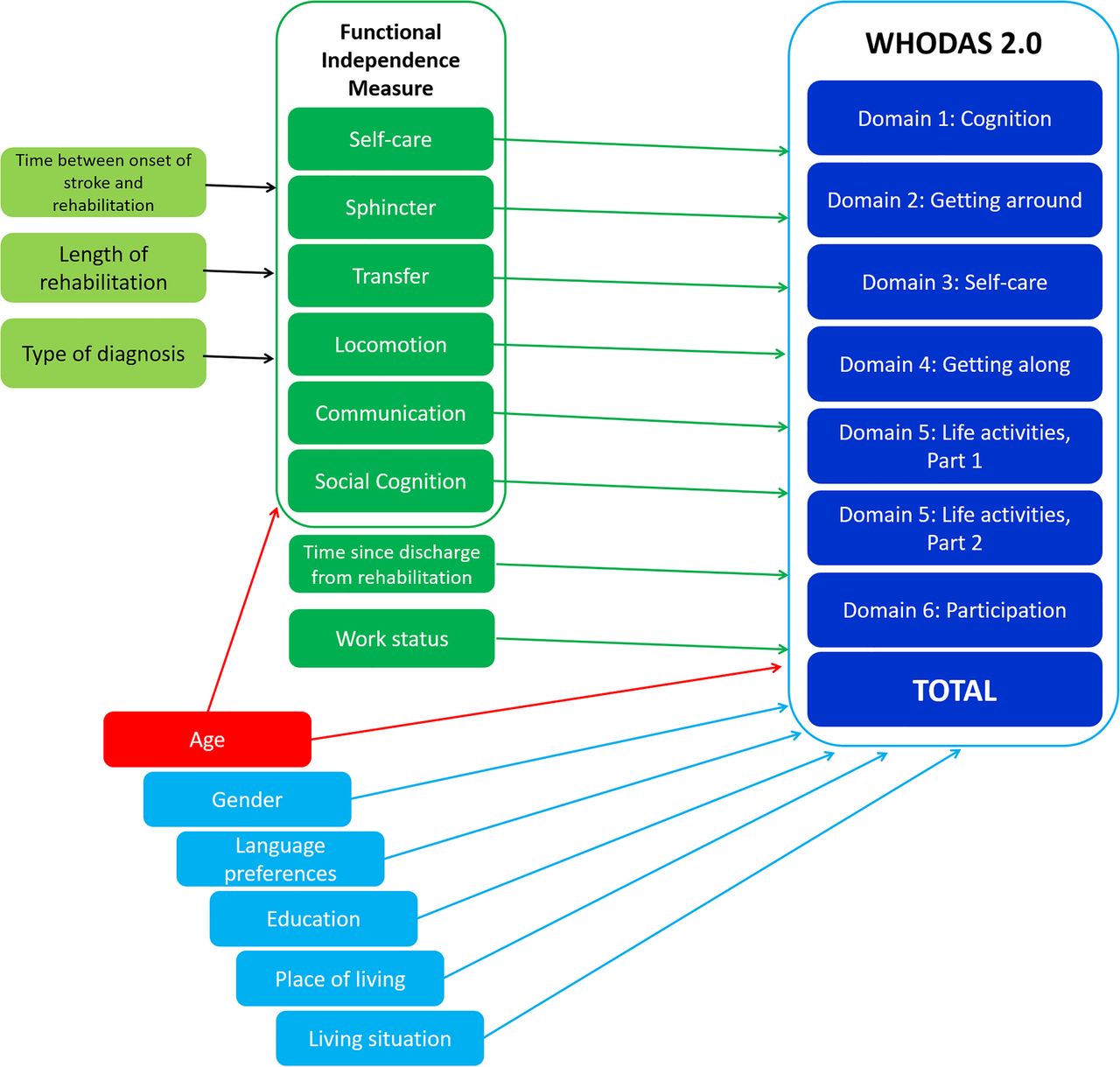
Initial model for the analysis. WHODAS 2.0, WHO Disability Assessment Schedule 2.0.
The steps for the multiple regression model building were as follows:
Step 1: univariate regression analyses were done to evaluate the association between each of the 16 predictor variables and the outcome.
Step 2: multiple regression analyses with all predictor variables with p<0.25 at step 1 were included in the model.
Step 3: those variables which showed p>0.25 were excluded from the model and multiple regression analysis with variables, significant in step 2, was performed.
Step 4: the variables rejected at step 1 were reinserted one by one in the model with the remaining variables from step 3. If the variable turned out to be significant (p<0.05), it was left in the model.
The best model was selected by comparing models with an F test. If the two models were significantly different (p>0.05), the model with higher R2 values was chosen. If the models were not significantly different, the model with the least amount of explanatory variables was chosen.
For each of the final models, analyses were conducted to ensure no violation of the assumptions of normality, linearity, multicollinearity and homoscedasticity.
Each of the significant factors in the final model in turn was excluded from the model and changes of R2 were reported, to illustrate the factors' unique contributions to the model.
Work as an explanatory factor was excluded from the analysis of domain 5.2 since this domain evaluates the ability to work and was not fulfilled by those who were unemployed.
Statistical analyses were made with SPSS (V.21.0).
Results
Descriptive statistics
The characteristics of the study population are shown in table 1. There were no significant differences in the basic characteristics between the selected and final study populations. Out of the 50 persons who were working, 39 were of working age (18–60 years) and 11 were above the official age of retirement. The group consisted of 52% males and the mean age was 63 (SD 13) years (range 22–92). The median time after discharge from rehabilitation was 1 year and 9 months. Most of them were independent at the time of discharge from rehabilitation (figure 3). However, the median level of self-perceived disability, evaluated by WHODAS 2.0, was 52% (figure 4).
Characteristics of the study population

Shifts between levels of dependence at discharge from rehabilitation centre by FIM domains. FIM, Functional Independence Measure.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box plot on WHODAS 2.0 results by domain. WHODAS 2.0, WHO Disability Assessment Schedule 2.0.
Multiple regression analysis
The models explained 23–43.5% of the variance in the outcomes. The explained variance of the total WHODAS 2.0 score was 40.8%. The domains of ‘mobility’ and ‘self-care’ were explained best, but the most poorly explained domain was ‘cognition’. For detailed results, see table 2.
The results of the final models of multiple regression analysis by WHODAS 2.0 domains and total score
The dependence level of ‘self-care’ at discharge from rehabilitation was included and significant in the final explanatory model in five out of seven analysed domains, as well as in the total WHODAS 2.0 score. Results indicated that being dependent at discharge led to a higher level of perceived disability. ‘Locomotion’ was significantly related to the ‘mobility, ‘self-care’, ‘life activities: work or school’ and ‘participation’ domains. Similarly, persons recognised by rehabilitation professionals as independent in ‘communication’ at discharge perceived fewer problems in the domains of ‘cognition’, ‘getting along’ and the total WHODAS 2.0 scores.
Work status was the factor that showed association with all domains of WHODAS 2.0, with the exception of ‘getting along’. Results indicated that those who were working reported fewer problems in functioning when other variables in the final model were held constant.
A longer time since discharge was a significant factor in explaining worse ‘self-care’ and total scores of WHODAS 2.0. Age was also a significant factor regarding ‘mobility’ and ‘getting along’ and the total score of WHODAS 2.0, indicating that older persons experienced greater disability. Between other personal factors chosen for the analysis, gender, language and living situation were those of significance. Males reported higher levels of disability in the ‘cognition’ and ‘getting along’ domains. Those who preferred to fill out the questionnaire in Latvian reported fewer problems in functioning in the ‘getting along’, ‘life activities’ and ‘participation in society’ domains, as well as in total WHODAS 2.0 scores. Persons who lived alone experienced greater problems in ‘participation in society’ than those who lived in a family.
Discussion
This study suggests that self-perceived disability in the chronic phase of stroke cannot be explained solely by the level of independence in daily activities at discharge from rehabilitation. Other factors, such as social and personal ones, are of similar importance. Some of the factors are modifiable by the healthcare system through improved functioning. However, others, such as work situation and language preferences, are not possible to influence from the healthcare system but are a responsibility of society as a whole.
Functional, social and personal factors chosen for the analysis could explain up to almost half of the variance in a person's experience of life after stroke, depending on the analysed life aspect. These factors explained such domains as ‘mobility’ and ‘self-care’ rather well. Both these domains represent the issues of basic skills of physical functioning. The models explained considerably less well the perception of ‘understanding and communication’, as well as ‘interaction with other people’. These tasks require complicated multilevel skills that are more challenging to evaluate than physical functioning.
‘Participation in society’ was also rather poorly explained in comparison to other domains. Moreover, this domain, along with ‘household activities’, was reported as most problematic for the study population. That is of interest and importance because participation in society involves the usage of complex skills and navigation in everyday life.
The status in the present study population varied in full range—from no disability to extreme disability. The overall levels of disability were more severe when compared with those in a stroke population in Spain gathered at a similar period after the event.32 However, the population for this study was recruited using data from the rehabilitation centre that provides in-patient rehabilitation services versus the Spanish population which got its data from an epidemiological study. Therefore, the functional level in this study population could be reported as worse compared with that in the overall stroke population.
The overall goal of rehabilitation is to enable a person to live a meaningful life according to his/her wish, that is, in direct line with the concept of participation in society. However, the field of physical and rehabilitation medicine directly after stroke is oriented to the medical assessment and the functional aspects and focuses mainly on the improvement of independence in basic daily activities. These aspects, in turn, give a basis for better participation in society,33 ,34 and thereby on the quality of life. That gives support to the role of the rehabilitation process and the results of our study also support this. Either ‘self-care’ or ‘locomotion’, or both were important in explaining all outcomes. Being independent in locomotion is of importance not only for the ‘mobility’ domain of WHODAS 2.0, where there is direct theoretical relationship, but also for perception of problems in ‘participation in society’, as well as for ‘work activities' for those who are employed.
The level of independence or amount of care needed in six domains of daily activities was used as an explanatory factor in the study. When discharging patients from the specialised in-patient rehabilitation unit, rehabilitation professionals evaluate a person's ability to do simple tasks. This evaluation is used to establish whether rehab has been effective. However, more than one person is assessing patients that may lead to a bias in the results generated from this evaluation. However, the definition of FIM scoring is detailed and excellent inter-rater reliability has been reported for the instrument.35
Nevertheless, the ability to perform activities independently cannot give the whole picture of the disability experience.34 The results of this study highlight the importance of factors that are beyond the scope of dependence/independence aspects and thus beyond the field of rehabilitation medicine.
In the data analysis, work was the most common important factor that explains the outcome for persons after stroke. One could argue that returning to work depends on the stroke outcome. However, our results showed that employment had the highest unique contribution in certain domains, even when controlling for other important factors. Returning to work could lead to more positive health outcomes and quality of life,36 and most probably it does not depend on the work load (part-time or full-time employment).37 The ability to return to work after experiencing a disabling condition is in the interests of politicians and decision-makers for its contribution to the economy. Moreover, work is considered to be among the most important meaningful activities of the lives of many people.38 It is of great importance in Latvian society and not only for those of working age. Of those who returned to work, 22% were over the retirement age. This could most likely be explained by each person's financial situation and returning to work may have been a financial necessity. Another explanation could be the historical importance of hard work and ‘self-sacrifice’ ideology, which McKevitt et al26 pointed out when analysing experiences of persons after stroke living in Riga at the beginning of the previous decade. The person who works has a clearly defined role that allows him/her to make a meaningful contribution to society. Although other activities attributable to participation in society are also of importance to the satisfaction with personal roles and quality of life,39 in our opinion the recognition of these roles is lacking in society.
Time is a factor that has a rather strong theoretical role in the experience of disability.3 However, the evidence for it is controversial. For instance, a recent study showed that the functional and motor outcomes did not differ between 2 months and 5 years after stroke,40 but White et al41 reported that the functioning of stroke survivors changes significantly over time and social support and social services are also of importance. The results of this study suggest that the time that has elapsed since a person has been discharged from a rehabilitation centre is of importance in ‘self-care’ activities and the total WHODAS 2.0 score and the role of this dynamic factor, if compared with other factors in the model, is rather small. Therefore, it looks as though the time that has passed after the disabling event is not a factor in and of itself, but gives a frame of reference in which the changes occur. Conversely, age is an independent factor that leads to better outcomes for younger persons.16 ,42 In this study, the statistical contribution of age is rather small, but significant in several aspects of the disability experience.
There was an obvious discrepancy between persons, depending on the language they preferred. Those who chose to fill out the questionnaire in Russian experienced greater problems in self-perceived disability in the ‘participation’ domain versus those who preferred Latvian. This aspect cannot directly influence an outcome of disability perception. The explanations for this significant association could be many. Some studies analysed differences between ethnic subgroups in an American population and explained these differences by the poorer neurological outcomes after stroke.43 ,44 Since the level of dependence at discharge did not differ between the two groups in this study, there is no reason to believe that this could be the cause. Kasmel et al45 found that self-reported health and health behaviour were similar in all three Baltic States, but different from results reported in Finland. As a possible explanation, they mentioned the former economic and political stability in the country. Other different ‘sociocultural’ explanations have been suggested such as organisational barriers of healthcare and issues in the communication between healthcare professionals and patients.46 Our personal experience shows that most of the healthcare professionals have skills to be able to communicate in both languages, depending on the patient's preference. Since the main importance of the language factor was on the ‘participation domain’, the assumption is that reported differences could be due to different health behaviours, beliefs and values between Russian and Latvian speakers. However, the issue of social integration cannot be excluded. To analyse the interactions between all those aspects, further research on this topic should be conducted. There may also be a bias of results due to usage of two translations of WHODAS 2.0. However, using two translations of WHODAS 2.0 allowed us capture a realistic picture of the poststroke population living in Latvia, regardless of language preference.
WHODAS 2.0 is an instrument which is designed to assess self-perceived functioning in the main aspects of disability. The perception of disability experience and recognition of problems can differ between the persons experiencing the condition and the professionals who perform the evaluation.47 That can lead to random variance due to the personal attitudes towards the situation, rather than defined personal factors, used for this study.
The results of this study underline the importance of the rehabilitation process. However, the consequences of stroke and its impact on lives depend on a complex entirety that is formed by interactions of different factors. Both modifiable and non-modifiable factors are included. Recognition of those factors that could be modified gives room for improvements in systems and services. Also, recognition of the factors that are important, but will remain unchangeable, would help in setting the focus for service improvements. The results of an Estonian study that aimed at testing the evaluation of needs for social rehabilitation highlighted the unclear and mixed roles between medical and social rehabilitation, also pointing out other services that should be involved in the process.48
Conclusions
The functional, social and personal factors used in this study could explain up to almost half of the variance in self-perceived level of disability in the chronic phase of stroke in a Latvian stroke population.
The social and personal aspects of a person and their level of independence in daily activities at discharge from an in-patient rehabilitation setting showed equal contribution to the outcome.
Therefore, this highlights the importance of medical and social systems in modification of important factors towards better outcomes and as well as being continuous, the process should be interactive. However, more research is needed to identify other important factors and determine the best approaches for addressing the problems in the most productive manner.
Acknowledgments
This publication has been produced during GB's scholarship period at the University of Gothenburg, thanks to the Visby Programme of the Swedish Institute.
References
Footnotes
Contributors GB has been involved in the design of the study, data collection, performing analysis, interpretation of the results and writing. BS has been involved in data collection and interpretation of the results. AV has been involved in the design of the study and interpretation of the results. KSS has been involved in the design of the study, interpretation of the results and writing. All authors have read and approved the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval The study was conducted to conform to the ethical principles of the Declaration of Helsinki and was approved by the Ethics Committee of Riga Stradiņš University, Latvia (27 September 2012).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data from this study are available on reasonable request from the corresponding author.