Article Text

Abstract
Introduction Emergency telephone calls placed by bystanders are crucial to the recognition of out-of-hospital cardiac arrest (OHCA), fast ambulance dispatch and initiation of early basic life support. Clear and efficient communication between caller and call-taker is essential to this time-critical emergency, yet few studies have investigated the impact that linguistic factors may have on the nature of the interaction and the resulting trajectory of the call. This research aims to provide a better understanding of communication factors impacting on the accuracy and timeliness of ambulance dispatch.
Methods and analysis A dataset of OHCA calls and their corresponding metadata will be analysed from an interdisciplinary perspective, combining linguistic analysis and health services research. The calls will be transcribed and coded for linguistic and interactional variables and then used to answer a series of research questions about the recognition of OHCA and the delivery of basic life-support instructions to bystanders. Linguistic analysis of calls will provide a deeper understanding of the interactional dynamics between caller and call-taker which may affect recognition and dispatch for OHCA. Findings from this research will translate into recommendations for modifications of the protocols for ambulance dispatch and provide directions for further research.
Ethics and dissemination The study has been approved by the Curtin University Human Research Ethics Committee (HR128/2013) and the St John Ambulance Western Australia Research Advisory Group. Findings will be published in peer-reviewed journals and communicated to key audiences, including ambulance dispatch professionals.
- Health services administration & management
- Protocols & guidelines
- Public health
- Qualitative research
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The study will provide a better understanding of factors impacting on the accuracy and timeliness of ambulance dispatch.
The study design will be mixed-methods and interdisciplinary.
This study will focus primarily on one of the most commonly used dispatch protocols and results may not be applicable to other dispatch protocols.
The study will be limited to emergency calls spoken in the English language and may therefore not be applicable to other languages.
The sample size will be limited to 200 calls to allow for qualitative analysis, which may limit the generalisability of the results to all emergency calls.
Introduction
Out-of-hospital cardiac arrest (OHCA) is a time-critical emergency in which every minute of delay negatively impacts on patient survival.1 2 The first link in the chain of survival3 is dependent on a layperson’s actions, as it requires a bystander to call the emergency telephone number (‘000’ in Australia) for help. The ensuing telephone call is crucial to the recognition of cardiac arrest by the call-taker, fast dispatch of the Emergency Medical Services (EMS) and initiation of basic life support instructions, such as bystander cardiopulmonary resuscitation (CPR) and defibrillation.4
Many emergency call centres worldwide use standardised protocols, such as the Medical Priority Dispatch System (MPDS),5 a well-established algorithm-based approach to process and prioritise medical emergency calls. The MPDS protocol includes instructions for bystander-CPR when OHCA is identified during the emergency call. The proportions of OHCA recognition and bystander-CPR are two key areas for improvement: a recent systematic literature review6 found a median recognition proportion of 74% (with marked variability) across 16 studies, while the proportion of recognised cases of OHCA who received bystander-CPR has been reported to be 32% across 19 studies.7 A number of studies have analysed the audio recordings of OHCA calls to understand the process of patient assessment,8 OHCA recognition9–15 and telephone-mediated instructions for basic life support.16–20 Studies which focused on the language used have attempted to identify keywords as indicators of cardiac arrest10 or to identify common causes of communication difficulties.21 Very few studies have focused on the interactional dimension of this decisive exchange between bystander and call-taker. There are two notable exceptions. An observational study conducted in Scotland22 matched the content of audio recordings to steps in the dispatch protocol (MPDS). The authors thus identified which stages took the longest and advocated for a more detailed content analysis to better understand the interactional difficulties found in OHCA calls. More recently, in France, an experimental study23 showed that call-takers with medical training were influenced in their decisions by the acoustic properties of callers’ voices.
Much research remains to be done for a better understanding of what goes on between caller and call-taker in OHCA calls. Most medical studies to date have only cursorily looked at the actual content and form of calls and have not used the meticulous methodologies specifically designed to analyse speech and interaction, for example, Conversation Analysis (CA).24–26 Emergency calls in particular have been extensively investigated by social scientists,27–29 although the focus has not been on OHCA. Some of these studies analysed ‘failed emergency calls’, that is, when communication issues (or ‘interactional trouble’)30 between caller and call-taker led to fatal consequences31–34; while others focused on how certain structures and actions are managed in calls. Topics have included how callers describe the emergency,35 36 make requests37 and complaints38 and how call-takers use questions.39 40 One study conducted in South Africa41 successfully used an interactional analysis of call openings to reduce call length. However, sociological and linguistic research on the topic has tended to consist of small case studies and was disconnected from other information about dispatch, patient information and medical care and outcome.
Aims and objectives
The aim of our study is to apply linguistics, social science and health science research methods to assess OHCA calls and provide a deeper understanding of the interactional dynamics between caller and call-taker. We will identify the interactional strategies deployed in a real-life, distressing situation for callers. Once such ‘endogenous practices’42 have been assessed, our objective is to propose the generalisation of the most successful strategies which are already used by some call-takers in some calls. This type of approach has been shown to be a very effective way to manage common obstacles in various types of institutional talk,42 such as mediation services,43 telephone helplines44 and police investigative interviews.45 In sum, our objectives are to:
Identify interactional factors which may improve/worsen dispatch.
Assess the current communicative strategies used by call-takers.
Methods
Framework
Our research objectives will be addressed through a linguistic and interactional analysis of a set of emergency calls concerning OHCA, to be conducted from August 2016 to December 2018. Our study will employ a mixed-methods approach,46–48 combining the frameworks of qualitative-oriented CA,25 26 49 and quantitative-oriented Corpus Linguistics.50–52 We will first collect data (in linguistic terms, a corpus) and code it in such a way as to provide a first layer of linguistic analysis. The corpus will be used to ask a variety of research questions about different interactional factors which may impact dispatch and the necessary cooperation between caller and call-taker to provide basic life support instructions before the paramedics arrive on scene. Our approach being inductive and data driven, the specific research questions can only arise once the data are collected and analysed. Immersion in the calls will allow us to identify linguistic phenomena of interest, which we will then investigate following the methods described in the present paper. At this stage, we may only offer a few suggestions of potential research topics. For example, we may choose to analyse in more depth the sequences that are known to be difficult in OHCA calls, such as detecting ineffective and agonal breathing53 and providing instructions for bystander-CPR.16 20 The different steps of the study protocol are summarised in figure 1 and explained below.

Summary of the study protocol for linguistic analysis.
Data collection
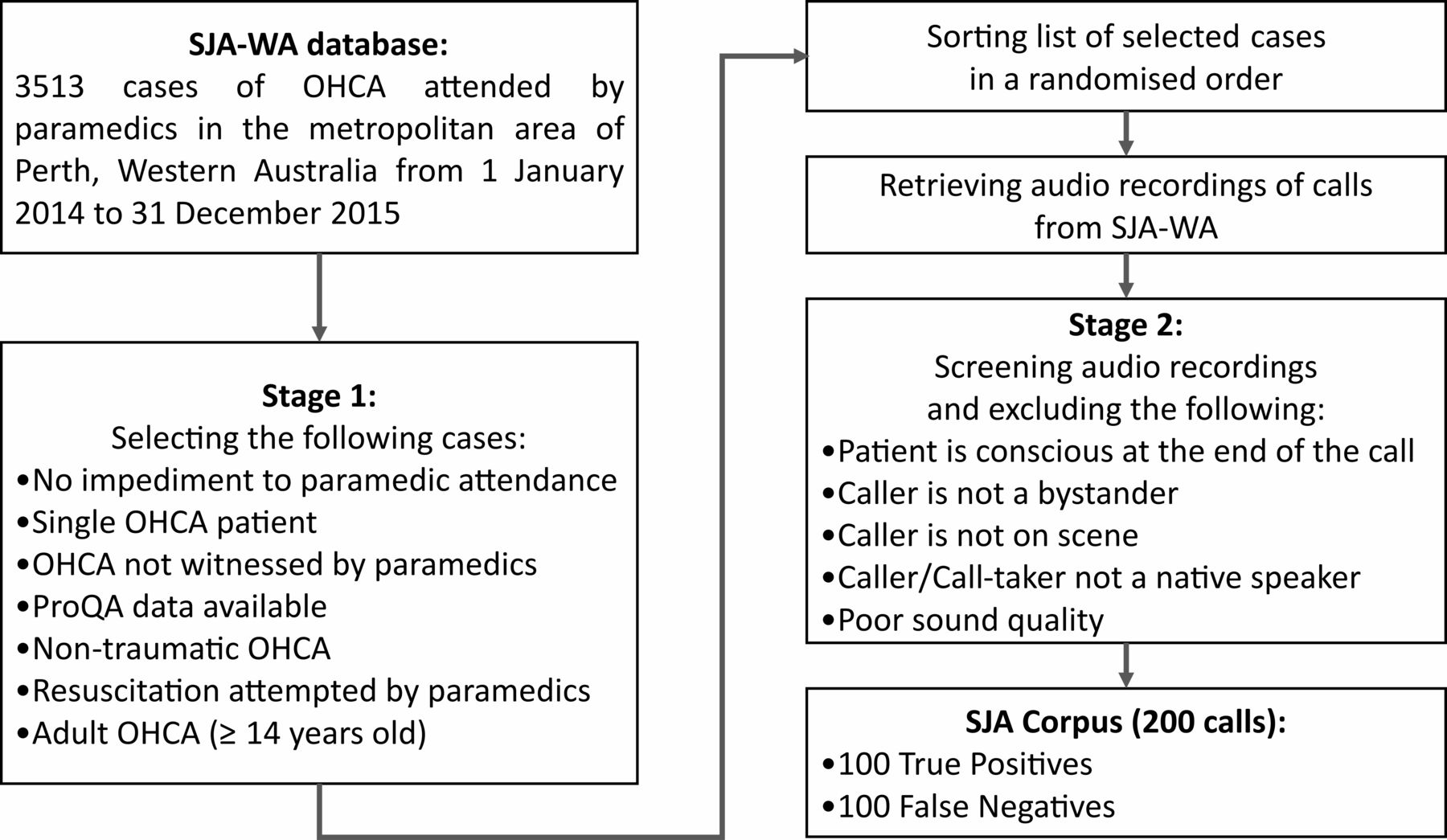
The study will combine two types of data: the content of the calls (in the form of transcribed audio recordings, ie, the corpus) and the dispatch data attached to each case (metadata retrieved from the EMS). The corpus (‘SJA Corpus’) will consist of emergency telephone calls concerning OHCA occurring in the Perth metropolitan area and processed at the call centre of St John Ambulance Western Australia (SJA-WA) between 1 January 2014 and 31 December 2015. SJA-WA uses the standardised protocol MPDS, implemented with the ProQA software.54 The SJA-WA OHCA database, maintained by the Prehospital, Resuscitation & Emergency Care Research Unit (PRECRU) at Curtin University, contains all cases of OHCA (paramedic-verified resuscitations and out-of-hospital deaths) in Perth, Western Australia since 1996. For the study period, there were 3513 OHCA cases attended by SJA-WA paramedics in the metropolitan area. An electronic copy of all incoming calls is stored by SJA-WA on a secure server as well as their corresponding ProQA data, listing all the information and steps entered by the call-taker in the dispatch system. Because of the time-consuming character of the transcription and qualitative analysis of audio data, the study will not analyse all the 3513 calls. A random sample of calls (minimum of 200 calls), including at least 100 calls in which OHCA was recognised by the call-taker (True Positives) and 100 calls in which OHCA was not identified at the time of the call (False Negatives), will be selected. We estimate that a sample size of 200 is suitable both for the qualitative and quantitative components of this mixed-methods study protocol.
Our definition of OHCA recognition originates from our previous study on OHCA recognition in Perth (submitted for publication, under peer review). We will consider that OHCA is recognised at dispatch in the presence of at least one of the following elements:
The dispatch code assigned by the call-taker indicates cardiac arrest.
MPDS protocol steps for CPR were taken by the call-taker, as evidenced by an electronic search for the words ‘CPR’ and ‘RESUS’ in the Computer-Aided Dispatch data.
Two priority 1 paramedic-staffed ambulances were dispatched, as SJA-WA reserves dual response to cardiac arrest.
There will be two stages to data collection, as illustrated in figure 2. In the first stage, we will select cases from the SJA-WA OHCA database which meet these criteria: no impediment to paramedic attendance (eg, patient not on aeroplane), incidents with a single OHCA patient, OHCA not witnessed by paramedics, cases for which ProQA data are available, non-traumatic OHCA, cases for which the paramedics attempted resuscitation and adult OHCA (≥14 years old).55 Second, the cases which meet the selection criteria in stage 1 will be sorted in a randomised order (using a random number generator). We will work through this list of randomised cases sequentially until we have reached the target of 200 calls. The call audio for these cases will be retrieved from the SJA-WA call centre (Belmont, Western Australia). We will listen to calls on a one-by-one basis and exclude the following: cases in which the patient is unequivocally conscious at the end of the call (as evidenced through their voice being audible during the call), calls in which the caller is not a lay bystander (eg, police officer), the caller is not on scene (relaying message third-party), the caller and/or call-taker is not a native speaker of English (determined by auditory assessment) and calls for which the sound quality is too poor to allow for acoustic analysis (eg, disruptive loud background noise throughout the call, saturated signal).
{kind=link}
{kind=link}
Summary of data collection.
Some of these criteria, though often used in the literature, require further justification. We will first discuss the criteria used to select cases from the SJA-WA OHCA database, and then review the exclusion criteria that we will use when screening the audio recordings.
Some studies on OHCA dispatch choose to exclude cases of obvious deaths14 or patients who were declared dead on arrival of paramedics.10 While such an exclusion criterion is rarely justified explicitly, we interpret it in light of previous findings showing that the population which would benefit the most from high priority response and resuscitation attempt are also the cases which are the most difficult to identify during dispatch.11 From the point of view of dispatch research, we find it analytically justifiable to focus on calls for which OHCA recognition is a real issue as the call unfolds. Patients who have obviously been deceased for several hours or days pose less issues of response time and recognition during dispatch. However, instead of using ‘obvious death’ as an exclusion criteria, we will only include cases for which resuscitation was attempted by paramedics,9–11 14 as recommended in a recent systematic review on OHCA recognition.6
Similarly, trauma is an exclusion criteria commonly found in the literature. A number of recent studies excluded OHCA cases presumably caused by trauma.9 10 12 14–17 OHCA from trauma has different clinical implications from OHCA with cardiac origin and lower survival rates.56 The issue of recognition during dispatch is also quite different. In the case of traumatic OHCA, the nature of the emergency tends to be more obvious and more readily describable by bystanders (eg, “someone’s fallen off the cliff”). Also, the MPDS dispatch code assigned to the case is not necessarily expected to correspond to cardiac arrest, but rather to the trauma itself (eg, ‘17D01’ for extreme fall). As was mentioned above regarding cases of obvious deaths, excluding cases of traumatic OHCA allows the study to focus on the group of patients which could benefit the most from faster recognition and dispatch. Trauma patients are much more likely to be readily identified as life-and-death emergencies at the time of dispatch. More opportunity for improvement lies in non-traumatic OHCA, which is much more difficult to identify during dispatch.11
We will exclude paediatric OHCA for two reasons. The first reason is to facilitate comparison with other studies which focused on emergency calls for adult OHCA.11 12 15 17 The second reason is that basic life-saving instructions are adapted to the age of the patient. For example, when callers are given instructions for chest compressions, they are asked to place their two hands (for an adult), only one hand (for a child) or the fingers of only one hand (for an infant) on the chest of the patient. As our study protocol focuses on the language used in OHCA calls, we will exclude paediatric OHCA because it involves variations in the script protocol which would not allow for comparison between calls. We will use the age limit of 14 years old to define paediatric OHCA as per the Clinical Practice Guidelines of SJA-WA.55
Calls in which the patient is unequivocally conscious at the end of the call (as indicated by hearing their voice) provide sufficient evidence that the cardiac arrest has not happened at the time of the call. While it is possible that such patients may subsequently suffer from a cardiac arrest and need urgent care, from the point of view of dispatch, it is unreasonable to expect call-takers to identify them as cases of cardiac arrest at the time of the call. The reason for this exclusion criterion is not just medical but also interactional, as it is of paramount importance to analyse interaction as it unfolds in real time, without using subsequent information to which the speakers involved did not have access.57
In a similar way to previous studies,10–12 16 we will restrict our focus to calls made by bystanders, or in more sociological terms, callers acting as ordinary members of society or laypersons. This means excluding calls made by the police or staff from nursing homes, retirement villages or health facilities as well as monitoring companies (eg, for patients who have a medical alert system). The role of the caller, rather than location, is the defining criterion. Hence, a call made by the manager of a retirement village for a resident will be excluded, while a call coming from the partner of a resident in a retirement village will be included. However, this does not exclude cases in which the caller is related to the patient but happens otherwise to be a health professional, as such callers do not tend to frame the call as a ‘professional to professional’ call, but rather as an institutional encounter involving an ordinary member of society and an institutional representative.58 59
We will exclude calls in which the caller is not on scene, that is, the caller is not in close proximity to the patient and is consequently unable to assess their status.10 11 15 In linguistic terms, this corresponds to direct epistemic access, that is, knowledge that callers acquired themselves (they can see, hear and/or feel the patient) rather than indirectly, such as being told about the patient’s condition by someone else. Differences in epistemic access have been shown to impact the way speakers talk,60–62 and analysing how this factors into emergency calls warrants further inquiry in the future.
The focus on native speakers of English is a standard one in the discipline of linguistics, where the study of English as a native language or as a second language involves starkly different issues and methods. Including non-native speakers would engender interferences and transfers between languages63 which could not be reasonably accounted for. The native status of speakers will be assessed aurally and through consensus in cases for which there is any doubt. We will not exclude bilingual speakers (native speakers of English plus another language) or speakers of other varieties than Australian English (eg, South African English and American English).
Transcription
The corpus will be transcribed following the revised system devised by Jefferson for CA.64 65 This involves a fine-grained level of details aimed at representing various dimensions of speech, such as intonation, tempo, pauses, false-starts and hesitations and overlap between speakers. The now well-established conversation-analytic method has shown that such minute variations carry crucial meaning and are highly relevant to how speakers interact.
We will use the transcription software CLAN66 which will make it possible to maintain a time-alignment between the transcript and the audio files. This method recognises that the primary data are the audio files, while the transcripts are a partial—but necessary—representation of the interaction between caller and call-taker.67 The transcripts will be reviewed independently for accuracy.
Sequential analysis
The first step of analysis will be sequential analysis, a method developed by CA to study spoken language. CA is an inductive qualitative method whose focus is the fine-grained orderliness that structures social interaction.25 26 68 The main assumption of CA is that interaction is structured at a minute level of detail and is shaped by the actions and the interactional projects that participants implement and actively orient to as relevant to them, in situ. The analytical effort focuses on identifying the ‘tying’ structures of the calls, that is, how each turn is occasioned by the preceding turns and what type of turn it projects next. The key analytic question is the famous ‘why that now?’,69 based on the assumption that spontaneous interaction is characterised by ‘order at all points’24 and that speakers are aware of—and react to—subtle variations in content and structure. One of the central tenets of CA is that the analyst should look for structures and formats that participants rely on and orient to, and that nothing should be dismissed as trivial without further investigation. Interactions are studied as they unfold turn-by-turn, focusing on the temporal development experienced by participants themselves. This method is essentially qualitative in nature; however, it can be conducted in such a way as to make quantitative analysis possible—even though such a practice remains non-canonical in the field of CA.70 71
Prosodic analysis
Prosodic analysis will be conducted where relevant. The term ‘prosody’ describes the different variations in pronunciation contributing to the specific melody with which an utterance is said. This includes a certain intonation (eg, rising or falling intonation), speech rate (slow or fast tempo, pauses and silences) and loudness (low or loud voice).72–74 We will use a combination of auditory as well as instrumental analysis, using the speech analysis software Praat,75 and focusing in particular on variations of pitch (pitch contour and pitch register).
Systematic coding
Using a coding spreadsheet, linguistic and interactional features will be operationalised as coding categories and potential variables for statistical analysis. This technique was developed for speech data by the field of Corpus Linguistics.51 52 Linguistic analysis of the calls will strive to identify usage-features bearing on the interactional success and appropriate dispatch. Such usage-features can consist in variations in linguistic structure (eg, using a declarative vs interrogative format, rising vs falling intonation) or interactional variables (eg, relationship of the caller to the patient, age of the caller). Each category will include a specific code for unclear or unknown cases (eg, if part of a sentence cannot be heard clearly because the caller and call-taker speak at the same time). This approach is quantitative but goes hand-in-hand with careful qualitative analysis at each stage of the research: initially to determine which features are of interest and how to analyse them, then during the process of manual coding and at the final stage of result interpretation.
Quantitative analysis
Quantitative analyses will involve a combination of descriptive statistics and statistical tests. For descriptive statistics, we will calculate the frequency of different linguistic choices made by the call-taker (eg, choice of tense, as in ‘what’s happened?’ vs ‘what happened?’) and by the caller (eg, responding in narrative vs report format). We will use two indices to assess quality of dispatch: efficiency and accuracy. Regarding efficiency, we will measure the time taken to complete steps of the call-taking process (summarised as medians and IQRs), for example, time to assess the patient’s breathing. Accuracy will be analysed through the prism of OHCA recognition (as defined above in the ‘Data collection’ section). Where relevant (where a causal relationship is plausible), statistical analyses will be used to measure the associations between different linguistic features of the calls, using logistic regression, χ2 or the Mann-Whitney test (depending on the format of the data as categorical or continuous), using the statistical software R.76 In terms of predictors, we will focus on modifiable aspects of the way call-takers ask questions or deliver prompts. For outcome variables, we will focus primarily on proximate (immediate) aspects of the caller’s response. As secondary outcome variables, we will examine aspects of call progression such as time to EMS dispatch and recognition of OHCA. Due to the inductive and data-driven nature of this research, all statistical tests should be considered post hoc as part of a process of hypothesis-generation rather than a priori hypothesis-testing.
Discussion
The main strength of our protocol is its interdisciplinary approach, as it seeks to answer questions crucial to emergency ambulance dispatch and emergency care, using the methods of linguistics, social sciences and health sciences. The mixed-methods component of this research also means that the data will be investigated from different and yet complementary angles. This novel approach to studying OHCA will provide a deeper understanding of interactional factors impacting on the accuracy and timeliness of ambulance dispatch.
This research will focus on emergency calls in which English is the only language used by call-takers to address callers. Consequently, our findings might not be applicable to other languages. Besides, environments in which English is not the sole official language pose unique challenges for emergency calls, as was shown by a recent study on switching between English, Afrikaans and isiXhosa in a South African call centre.77 Thus, one limitation of this research is that it will not take into account non-English and multilingual contexts. Another important limitation is the focus on one dispatch protocol, namely the MPDS. Further research will be needed to determine the relevance of findings to other protocols and guidelines, such as Criteria-Based Dispatch.78
This research will translate into applied outcomes. The management of OHCA calls at dispatch will be improved by the insights about the early recognition of OHCA gained from this research. Furthermore, the research will inform more efficient delivery of instructions to bystanders, such as dispatcher-assisted CPR. It will generate evidence-based recommendations for modifications of the MPDS algorithm for ambulance dispatch, and more generally for call-centres in which dispatch is conducted in English. We envisage that the results of this research could also translate into reduced ambulance response time for OHCA, as undetected or unresolved communication issues can create considerable delays. And finally, a better understanding of OHCA calls in general could have applications for the training of call-takers, specifically targeting the interactional component of emergency ambulance calls.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
Footnotes
Contributors JF is the scientific coordinator of the study. The SJA-WA OHCA database is maintained by MI. AW contributed to the acquisition of data. The study objectives were defined by JF, PB, AW, DB, JB, GDP, PC, DMF, KS, TAW, SB, MI, KLOH and PD. The study was designed by MR, JF and SB. MR drafted the manuscript and JF, SB, TAW, KOH, JB, DMF, PC, GDP and MI reviewed and provided comments to improve the paper. All authors have read and approved the final version.
Funding This work has been supported by an NHMRC Partnership Project between Curtin University and St John Ambulance Western Australia (APP1076949 ‘Improving ambulance dispatch to time-critical emergencies’).
Competing interests JF is the Director of the Australian Resuscitation Outcomes Consortium (Aus-ROC). JF, MI and JB receive partial salary support from the NHMRC Aus-ROC Centre of Research Excellence #1029983. MR receives full salary support from the NHMRC Partnership Project #1076949. AW and DB received full salary support and JF, PB and MI received partial salary support from St John Ambulance Western Australia. Other authors have no competing interests to decline.
Ethics approval Curtin University Human Research Ethics Committee (HR128/2013) and SJA-WA Research Advisory Group.
Provenance and peer review Not commissioned; externally peer reviewed.