Article Text

Abstract
Introduction Osteoarthritis (OA) is the leading cause of disability and pain in older adults. Although increasing physical activity (PA) can help reduce symptoms, patients with lower-limb OA are less active than the general public. Although physiotherapists commonly deliver PA programmes, they lack knowledge of key barriers and facilitators to adherence to prescribed PA that patients with lower-limb OA experience while attending physiotherapy appointments (treatment period) and after discharge (post-treatment period). This study aims to explore the perspectives of patients with lower-limb OA of barriers and facilitators to adherence to physiotherapy prescribed PA in the treatment and post-treatment time periods to inform the development of intervention underpinned by behaviour change theory.
Methods and analysis A qualitative study, based on phenomenology, will purposively recruit patients with lower-limb OA who have had physiotherapy. In-depth semi-structured interviews will be undertaken following discharge from physiotherapy at a single time point. Participants’ perspectives of physiotherapy interventions, including barriers and facilitators to prescribed PA and techniques that they felt optimised adherence to physiotherapist PA prescription will be explored (phase I). The acceptability and feasibility of delivering a physiotherapy intervention incorporating the techniques identified in the semi-structured interviews will then be explored through focus groups conducted with physiotherapists (phase II). Data will be coded following thematic analysis, with barriers and facilitators mapped to the constructs on the theoretical domains framework, and behaviour change techniques identified following definitions from Michie’s V1 taxonomy.
Ethics and dissemination Findings from this study will inform development of a physiotherapy intervention underpinned by behaviour change theory aiming to optimise adherence to PA prescription in patients with lower-limb OA during the treatment and post-treatment time periods. This study has ethical approval (IRAS 247904) and results will be disseminated through publications in peer-reviewed journals and presentations at conferences and to study participants.
- osteoarthritis
- qualitative study
- behaviour change
- physical activity
- adherence
- physiotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This qualitative study is the first to seek an in-depth understanding of the barriers and facilitators to adherence to physiotherapy prescribed physicalactivity in both treatment and post-treatment time periods in patients with lower-limb osteoarthritis (OA).
Patient and public involvement has been utilised in the design of the study and will inform data analysis ensuring that the perspectives of patients with lower-limb OA is captured throughout the study.
Seeking the opinion of physiotherapists who currently treat patients with lower-limb OA on the acceptability and feasibility of delivering a pilot intervention enhances the clinical applicability of the study.
This study has a relatively small sample size and excluding patients with lower-limb OA who do not speak English or who not attended physiotherapy will further limit its generalisability and applicability.
INTRODUCTION
In the UK, osteoarthritis (OA) is the leading cause of individual level disability and the most common cause of pain in older adults1 with one-third of patients over 45 years old, equating to almost 9 million individuals, having sought treatment for OA related symptoms.2 Lower-limb OA is particularly problematic in the UK, with 4.1 and 2.5 million individuals experiencing knee and hip OA related symptoms, respectively.3
Physical activity (PA), incorporating both structured exercise and broader concepts such as leisure activities, is advocated by international healthcare guidelines and is used extensively as part of non-surgical management of lower-limb OA-related symptoms.4 However, patients with lower-limb OA have reduced PA levels compared with the general population5 and interventions incorporating PA strategies generally only facilitate short-term management of pain and function.6 7 This short-term time frame generally corresponds to when the patient is attending sessions under the supervision of a healthcare professional (eg, a physiotherapist) and doing prescribed PA away from the clinic as part of the treatment regime (treatment-period). The primary reason for decreased long-term effectiveness of PA interventions is related to reduced adherence to PA prescription from patients with lower-limb OA8–10 when they are required to maintain their prescribed PA independent of input from the healthcare professional (post-treatment period).
The behaviour change literature outlines that learning and consolidating new behaviours, such as PA, requires individuals to go through several phases of behaviour change including initiation11–13 or adoption14 15 and maintenance.12–17 It is likely that most treatment periods occur during the ‘adoption’ phase,16 when the individual would be learning new habits and techniques to enhance their PA levels. The post-treatment period would coincide with the ‘maintenance’ phase,17 where the individual consolidates their PA behaviours. The skills required to maintain a behaviour are distinct from those that enables an individual to adopt it16 17 and a healthcare intervention aimed at optimising adherence to PA likely requires unique techniques that match the changing needs of its target patients. This may in part explain the drop off in effectiveness in clinical outcomes during the post-treatment phase.
The Medical Research Council advocates that interventions that alter participant behaviours (such as PA) should be underpinned by behaviour change theory18 as they are thought to be more effective than non-theoretical interventions and specific determinants of behaviour can be tested with subsequent refinement of the intervention.19 However, few intervention studies exist that are underpinned by behaviour change theory.19
Physiotherapists are the primary healthcare professionals responsible for providing PA prescription in the National Health Service (NHS),20 and well placed to provide PA interventions to patients with lower-limb OA.21 Although physiotherapists believe that they have the necessary skills to promote PA,22 recent systematic review evidence suggested that physiotherapists do not possess the requisite knowledge of behavioural theories or techniques to apply them effectively in their clinical practice.23
The theoretical domains framework (TDF) synthesises different theories of behaviour change into one framework and enables the mapping of barriers and facilitators against theoretically derived domains that influence patient behaviour.24 The original TDF24 has been validated and updated to include 14 domains incorporating 84 theoretical constructs.25 The domains include knowledge, skills, social/professional role and identity, beliefs about capabilities, optimism, beliefs about consequences, reinforcement, intentions, goals, memory, attention and decision processes, environmental context and resources, social influences, emotion and behavioural regulation.25 The TDF has been used extensively in the behaviour change literature with over 800 citations in peer-reviewed journals.26
Interventions underpinned by behaviour change theory can be developed by identifying behavioural techniques relevant to the TDF domains.27 Behaviour change techniques (BCTs) are the theoretically derived, active components found within behaviour change interventions.28 Michie et al28(p82) define a BCT as ‘an observable, replicable and irreducible component of an intervention designed to alter or redirect causal processes that regulate behaviour’ and include techniques such as ‘reinforcement’, ‘self-monitoring’ and ‘feedback’. The taxonomy contains 93 distinct BCTs grouped into 16 hierarchies28 and has been used extensively in the literature.29 Our recent systematic review (Willett et al, under review) of randomised controlled trials examining the effectiveness of BCTs used in physiotherapy interventions to optimise adherence to prescribed in patients with lower-limb OA identified the BCTs ‘behavioural contract’, ‘non-specific reward’, ‘goal setting (behaviour)’, ‘self-monitoring of behaviour’ and ‘social support (unspecified)’ as effective at optimising adherence to prescribed PA across all measured time points (from ≤3 to ≥12 months postbaseline). The results also suggested that certain BCTs may be more useful during the treatment period (eg, ‘action planning’) while others more effective during the post-treatment periods (eg, ‘graded tasks’ and ‘problem solving’). However, the overall effectiveness of these BCTs was modest and based on results from RCTs graded as medium-high risk of bias and with poor intervention reporting. Therefore, further research is needed to verify and expand on these results.
To develop a physiotherapy intervention aimed at optimising adherence to prescribed PA that is underpinned by behaviour change theory and incorporates the most appropriate BCTs, key barriers and facilitators that patients face need to be identified. Barriers and facilitators to adherence to prescribed PA in patients with lower-limb OA have been outlined in the literature and include fear of pain with movement, reduced motivation for PA engagement and limited access to facilities to promote PA.30 31 However, only one study32 has identified determinants at a specified point in the behaviour change process and this study focused exclusively on PA maintenance. No research to date has sought to gain an in-depth understanding of patients with lower-limb OAs’ perceptions of barriers and facilitators to physiotherapist prescribed PA during both the treatment and post-treatment timeframes or identified the most important BCTs to include as part of a physiotherapy programme aimed at optimising PA adherence. Furthermore, no research has examined the perspectives of physiotherapists on whether a pilot intervention that is underpinned by behavioural theory and includes BCTs which have been identified by patients with lower-limb OA as important at optimising PA in the treatment and post-treatment time periods would be acceptable and feasible to be delivered consistently in their clinical setting.
Aims
The studies aim is to explore the perspectives of patients with lower-limb OA of barriers and facilitators to adherence to physiotherapy prescribed PA in the treatment and post-treatment time periods to inform the development of intervention underpinned by behaviour change theory.
Objectives
Phase I
To explore patients’ perceptions of barriers and facilitators to adherence to PA prescribed within physiotherapy sessions during the treatment and post-treatment time period.
To identify which BCTs patients with lower-limb OA perceive to be most important to include in a physiotherapy programme aimed to optimise adherence to prescribed PA in the treatment and post-treatment period.
Phase II
To determine physiotherapists’ perspectives on the feasibility and acceptability of incorporating the identified BCTs into a real-world pilot physiotherapy intervention.
METHODS AND ANALYSIS
Research team and reflexivity
Phase I
The semi-structured interviews will be undertaken by the lead researcher (MW), an advanced practice physiotherapist with over 15 years of experience in managing patients with lower-limb OA. Although no specific relationship will be established prior to the commencement of the interviews, MW will outline that the interviews are part of a programme of research that intends to develop a physiotherapy intervention aiming to promote adherence to prescribed PA in patients with lower-limb OA. The participants will be informed of MW’s professional background to ensure full disclosure but will be assured that MW is there as a researcher rather than a clinician.
Phase II
The focus groups will be led by the chief investigator (AR), an experienced musculoskeletal physiotherapist who has a PhD and extensive experience conducting qualitative research; with MW as the observer who will record who is speaking at each time point and participants’ reactions. AR will be familiar to many of the participating physiotherapists. The focus group participants will be told that the study forms part of a programme of research and that it will be used to develop a physiotherapy intervention based on behaviour change theory that seeks to optimise adherence to PA prescription during the treatment and post-treatment period in patients with lower-limb OA.
Study design
Theoretical framework
Patient perspectives are integral to determining the effectiveness of complex clinical interventions33 and qualitative research is becoming more influential in NHS guidelines for clinical practice.34 As the perspectives of patients and physiotherapists are central to developing an intervention35 and an in-depth understanding is sought,36 this qualitative study is based on a phenomenological framework. This study is designed and will be reported in line with the Consolidated Criteria for Reporting Qualitative Studies.37
Participant selection and setting
Phase I
Adults (≥18 years) with a diagnosis of unilateral or bilateral lower-limb OA who are attending physiotherapy at one site (The Royal Orthopaedic Hospital NHS Trust, Birmingham, UK) will be invited to take part in a single one-to-one, semi-structured interview (figure 1). Diagnosis of OA can be through self-report of symptoms (≥45 years old, activity-related joint pain and morning stiffness ≤30 min duration) as per National Institute for Health and Care Excellence (NICE) guidelines or imaging.1 Participants are required to be able and willing to give informed consent, and able to communicate fluently in English. Patients who have coexisting articular pathology effecting their hip or knees for example, gout, ankle arthritis, rheumatoid arthritis, have had or on a waiting list for hip or knee joint replacement, or are wheelchair dependent/have an inability to transfer will be excluded.
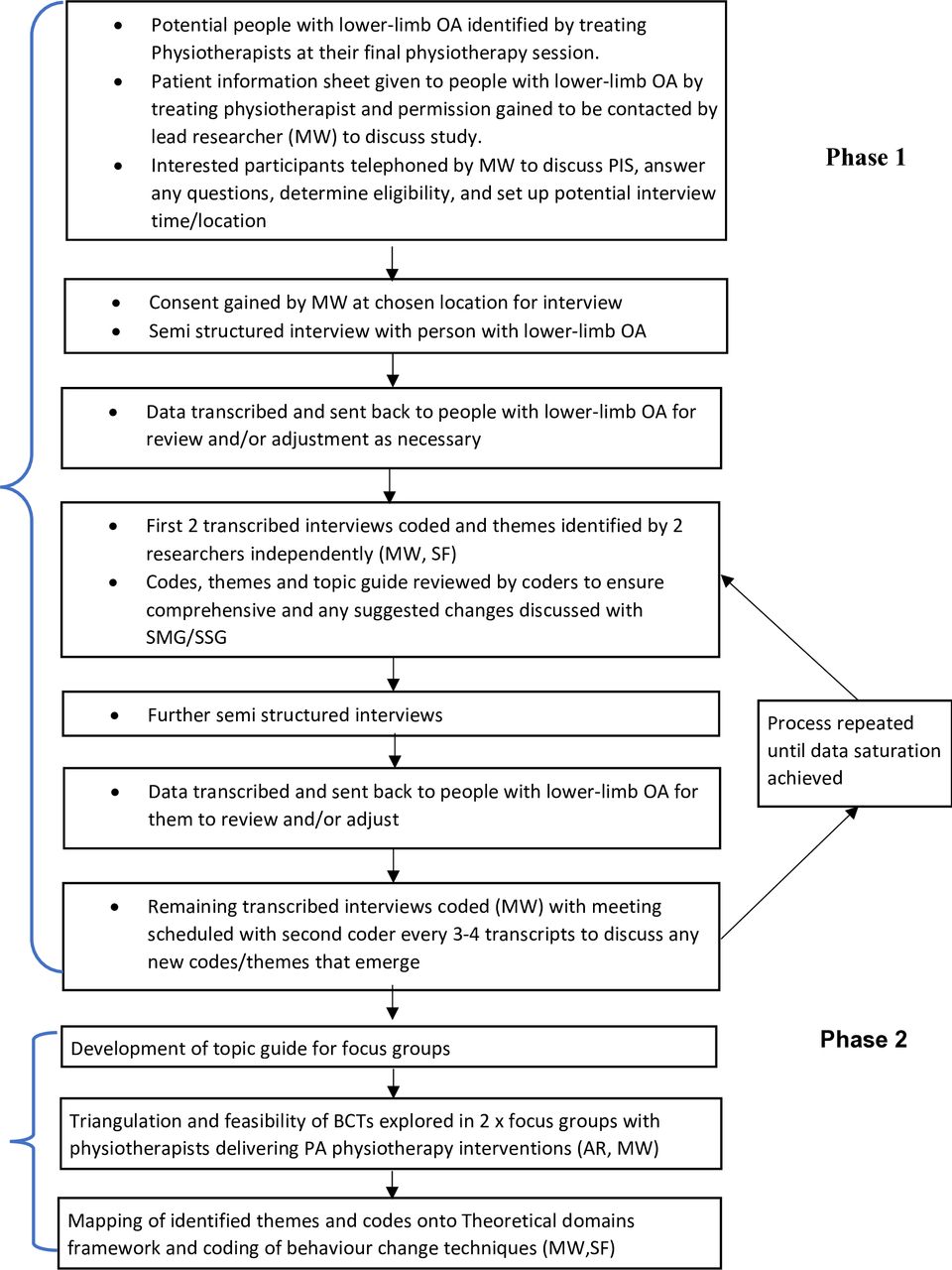
{kind=link}
Study flowchart. BCTs,behaviour change techniques; OA, osteoarthritis; SMG,Study Management Group; SSG, Study Steering Group.
Consenting participants will be offered a choice of having their interview at their home or at the Royal Orthopaedic Hospital or the University of Birmingham. Purposive sampling will be used gain a wide variety of opinions and recruitment will continue until data saturation has been reached (minimum of 10 participants) which is defined by no additional themes emerging from the analysis38 (please see figure 1 for detail). In the UK, ~60% of patients with lower-limb OA have knee OA39 and 60% are females. Therefore, initially stratified purposive sampling will target participants based on these ratios.40 The initial purposive sampling framework is outlined in table 1. As sampling progresses, theoretical purposive sampling will be utilised to target key secondary factors to ensure that those who work/do not work and those from different ethnic and educational backgrounds are also captured within the sample.41
Purposive sampling framework target
The site lead researcher (DR), who is an advanced physiotherapy practitioner within the trust, will outline the study to physiotherapists who treat patients with lower-limb OA at the Royal Orthopaedic Hospital. Participants will then be identified by their treating physiotherapist and the study will be outlined with them at their final physiotherapy appointment. If they show interest in the study, the patient with lower-limb OA will be given a participant information sheet (PIS), and consent to contact will be sought for the lead investigator (MW) to contact them by telephone. Potential participants will then be contacted by telephone ~1 week after the date of their final appointment, so they have time to think about the study and consult with family and friends. During the telephone call, MW will confirm eligibility, discuss the participant information sheet and answer any questions about the study before arranging a time and location for the interview.
Phase II
Physiotherapists who have delivered PA interventions for patients with lower-limb OA within the last 6 months at the Royal Orthopaedic Hospital will be eligible to participate. The site lead researcher (DR), will use convenience sampling to approach and recruit the physiotherapists in person. Focus groups will be conducted at the Royal Orthopaedic Hospital for pragmatic reasons, time commitments and convenience of the clinicians. There are ~16 physiotherapists who regularly treat patients with lower-limb OA, therefore, it is anticipated that 2 focus groups will be conducted (based on 6–8 in each group). The total number of physiotherapists approached compared with those who attended the focus groups will be recorded.
Data collection
Phase I
Semi-structured interviews were chosen for the phase I data collection to enable patients with lower-limb OA to go into great depth when discussing their perceptions of PA,42 to provide a rich account of their perspectives, while allowing for flexibility with-in the session.43 Questions will initially be asked in an open manner with prompts given or clarification sought if key points are identified with participants encouraged to identify new ideas during the interview. The topic guide (please see online supplementary appendices for the phase I topic guide) has been developed by including perspectives of patients with lower-limb OA (through patient and public involvement), and incorporating systematic review data, contemporary interview research,31 43–45 and surveys exploring perspectives46 of patients with lower-limb OA. The guide includes questions regarding a participant’s current PA, their perspectives of physiotherapy interventions including barriers and facilitators to (objective 1), and BCTs they believe would optimise (objective 2), adherence to physiotherapist PA prescription during the treatment and post-treatment time periods. Demographic data including participants gender, age, Body Mass Index (BMI), ethnicity, educational level, length of time since OA diagnosed and the number of times they have been referred for referred to physiotherapy for management of their lower-limb OA symptoms will be collected. Further detail on participants functional level (Short-form Knee Injury and Osteoarthritis Outcome Score47 48)/Hip Injury and Osteoarthritis Outcome Score47 49 and PA (3-day physical activity recall interview50 51) will be collected as part of the interviews. MW will take supplementary field notes during the interview process to enable triangulation during data analysis. Interviews will be audio recorded and transcribed verbatim and are anticipated to last ~60 min. Repeat interviews will not be conducted but the transcripts will be posted or emailed to participants (according to their preference) for member checking. Any adjustments or additional comments which arise from member checking, including contradictory statements, will not be included in the main data analysis but will be presented to the study steering and management groups when presenting the emerging themes to challenge the robustness of the barriers and facilitators identified. The member checking will also be used to verify approval of quotations to use in the final write up.52 The topic guide will be pilot tested prior to use with members of the Centre for Precision Rehabilitation Spine’s Patient and Public Involvement Group at the University of Birmingham who have lower-limb OA and are not be part of the main study. The topic guide can be found in the online supplementary appendices.
Analysis and findings
Data analysis and reporting
Development of the pilot physiotherapy intervention
The pilot physiotherapy intervention will follow a modified version of the guidance outlined by French et al53 to develop complex interventions which are underpinned by behaviour change theory.
Identification of barriers and facilitators
Data from the semi-structured interviews and focus groups will be analysed inductively following the six stages from Braun and Clarke.54
Familiarise yourself with the data.
Generate initial codes: coding for as many patterns as possible with surrounding words included to maximise contextual factors
Searching for themes: sort codes into potential themes.
Reviewing themes.
Defining and naming themes.
Producing the report.
This is an established method,26 having been utilised extensively in qualitative studies, and enables flexibility54 to analyse the research topic while developing unexpected themes that emerge from the transcripts during coding.55 The first transcript from the semi-structured interview will be coded by two researchers (MW, SF who has expertise in behaviour change) in tandem to develop a coding strategy with the second transcript used to ensure the researchers are comfortable with the coding.56 The remaining semi-structured interviews will be coded independently by MW and the coders will meet every 2–3 semi-structured interviews to review any new codes and themes that emerge from the transcripts and emerging themes will be presented to the Study Steering Group (SSG) to iteratively discuss any emerging themes. The coders will actively read the entire transcription before beginning to code the data and will attempt to suspend any presuppositions. To enable transparency within the audit trail, NVivo software will be used to store information and coders will keep a reflexive journal to identify their initial thoughts and perceptions.
To identify the most important themes to target in the developing intervention, the coders will pay specific attention to57:
High frequency of specific beliefs and/or themes.
Presence of conflicting beliefs.
Strongly emphasised beliefs that may affect adherence to physiotherapy prescribed PA.
Quotations from participants will be presented to highlight key themes (participants will be identified with an assigned code) that emerge from the thematic analysis, with major and minor themes clearly delineated in the study report. Finally, the themes will be categorised as barriers or facilitators to adherence to physiotherapy prescribed PA in the treatment and post-treatment period. The barriers and facilitators will then be mapped onto relevant domains of the TDF25 27 by the same two researchers who conducted the thematic analysis.
Identification of BCTs to overcome barriers and aid facilitators
BCTs (from the BCT taxonomy)28 will be coded from the identified domains on the TDF by the same two researchers following established guidelines.27 58 Important and priority BCTs will be related to the barriers and facilitators from which they were coded based on the criteria outlined in the thematic analysis (ie, frequency, presence of conflicting opinions and those that are strongly emphasised). The phase I topic guide (please see online supplementary appendices) is divided into treatment and post-treatment time frames to enable sequencing of BCTs. The timing and means of delivery of the BCTs will be further informed by reviewing the interventions from the low risk of bias RCTs (identified in our systematic review) which demonstrated effect of adherence to prescribed PA.
Phase II
The pilot physiotherapy intervention will then be explored in focus groups (objective 3) (figure 1). The focus group topic guide will seek the physiotherapists’ perspectives on the structure and content of the pilot intervention including its acceptability, feasibility and practicality (capability, opportunity, challenges to delivery)45 and the incorporated BCTs. The focus groups will be used to maximise insight of physiotherapist perspectives through an interactive group process providing multiple perspectives.26 This will enable physiotherapists to propose and, through challenging and adding to others’ points,59 to articulate logistical issues around implementation of the outlined physiotherapy intervention within their trust that are not apparent to the researchers.60 Prior to the focus group, basic demographic data will be recorded from the participating physiotherapists (gender, age, total time in clinical practice since graduation and amount specifically treating patients with lower-limb OA, their level of education, frequency treating patients with lower-limb OA, and how often they use strategies to target adherence to prescribed PA and their perceived effectiveness during the treatment and post-treatment time periods). Each focus group is anticipated to last ~90 min and the discussion will be audiotaped and transcribed verbatim, with the transcripts emailed to participating physiotherapists to enable further review and feedback. Please see online supplementary appendices for the phase II topic guide. Data from the focus groups will be analysed following the same processes by the same two researchers as the semi-structured interviews from phase I.
Implications of results
The BCTs and key barriers and facilitators identified from the semi-structured interviews will be synthesised to develop a pilot physiotherapy intervention aimed at optimising adherence to physiotherapy prescribed PA in patients with lower-limb OA. The focus groups will enable the feasibility and acceptability of delivering the identified BCTs as part of an intervention to be determined and enhance it clinical applicability. Comparison of the findings with our systematic review (Willett et al, under review) will enable incorporation of the most effective BCTs identified across both research projects to develop the physiotherapy intervention for a proposed pilot and feasibility study.
Patient and public involvement
This study is informed by suggestions made by a patient with lower-limb OA who is an integral member of the research team (member of both Study Management Group (SMG) and SSG). This has ensured that their perspective has contributed to the development of the phase I interview topic guide, participation information sheet and consent forms, and will further inform the data analysis and production of a lay summary of findings for dissemination. Members of the Centre for Precision Rehabilitation Spine Patient and Public Involvement group will be used to pilot the phase I topic guide.
LIMITATIONS
The lead investigator, who will conduct the interviews, code transcript data for themes, identify barriers and facilitators, and code BCTs is a musculoskeletal physiotherapist with extensive experience with patients with lower-limb OA. Therefore, it will be problematic to remove all presuppositions and some researcher bias is expected. As this study focuses on patients with lower-limb OA who have already attended physiotherapy, it will not identify barriers that patients with lower-limb OA who are invited but do not attend physiotherapy sessions experience. Therefore, specific BCTs that could facilitate patients with lower-limb OA attending physiotherapy will not be identified and could be explored in future studies.
Furthermore, this study also has a relatively small sample size and excluding patients with lower-limb OA who do not speak English will further limit its generalisability and applicability.
ETHICS AND DISSEMINATION
Research governance
The study will be conducted in accordance with the principles of the Research Governance Framework for Health and Social Care. The study protocol (IRAS 247904) has received Health Research Authority and site confirmation of capacity and capability approval, and a favourable opinion has been given by a research ethics committee (18/WM/0363). Pseudonymised participant data will be stored confidentially for 10 years in the protected REDCap data storage system in the Centre for Precision Rehabilitation of Spinal Pain at the School of Sport and Exercise, Rehabilitation Sciences, at the University of Birmingham, in accordance with General Data Protection Regulation (GDPR) and the Data Protection Act 2018 and University of Birmingham’s research governance frameworks. The study will be coordinated by a SMG and overseen by a SSG. The SMG includes the researchers involved in designing the study, the site principle investigator (DR), and the patient and public involvement representative and will discuss and resolve any logistical issues that occur. The SSG is responsible for the analyses of results and will include the chief and lead researcher, the patient and public involvement representative, the site principle investigator and academics from the University of Birmingham with expertise in designing and conducting PA interventions.
Any protocol deviations will be documented, and the sponsor and chief investigator will be notified instantly. All investigators and site staff will comply with GDPR and the Data Protection Act 2018 when gathering, storing and dispensing of personal participant information. Only the chief investigator, who will also be the data custodian, the lead investigator, and second coder (SF) who is part of the SMG, will have access to the data to enable quality inspection and data analysis. Although there are minimal risks involved with this study, a management plan is in place should any problem arise. During the semi-structured interviews or focus groups if the researchers are concerned for the participants well-being, mechanisms for safeguarding the participant and managing any distress will be implemented, including discussion (with permission from the participant) with the site lead physiotherapist (DR) to mitigate harm.
Peer review
As part of the funding application, the study rationale, methodology and intended analysis have been independently peer reviewed by the Musculoskeletal Association of Chartered Physiotherapists’ research committee. Therefore, this protocol has been peer reviewed by an appropriate, independent professional body. The findings will be presented in an article in an open access peer-reviewed journal and conferences nationally and internationally. The funder will be provided with a study report and a lay summary of the report (led by the patient and public involvement representative) will be written for patients with lower-limb OA. Phase I participants will be invited to attend a presentation of the results which will provide a further opportunity for them to provide critical feedback.
Supplemental material
Supplemental material
References
Footnotes
Twitter @abrushton
Contributors MJW is a PhD student and AR is the lead supervisor, and JD and CAG are cosupervisors. AR (chief investigator) and MJW (lead investigator) led on development of the protocol and gaining approvals (eg, ethics). AR, CAG and JD provided critical guidance on the conception, methodological decisions, design, and proposed analyses and dissemination. MJW and SF will be involved in data analysis and interpretation. DR is the principal investigator at the clinical site and is involved in data acquisition. All authors will contribute to data interpretation and conclusions. MJW drafted the initial version of the protocol manuscript. All authors have read, contributed to and agreed the final manuscript. AR is the guarantor of the study.
Funding This study is being supported by the Musculoskeletal Association of Chartered Physiotherapists level 3 research award.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval NHS ethical and HRA approval and site capacity and capability have been obtained (IRAS 247904).
Provenance and peer review Not commissioned; externally peer reviewed.