Article Text

Abstract
Introduction Emergency management of upper cervical spine injuries often requires cervical spine immobilisation and some critical patients also require airway management. The movement of cervical spine created by tracheal intubation and cervical spine immobilisation can potentially exacerbate cervical spinal cord injury. However, the evidence that previous studies have provided remains unclear, due to lack of a direct measurement technique for dural sac's space during dynamic processes. Our study will use myelography method and a wireless human motion tracker to characterise and compare the change of dural sac's space during tracheal intubations and cervical spine immobilisation in the presence of unstable upper cervical spine injury such as atlanto-occipital dislocation or type II odontoid fracture.
Methods and analysis Perform laryngoscopy and intubation, video laryngoscope intubation, laryngeal tube insertion, fiberoptic intubation and cervical collar application on cadaveric models of unstable upper cervical spine injury such as atlanto-occipital dislocation or type II odontoid fracture. The change of dural sac's space and the motion of unstable cervical segment are recorded by video fluoroscopy with previously performing myelography, which enables us to directly measure dural sac's space. Simultaneously, the whole cervical spine motion is recorded at a wireless human motion tracker. The maximum dural sac compression and the maximum angulation and distraction of the injured segment are measured by reviewing fluoroscopic and myelography images.
Ethics and dissemination This study protocol has been approved by the Ethics Committee of the State Medical Association Rhineland-Palatinate, Mainz, Germany. The results will be published in relevant emergency journals and presented at relevant conferences.
Trial registration number DRKS00010499.
- iaryngoscopy
- intubation
- laryngeal
- fiberoptic
- cervical collar
- dural sac
- myelography
- unstable upper cervical spine
- protocol
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- iaryngoscopy
- intubation
- laryngeal
- fiberoptic
- cervical collar
- dural sac
- myelography
- unstable upper cervical spine
- protocol
Strengths and limitations of this study
This study will develop a measurement technique for dural sac's space, ensure us to directly measure the real-time change of dural sac's space during manoeuvres.
This study will originally develop an atlanto-occipital dislocation model in an intact cadaver and addresses the change of dural sac's space during emergency management.
This study uses a wireless human motion tracker to capture the movement of cervical spine by measuring the changes in three-dimensional orientation of the head relative to the trunk.
Because the information about the injury of cervical spine and the airway devices would be detected under fluoroscopic view, the outcome assessor could not be fully blinded.
Introduction
About 30% of cervical spine injuries occurred in the sites from occiput to C2;1 C1 and C2 injuries were postmortem diagnosed in 22.6% of 312 deceased after traffic trauma.2 The upper cervical spine injuries are frequently associated with significant neurological deficits and high mortality as a consequence of spinal cord injury or brainstem injury.3 4 Among these, the atlanto-occipital dislocation (AOD) is considered as the most fatal injury of the cervical spine,4–6 whereas C2 is the most frequent level of cervical spine injury.7–9 Furthermore, type II odontoid fracture is reported as the most frequent site of injury to C2.7 Improvements of cervical spine immobilisation, airway management and more progressive treatment have reduced the mortality of upper cervical spine injury.
Maintaining a secure airway and cervical spine immobilisation are often required in most patients with unstable cervical spine injury; some critical patients even require tracheal intubation.10–12 However, tracheal intubation and application of a cervical collar in the setting of unstable cervical spine can potentially exacerbate cervical spinal cord injury.13–16 Previous studies suggest that the main movement of the cervical spine during tracheal intubation is extension; the maximum movement occurs in the atlanto-occipital level, followed by atlanto-axial level, and below C3 segments show less movement.17 18 The study concerning intubation biomechanics in the setting of AOD is rare; most previous relative studies focused on the unstable C1/C2 segment. It has been demonstrated that the movement of unstable C1–C2 segment during laryngoscopy and intubation in the presence of C2 fracture reduce the little space available for the cord of cervical spine, and does not exceed normal value in maximum flexion and extension.11 19 Furthermore, McCahon et al 11 have found no significant differences between the Airtraq and Macintosh or the Airtraq and McCoy on cadaveric models of type II odontoid fracture. However, due to the lack of an effective measurement method, compression on dural sac was revealed unclearly. Therefore, this study is designed to previously perform myelography on each cadaver, enabling us to directly assess the changes of dural sac's space during airway managements and cervical collar application.
As an effective method of external immobilisation,20 21 manual inline stabilisation is recommended during intubation using direct laryngoscopy to minimise cervical spine motion. However, about 12% of the patients with cervical spine injuries are not immobilised.22 Especially during airway management, manual inline stabilisation may be neglected due to a significant decrease in glottis view and an increased difficulty in intubation.23 24 There are doubts if external immobilisation is applied in general. Thus, this study is designed to determine cervical spine motion and dural sac compression during airway management without external immobilisation.
Cervical collars are widely applied in cervical spine injury, specifically intended to restrict the cervical spine in a neutral position and protect against secondary injury to the spinal cord. However, a recent case report documents that a patient with ankylosing spondylitis applied a cervical collar after cervical spine injury, resulting in neurological deterioration and finally death.16 Furthermore, a cadaveric study shows that application of a cervical collar generates a separation within injured cervical segment in the presence of unstable upper cervical spine injury.25 Movement of unstable cervical spine segment caused by application of a cervical collar may create secondary injury to cervical spinal cord, and the compression of dural sac and spinal cord during cervical collar application still remains unclear.
Objective
The primary aim of this study is to characterise and compare the change of dural sac’s space during laryngoscopy and intubation, video laryngoscope intubation, laryngeal tube insertion, fiberoptic intubation and application of a cervical collar in the presence of unstable upper cervical spine injury such as AOD or type II odontoid fracture.
Methods and analysis
Setting
This trial is a prospective, investigator and observer blinded, randomised, superiority, crossover trial. This study will be carried out in the Institute of Anatomy at Heidelberg University. This study will begin in February 2017. Flow diagram through the trail is outlined in figure 1. Adherence reminder meeting will take place before the beginning of the study. Every team member and research physician will be informed the importance of following flow diagram.

Flow diagram through the study. AOD, atlanto-occipital dislocation.
Eligibility criteria
We will recruit fresh cadavers donated for medical research. These fresh cadavers are frozen shortly after mortem and are thawed to room temperature for simulating the elasticity of joints and soft tissues in living situation. Fresh cadavers will be eligible for the study inclusion if they are <5 days postmortem.
Before experiment, a team member from the institute of anatomy will check every deceased’s medical records for exclusion criteria.
Exclusion criteria will be:
Cervical spine disease
Cervical spine surgical history
Neck trauma
Upper airway disease
Sample size
We will recruit 12 fresh cadavers for this study, and 6 cadavers for each injured level. The data from preliminary experiment demonstrate an SD value of 0.51 mm for the change of dural sac's space during tracheal intubation. To achieve α=0.05 at power 80%, six cadavers for each model will be required to detect a 0.58 mm difference for the change of dural sac's space during manoeuvre. Spinal cord will be compressed when spinal canal's space reduce more than 9 mm in C1/C2 level;26 thus, the mentioned sample size should be sufficient to detect the change of dural sac's space and identify secondary injury to the spinal cord.
Recruitment
We will recruit fresh cadavers from the body donation programme at Heidelberg University. A written informed consent will be required in the enrolment of cadavers. Members of the public have agreed to donate their body after death and provided written informed consent to be used in medical research and education during their lifetime. A team member from the institute of anatomy at Heidelberg University will obtain informed consent from potential trial participants or authorised surrogates. A secretary from research group will provide study information pamphlet, recruitment plan to the authorised representatives of the body donors and some interested third parties, and answer the relevant questions.
Randomisation
The order of both cadavers and interventions will be generated by a randomisation service provided by randomiser, and the information of cadavers will not be disclosed, to ensure concealment. It will not release the randomisation until the study has been finished.
Blinding
The intervention provider will be blinded from the fluoroscopic images and the wireless human motion tracker system during the entire trial. Both the outcome assessor and the data analyst will be blinded from the information of cadavers and interventions. The personal information about potential and enrolled cadavers will be collected and maintained in the institute of anatomy, and the information will be blinded to other members of research group.
Intervention
All interventions will be performed by an anesthesiology resident in random order. We will study the following interventions:
Orotracheal intubation using conventional direct laryngoscopy with Macintosh-blade size 3 and intubation stylet
Orotracheal intubation using video laryngoscopy (Ambu King Vision aBlade, Ambu GmbH, Bad Nauheim, Germany)
Orotracheal intubation using a flexible fiberoptic device (aScope 3, Ambu GmbH, Bad Nauheim, Germany)
Insertion of a laryngeal tube (LTS-D, VBM Medizintechnik GmbH, Sulz, Germany)
Application of a cervical collar (Stifneck Select extrication collar, Laerdal Medical GmbH, Puchheim, Germany)
A Magill tracheal tube will be used for all tracheal intubations. The laryngeal tube was inserted as recommended by the manufacturer. The head will be held in neutral position during application of the cervical collar. During intubation procedures, there will be no external stabilisation.
Development of cadaveric models
AOD cadaveric model
To our knowledge, there is no cadaver study that has formally reported to create an AOD model in an intact cadaver. Thus, we attempt to develop an original cadaveric model by referring to the anatomical studies about AOD. Previous anatomical studies have documented that the rupture of both tectorial membrane and alar ligament may play a critical role in causing an AOD.27–29 Furthermore, the superior band of cruciate ligament also provides structural support for the atlanto-occipital junction.27 A posterior surgery is performed on a cadaver by severing the tectorial membrane, alar ligament and superior band of cruciate ligament to develop an AOD cadaveric model.
The model will be confirmed during flexion and extension by lateral video fluoroscopy. According to the consensus statement of measurement for upper cervical spine injuries,30 the value of basion-dental interval (BDI) measured more than 12 mm is highly suggestive of AOD (the exact method of measurement is described below).
Type II odontoid fracture cadaveric model
This study uses Donaldson et al’s19 cadaveric model. We will make a transverse incision about half inch in the posterior pharynx via transoral approach, and then perform an osteotomy in the base of odontoid to create a type II odontoid fracture.
The model is confirmed when a fracture at the odontoid's base is documented during flexion and extension under lateral video fluoroscopy.
Myelography
The cadavers are positioned prone on a table, a mini-incision surgery is performed to expose dural sac in upper thoracic spine via posterior approach, then a subarachnoid space puncture is made and a tube towards upper cervical spine is placed, and the contrast medium (Optiray300, 300 mg/mL) is pump injected through the tube into dural sac. This method of puncture ensures that contrast has sufficiently worked in cervical dural sac.
Outcomes
Dural sac's space (myelography method)
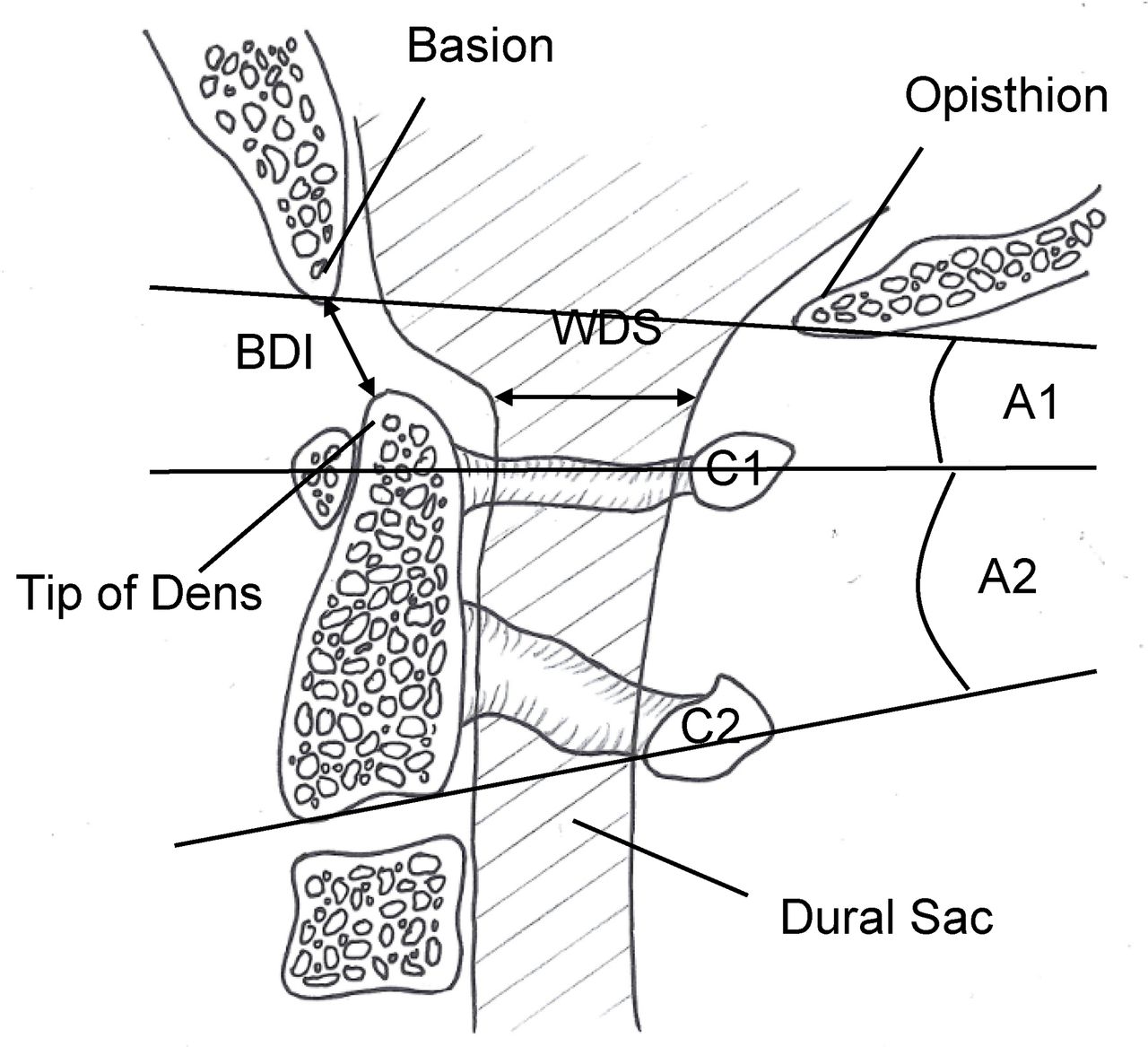
This study is primarily designed to measure the change of dural sac's space. We assess the dural sac's space by directly measuring width of dural sac (WDS) in myelography, WDS is defined as the narrowest distance of the dural sac in the injured level. The WDS of unstable cervical spine is obtained at the narrowest portion, and then the stable one is subsequently measured at the corresponding portion. A decrease of WDS represents the maximum amount of compression on dural sac (figures 2 and 3).

Fluoroscopy and myelography images demonstrating measurement techniques in atlanto-occipital dislocation model. BDI: the distance between basion and the tip of dens; WDS: the narrowest sagittal distance of the dural sac in the injured level; A1=angulation of OC–C1 segment: the angle of intersection between the line drawn from basion to opisthion and midpoint line of C1; A2=angulation of C1–C2 segment: the angle of intersection between midpoint line of C1 and inferior endplate line of C2. BDI, basion-dental interval; WDS, width of dural sac.

Fluoroscopy and myelography images demonstrating measurement techniques in type II odontoid fracture model. A3=angulation of C2–C3 segment. D=distraction of C1–C2 segment: the perpendicular distance between the posterior ring of C1 and the superior spinolaminar line of C2. WDS, width of dural sac.
Basion-dental interval
According to the consensus statement of measurement for upper cervical spine injuries,30 BDI is measured through the distance between basion and tip of dens; it is recommended by Spine Trauma Study Group as standardise measurement techniques to describe the spatial relationship between occiput and atlas. The value of BDI more than 12 mm is highly suggestive of AOD (figure 2).
Angulation
The angle of intersection of reference lines on each vertebral body is measured as angulation of each cervical spine motion segment,11 19 31 the measurement is described below (figures 2 and 3). The angulation we measured involves injured segment, as well as the adjacent superior and inferior segments. The position before manoeuvres is recorded as neutral position; we define extension as positive value and flexion as negative value.32 33
Distraction of C1–C2
Distraction is measured through the perpendicular distance between the posterior ring of C1 and the superior spinolaminar line of C219 (figure 3).
Movement of the whole cervical spine
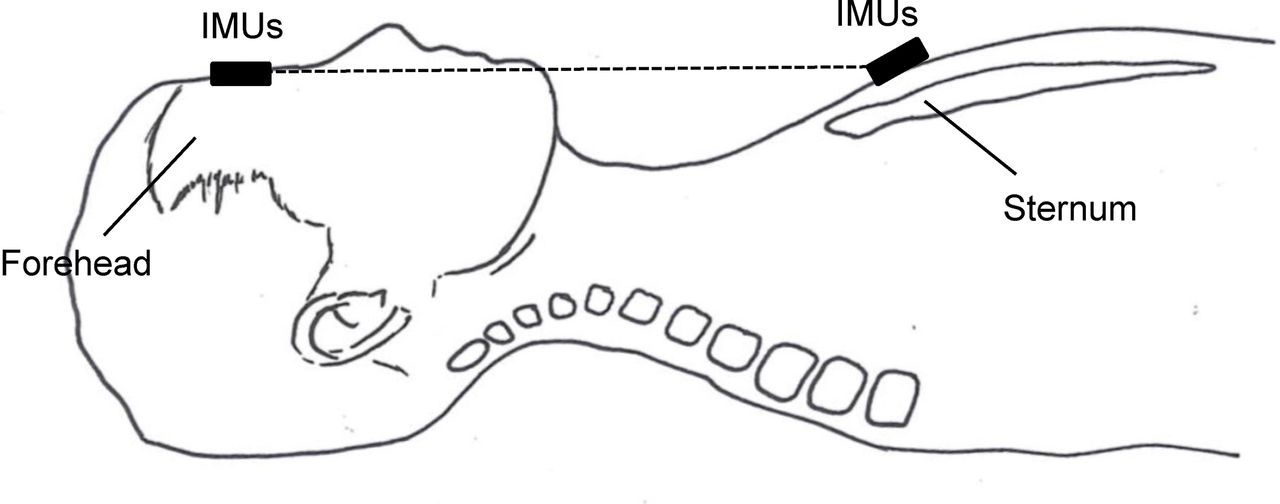
We use a wireless human motion tracker system (Xsens Technologies, Enschede, The Netherlands) to capture the movement of cervical spine during manoeuvres. The use of tracker system is based on the inertial measurement units (IMUs), which is a wearable multisensor and comprises accelerometer, gyroscope and magnetometer. We assess the movement of the whole cervical spine by quantifying the change in three-dimensional (3D) orientation of the head relative to the trunk.34 35 Two IMUs are respectively placed on the forehead and sternum of each cadaver (figure 4). The IMUs output angular orientation of each site, and the relative angular change is calculated in the terminal. The movement of the whole cervical spine is recorded in both static and dynamic conditions with a high accuracy and precision.35 The state of cadaver positioned supine on a table before manoeuvres is recorded as the neutral state. We define extension as positive values and flexion as negative values. We assess rotation and lateral bending using the absolute value, regardless of right or left of rotation and lateral bending.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The movement of the whole cervical spine. Two IMUs are placed on forehead and sternum and recorded as the neutral state. We measure the change of 3-dimensional orientation between the motion state and the neutral state as the movement of the whole cervical spine. IMUs, inertial measurement units.
Outcomes and prioritisation
The primary outcomes for this study are WDS during laryngoscopy and intubation, video laryngoscope intubation, laryngeal tube insertion, fiberoptic intubation and cervical collar application in the presence of AOD or type II odontoid fracture. WDS quantifies the compression of spinal canal or spinal cord and indicates secondary injury to the cervical spinal cord, which frequently associated with significant neurological deficits and high mortality.
The secondary outcomes are simultaneous motions of injured segment such as angulation, distraction and movement of the whole cervical spine during tracheal intubations and cervical collar application.
Data management
Data collection process
The following data will be collected: identifiable information of cadavers, exclusion criteria by checking the deceased’s medical records, interventions (tracheal intubations, cervical collar application), dural sac's space on myelography and the motion of injured segment (angulation, distraction) are simultaneously recorded at video fluoroscopy; motion of the whole cervical spine will be recorded at wireless human motion tracker.
Monitoring of data quality
Video fluoroscopy using a Philips Veradius C-Arm (Philips, Amsterdam, The Netherlands). Real-time fluoroscopic images with previously performing myelography were stored on the Trust Picture Archiving Computer System. Data are stored directly on being recorded and backed up regularly; the lead investigators will have access to the trial dataset. Two outcome assessors will be involved to independently evaluate the fluoroscopy images together. Data requiring manual calculation in myelography and video fluoroscopy images will be measured by two assessors. Consistent outcomes are reported, and disagreement will be resolved by checking myelography and video fluoroscopy reviewed images together and make a consensus decision. Another assessor will be who process the data from wireless human motion tracker. All the assessors will be blinded from the information of cadavers and interventions. This study will last a week from enroll fresh cadavers to conduct and finish the trial, no interim analysis will be performed during the study.
Statistical analysis
Continuous variables are reported as mean with SD. The Wilcoxon signed-rank test is used to make pairwise comparisons in stable versus unstable upper cervical spine for each intubation and cervical collar application; the Mann-Whitney test is used to make non-paired comparisons between tracheal intubations using SPSS Statistics V. 22.0 (IBM, Ehningen, Germany).
Ethics and dissemination
Ethics approval
The study proposal is approved by Ethics committee of the State Medical Association Rhineland-Palatinate, Mainz, Germany. Registry No. 837.156.16 (10475). The study is registered in the German Clinical Trials Register (DRKS) with the ID DRKS00010499. Any modifications to the protocol may impact the conduct of the study and any amendment will be agreed on by Spine Motion Reaearch Group and approved by the ethics committee.
Dissemination
The results will be published in highly cited and open-access peer-reviewed emergency journals, and we will present findings at relevant conferences. The datasets used and analysed during the study will be available from the corresponding author on reasonable request.
Discussion
This study will specifically create AOD cadaveric models and type II odontoid fracture cadaveric models simulating unstable upper cervical spine injuries. Airway interventions and cervical spine immobilisation will be performed to evaluate the current emergency management of unstable upper cervical spine injuries. We improve the measurement to record the changes of dural sac’s space during dynamic processes. We try to discuss the risks and benefits of four kinds of intubation techniques in the setting of unstable upper cervical spine. Meantime, we will quantify the compromise of dural sac during cervical collar application. These findings will offer some useful information to improve the emergency care of unstable upper cervical spine injuries.
MRI is considered as an essential step in diagnosis of spinal cord injury. A recent study36 recommended an MRI-based measurement to diagnose spinal stenosis through assessing the spinal cord occupation rate, due to a higher imaging modality and reliability. Since this study is designed to record the entire dynamic process during performing interventions, MRI does not meet the requirement. Previous relative studies11 19 assessed spinal cord compression by measuring the decrease of spinal canal in a video fluoroscopy and neglected the bulge of surrounding soft tissue. Thus, we improve the measurement method to directly measure dural sac by preforming an additional meylography.
In this study, we observe both intervertebral movement of injured levels and movement of the whole cervical spine. We assess that intervertebral movement mainly focus on the injured segments, which involve the superior and inferior segments. Since cervical spine motion manifests as extension at upper cervical spine and as flexion at lower cervical spine,23 37 both movements should be involved. The movement of adjacent lower cervical spine is measured in fluoroscopic view, and the overall movement of lower cervical spine can be assessed through analysing the difference between the movement of upper cervical spine and the whole cervical spine. We assess the movement of the whole cervical spine by measuring the change in 3D orientation of the head relative to the trunk motion. The measurement could be criticised in the fact that the experiment only provides outcomes of orientation and cannot measure translational motions. Translational motions may create or exacerbate spinal cord injury during cervical spine management. However, previous studies suggest that the predominant motion of cervical spine during intubation is extension17 18 and the orientation motions can be used to represent mainly movement of cervical spine during tracheal intubation.
Another important question is whether cadavers are valid and credible models, and whether the biomechanical properties of soft tissues and cervical joints in fresh cadavers are similar to the living patients. In recent studies of biomechanics, a non-significant difference in cervical spine motion between fresh cadavers and patients in both stable and unstable situations has been documented.18 31 Thus, the fresh cadavers are valid models to simulate unstable upper cervical spine injuries, and outcomes of the cadaveric study relevant to clinical situation.
A limitation of the study described is the small number of subjects, and the small sample size may increase the possibility of a type II error. However, six cadavers for each traumatic model will have an 80% power and 5% level of significance to detect a 0.58 mm difference in the change of dural sac's space, the value is far less than 9 mm that creates secondary injury to the spinal cord.26 Furthermore, the previous cadaver studies with small sample size still had 80% power to detect a significant difference in space available for the spinal cord between the laryngoscopes.11 19 31 38
Acknowledgments
The authors are grateful to Dr Chen Yiheng for valuable suggestions and Carola Lingner for the graphic design during the development of our protocol. The authors also thank Silke Weissenmayer, Dr Zhou Zizi, Anne Stehr and Sarah Doll for supporting this research project.
References
Footnotes
Contributors SL, EP, NS, FW and MK participated in the design of the study and reviewed the literature. SL, NS, PH, EP, FW and MK developed the protocol. NS, EP, PH, MM and MK participated in study coordination. All authors helped to draft the manuscript and approved the final version.
Competing interests None declared.
Patient consent Obtained
Ethics approval Ethics Committee of the State Medical Association Rhineland-Palatinate, Mainz, Germany.
Provenance and peer review Not commissioned; externally peer reviewed.