Article Text

Abstract
Objectives To reveal the prevalence and associated influencing factors of hepatitis B among a rural residential population in Zhejiang, China, in order to help develop specific control strategies.
Methods We conducted a cross-sectional study among a rural residential population in Zhejiang, China. Stratified multistage cluster sampling was utilised in five districts; a structured questionnaire was used to collect the information such as age, gender, education, occupation, living status, and other health related information of the participants by trained local staff; and the hepatitis B virus (HBV) infection status of the participants was determined by the chemiluminescence immunoassay test. Univariate and multivariate analyses were applied to evaluate the influencing factors of HBV infection. The odds ratio of each related factor was assessed with or without adjustment separately.
Results The mean age of the 16 601 participants (7881 males and 8720 females) who completed the survey was 40.28±19.47 years. The positive rate of hepatitis B surface antigen (HBsAg) was 4.04% (95% CI 3.74% to 4.35%), and 3.85% when standardised by age and gender. Univariate analysis showed that age, educational level, occupation, living status, history of hepatitis B examinations, history of blood transfusion, vaccination, family history, coastal living, and district were the potential influencing factors. Multivariate logistic regression indicated that occupation, living status, history of hepatitis B examinations, vaccination and district were the influencing factors. Undertaking a service-based tertiary industry job (ORa 1.19, 95% CI 0.94 to 1.51) and non-single living (ORa 2.84, 95% CI 2.17 to 3.70) might be risk factors, while vaccination (ORa 0.43, 95% CI 0.34 to 0.53) and history of hepatitis B examinations (ORa 0.71, 95% CI 0.48 to 1.03) were potential protective factors.
Conclusions The prevalence of hepatitis B is at an intermediate epidemic level in a rural residential population in Zhejiang, China. Raising vaccination coverage, especially in adults, is a suitable strategy for the prevention and control of hepatitis B.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study focused on the prevalence of hepatitis B in a rural residential population.
The study involved a large rural residential population and the logistic regression model provided a quantified result of the influencing factors of hepatitis B.
The main limitation of the study was that recall bias could exist due to its cross-sectional design.
Introduction
Hepatitis B is a potentially life-threatening infection caused by hepatitis B virus (HBV), which attacks the liver and can cause both acute and chronic disease. Two billion people have evidence of past or present HBV infection, and, globally, an estimated 240 million people are chronically infected with HBV.1 ,2 More than 6 86 000 people die annually due to complications of hepatitis B, including cirrhosis and hepatocellular carcinoma (HCC).3 Previously, studies revealed that the incidence of HBV-related HCC in adults remains high, and a high serum HBV DNA level increases the risks of cirrhosis and HCC.4 ,5
Overall, nearly half of the global population lives in areas of high hepatitis B endemicity.6 The global prevalence of HBV infection is heterogeneous,2 and the prevalence of hepatitis B is highest in sub-Saharan Africa and East Asia, where 5–10% of the adult population is chronically infected.1 The most recent large, nationwide survey in China was conducted in 2006, which showed that the weighted positive rate of hepatitis B surface antigen (HBsAg) was 7.2% among those aged 1–59 years, and the rate among children aged <5 years was only 1.0%.7 According to the disease distribution maps,2 hepatitis B in China was at a higher intermediate level. Since that time, several studies8–14 have been conducted to investigate the prevalence of hepatitis B in different areas among the general population in mainland China. The reported prevalence was 3.49% in Beijing (2007),8 4.38% in adults in Northeast China (2007),9 7.44% in Anhui Province (2006),10 5.17% in Henan Province (2006–2009),11 7.2% in Northwest China (2010),12 3.17% in Sichuan blood donors (2010–2011)13 and 2.73% in Beijing (2013–2014).14 The rates varied in different areas and at different time periods.
China has the largest rural population and labour resources in the world,15 and rural population flow is the main component of China's overall population flow and has an important impact on the spatial pattern of the population in terms of regional economic and social development.16 A hepatitis B prevalence of 3.7% (642) in a large sample was previously reported,17 while another study18 reported a 6% (124 274) HBsAg positive rate among males in rural areas. The rural economy lags behind the urban economy in China, along with health and education resources.
It is important to identify the prevalence of hepatitis B and the basic procedure for eradicating HBV infection. This study aimed to investigate the prevalence of hepatitis B and its potential influencing factors in a rural residential population in Zhejiang Province, China. By clearly indicating the characteristics of hepatitis B and its associated risk factors, we intend to develop specific prevention and control strategies.
Methods
Study design
A stratified multistage cluster sampling survey was conducted in five districts in Zhejiang Province, China from January 2014 to December 2015. We took geographic characteristics and economic levels into consideration when choosing the five districts in our study: coastal areas such as Putuo and Yuhuan, inland areas such as Shaoxing, Tonglu and Tongxiang, higher economic level areas such as Shaoxing and Tongxiang, and lower economic level areas such as Putuo, Yuhuan and Tonglu. Further stratified sampling was based on the population in rural towns and villages. All participants were registered as rural residents, who had continuously resided in their location for at least 6 months. A total of 22 000 people were recruited, and after 5399 were excluded because of missing information, 16 601 eligible participants ultimately completed the survey. The research ethics committee at the First Affiliated Hospital, School of Medicine, Zhejiang University approved the study, and all participants gave written informed consent.
During the 2-year investigation, a structured questionnaire was designed to collect basic information such as age, gender, ethnicity, education, occupation, living status, medical insurance, etc., and the potential factors related to HBV infection such as history of blood transfusion, surgery, vaccination for hepatitis B, family history of hepatitis B, and whether the participants had moved away from their resident location for more than 3 months, etc.
The investigation was completed by trained staff and local doctors. To increase the response rate, investigators were recommended to visit target houses at an appropriate time, such as nightfall. One percent of questionnaires were randomly selected to be checked for completeness and accuracy. During the investigation, blood samples (5 mL for individuals aged ≥6 years and 2 mL for children aged ≤5 years) were collected from the participants. Sera were separated and stored at −20°C by laboratory staff from the local hospitals. After timely transportation to our state key laboratory of the First Affiliated Hospital, College of Medicine, Zhejiang University, the serum samples were tested by chemiluminescence immunoassay with Abbott reagents (Abbott Laboratories, Abbott Park, Illinois, USA). The positive rate of HBsAg in the population was considered to be the prevalence level of hepatitis B.
Statistical analysis
All collected data were doubly entered into an EpiData V.3.1 software database by two staff, independently. Then we checked the accuracy, consistency and logicality of the data. SAS V.9.4 (SAS Institute Inc, Cary, North Carolina, USA) software was used for data processing and analysis. Social demographic information was analysed by descriptive statistics. Univariate logistic analysis was used to identify potential influencing factors associated with hepatitis B infection; we selected the factors with p<0.1 in the univariate model and conducted a stepwise multivariate logistic model to seek the independent risk factors for hepatitis B. OR, 95% CI and adjusted OR (ORa) for each factor were also calculated. The statistical hypothesis test level was 0.05. GraphPad Prism 6.0 (GraphPad Software, Inc, La Jolla, California, USA) was used to draw the figures.
Results
Characteristics of participants
Of the 22 000 eligible participants, 16 601 completed the survey with a response rate of 75.5%, including 7881 (47.47%) males and 8720 (52.53%) females in five districts. The mean age of the participants was 40.28±19.47 years. The prevalence of hepatitis B in all participants was 4.04% (95% CI 3.74% to 4.35%), and the prevalence was 3.85% standardised by age and gender when using the population of Zhejiang Province as the standard population. The results showed that Zhejiang was an intermediate epidemic area of hepatitis B.
The distribution of the population and the prevalence between the different age groups are shown in figure 1. We observed that those aged <20 years was the group that had the lowest prevalence of hepatitis B, while groups aged 41–60 years had the highest rates. There was a rapid increase in the prevalence between those aged 21–25 years and 26–30 years.
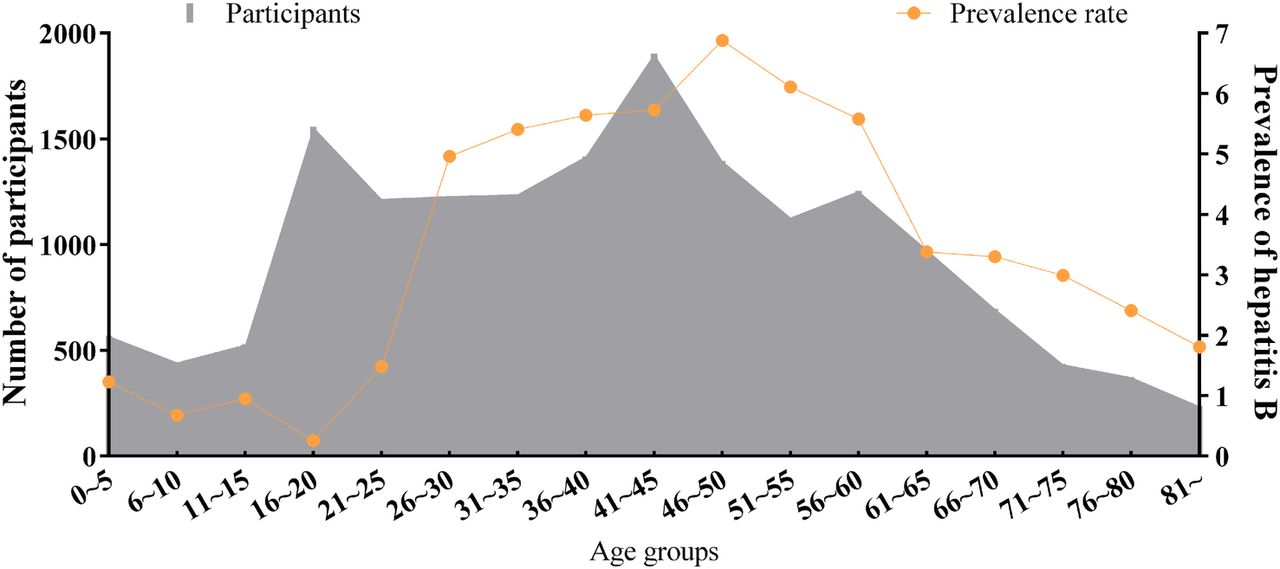
Prevalence of hepatitis B among different age groups.
Among the five districts, Shaoxing had the highest number of participants with 5416 (32.65%), while Yuhuan had the smallest number with 1447 (8.72%) participants. The number of participants was 4370 (26.32%), 3523 (21.22%) and 1845 (11.11%) in the Putuo, Tonglu and Tongxiang areas, respectively. In our study, the prevalence of hepatitis B was highest in Yuhuan (9.81%) and lowest in Tongxiang (2.49%) (figure 2).

Distribution of participants and prevalence of hepatitis B in different districts. HBsAg, hepatitis B surface antigen.
We collected all the relevant data of the participants and their basic characteristics are listed in table 1. Most of the participants' educational level was primary school or lower (44.25%); only 6.5% had college level or higher education, and this group had the lowest prevalence of hepatitis B (2.21%). Only 13.48% of the participants had undergone hepatitis B examinations previously, and few had a history of surgery (3.46%) or blood transfusion (0.57%). There were 6358 (38.30%) participants who had a vaccination history of hepatitis B; this figure was 75.5% in those aged <20 years and only 29.8% in those aged ≥20 years. Of all the participants, 5817 (35.04%) were living in coastal areas.
Characteristics of participants in the study and univariate analysis results
Univariate and multivariate analysis
Univariate analysis showed that age, educational level, occupation, living status, history of hepatitis B examinations, vaccination history of hepatitis B, history of surgery, history of being away 3 months, family history of hepatitis B, and living in a coastal area and district could be the potential influencing factors associated with hepatitis B among the population (table 1).
The stepwise multivariate analysis showed that occupation, living status, history of hepatitis B examinations, vaccination history of hepatitis B and district were the independent influencing factors of hepatitis B in a rural residential population in Zhejiang. The age and gender adjusted model revealed that undertaking a service-based tertiary industry job (ORa 1.19, 95% CI 0.94 to 1.51) and non-single living (ORa 2.84, 95% CI 2.17 to 3.70) were the risk factors for increasing hepatitis B prevalence; while having undergone an examination for hepatitis B (ORa 0.71, 95% CI 0.48 to 1.03) and being vaccinated for hepatitis B (ORa 0.43, 95% CI 0.34 to 0.53) might be the protective factors for hepatitis B (table 2). Figure 3 illustrates the values of OR and ORa in the two logistic models.
Results of multivariate analysis for hepatitis B

{kind=link}
{kind=link}
{kind=link}
Values of OR and adjusted OR (ORa) in the logistic models.
Discussion
Prevalence of hepatitis B
Viral hepatitis is a leading cause of death and disability worldwide. Acute hepatitis infection, cirrhosis and liver cancer were the 10th leading cause of death worldwide in 1990, and the seventh leading cause of death in 2013. Indeed, the number of deaths worldwide attributable to viral hepatitis increased by 63% from 1990 to 2013.19
The prevalence of hepatitis B in all rural residential participants was 4.04% in Zhejiang (3.85% when standardised by age and gender). Our results indicated that the Zhejiang rural residential population would be categorised as an intermediate group and that the prevalence of hepatitis B was significantly lower than 9.8% reported in 1992 and 7.2% reported in 2006 across China.7 Following a series of interventions conducted by the Chinese government, the hepatitis B epidemic declined significantly. A larger nationwide survey would be needed to assess the current epidemic of hepatitis B in China to provide the epidemiological features and update the controlling or prevention strategies, especially in the rural population.
Influencing factors of hepatitis B
There was no significant association between hepatitis B prevalence and age in our study, even though previous studies referred to age as a factor20–22 and showed that an older age group had a higher prevalence in the population. Our univariate analysis also indicated this phenomenon. We thought this outcome was a result of confounding by hepatitis B vaccination or other factors. A previous study also reported an inverse result.23 For the factor of gender, the results were varied. Previous studies11 ,21 ,23–25 showed that the prevalence was higher in males than in females, while one study found that there was no association between gender and hepatitis B,20 which was similar to ours.
Our study showed that education was not an independent influencing factor on hepatitis B, which was also noted in other studies.26 ,27 However, there could be a possible trend of decreasing hepatitis B prevalence with increasing educational level from our univariate analysis, as shown in table 1; it can be observed that the population with a higher educational level had a lower hepatitis B prevalence. One possible explanation is that among the higher-educated population there is better awareness of infectious disease prevention and a higher acceptance of vaccination; furthermore, having at least a college education (OR 2.55, 95% CI 1.28 to 5.07) was an important predictor of vaccine completion.28
We found that only 13.48% of all participants had undergone a previous hepatitis B examination, and that there was a lower prevalence of hepatitis B among those participants; however, there was a higher prevalence in those participants who had not been previously examined. We could infer that those infected by HBV, who had not been diagnosed by the examinations, could be the potential source of hepatitis B. By encouraging people to take part in hepatitis B examinations, along with routine physical examinations, we could benefit by: first, finding out those who are infected; second, treating those who are infected immediately; and third, taking the opportunity to raise awareness of hepatitis B among the population, especially in rural areas.
Compared to other types of occupation, service-based tertiary industry occupations seemed to be a risk factor, along with non-single living (ORa 2.84, 95% CI 2.17 to 3.70). The factors mentioned above had the same feature; that they are likely to result in more communication between people. We should take these into consideration, since hepatitis B is an infectious disease and has a sign of clustering among the population.
Hepatitis B epidemics are scattered in different areas globally,2 ,22 and hepatitis B prevalence also varied among different districts in our study. These circumstances would be caused by geography, economic level, population density, living habits or other factors. Economic level seems to be a potential factor, since areas of lower economic level such as Yuhuan had a higher prevalence of hepatitis, and areas of higher economic level such as Shaoxing and Tongxiang had a lower prevalence. Regardless of all these features, we should consider district as a non-negligible factor, especially the district with a high prevalence, when developing and implementing strategies for fighting hepatitis B.
Control strategies for hepatitis B
WHO adopted the first-ever global hepatitis strategy with the goal of eliminating viral hepatitis B and C as public health threats by 2030, which was defined as a reduction in incidence by 90% in new chronic infections and mortality by 65% for viral hepatitis B and C.29 Currently, hepatitis B is a major health problem and has a significant socioeconomic impact all over the world.30 HBV vaccination is the mainstay of HBV prevention and is the most effective prevention strategy.31 ,32
The Chinese government has made great progress with hepatitis B vaccination.33 The national hepatitis B immunisation plan was established in 1992. In 2002, the Global Alliance on Vaccine and Immunisation (GAVI) partnered with the government of China to provide free hepatitis B vaccine34 and full integration into the routine immunisation programme; the vaccine was provided completely free to infants nationally in 2005.35 The carrier rate in Chinese children aged <5 years fell from 10% in the 1990s to <1% in 2006 and to 0.32% in 2014.36 Recently, WHO estimated that the protection rates of the timely birth dose and third dose of hepatitis B vaccine (HepB3) among newborns in China, were 96% and 99%, respectively.37 Our study showed that hepatitis B vaccination (ORa 0.43, 95% CI 0.34 to 0.53) was the protective factor for hepatitis B, and the same results have been observed in other studies.12 ,13 ,26
Regarding vaccination coverage related to the economic status, a former study suggested that higher HBV vaccination coverage rates among adults were obtainable. The user fees, time needed for vaccination and travel costs acted as economic barriers to vaccination.38 Hepatitis B vaccination has been reported as low as 13.89% in rural China.39 We call for strengthening of HBV vaccination in rural areas, and raising the vaccine coverage rate.
Our survey also showed that the vaccination rate was 75.5% in persons aged <20 years, while it was only 29.8% in those aged ≥20 years. Expansion of the hepatitis B vaccination programme since 1992 has been accompanied by a decrease in the nationwide prevalence of hepatitis B. Preventing hepatitis B through vaccination is currently the most efficient way to decrease the incidence of HBV-related cirrhosis and liver cancer, and reduce the HBV reservoir.30 The role of the vaccination programme for the effective control of hepatitis B should be emphasised.40 In the near future, efforts for hepatitis B vaccination should be focused on adults, under the consideration of policies for universal vaccination, especially in those areas with high hepatitis B endemicity.
Limitation
This study was cross-sectionally designed, and we could not exclude the cases of acute infection. Thus hepatitis B prevalence may be overestimated in the population when using the HBsAg positive rate as the level of chronic HBV infection. There was also a certainty of recall bias in this study design. Additionally, the sample sizes were not balanced between districts in our study. We considered taking a vaccination history of hepatitis B as an indicator of vaccine success due to the effectiveness of vaccination.30 To interpret the results, we simply divided the variables into a few groups, such as occupation. A more precise classification of factors could be assessed in later studies, along with more potential factors, such as family income.
Conclusions
Although our study showed that the Zhejiang rural area is categorised as being at an intermediate epidemic level for hepatitis B in China, there remains the important issue and formidable challenge of dealing with the problem of hepatitis B in rural areas among the resident population. Specific methods such as raising the coverage of vaccination, particularly in adults, are suitable and effective strategies to prevent and control hepatitis B in Zhejiang rural areas. Furthermore, increasing the percentage of the hepatitis B examinations may also be considered as a potential strategy. The significant findings in this study, with potential implications for public health, would be helpful to China and other countries in the fight against hepatitis B.
References
Footnotes
SY and CD contributed equally.
Contributors LL, JR, BR, JY and SY conceived and designed the study. CD, YC, JW, CY, PC, KX, MD, YL, JL, PY, WR, YQ, QC and YZ collected cleaned, analysed the data and revised the paper. CD and SY wrote the first draft of the paper, contributed to figures and paper preparation. All authors critically revised the paper and gave final approval for publication.
Funding This study was supported by the Mega-Project for National Science and Technology Development under the 12th 5-Year Plan of China (2014ZX10004008, 2013ZX10004904), the National Natural Science Foundation of China (grant numbers 81001271, 81672005), the key project for data centre of the National Natural Science Foundation of China and Guangdong Provincial Government (U1611264), and the self-research and open-research project of State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, College of Medicine, Zhejiang University, China (2016KF11).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.