Article Text

Abstract
Background Immune checkpoint blockade (ICB) targeting programmed cell death protein 1 and cytotoxic T lymphocyte-associated protein 4 has achieved modest clinical activity as salvage therapy in relapsed small cell lung cancer (SCLC). We conducted this signal-finding study to assess the efficacy of ICB with or without radiation in relapsed SCLC.
Methods Patients with relapsed SCLC and ≤2 previous lines of therapy were randomized to (1) arm A: durvalumab (D) 1500 mg/tremelimumab (T) 75 mg (intravenously every 4 weeks without stereotactic body radiation therapy (SBRT)) or (2) arm B: immune-sensitizing SBRT to one selected tumor site (9 Gy × 3 fractions) followed by D/T. Treatment continued until progression or a maximum of 12 months. The co-primary endpoints of the study were overall response rate (ORR) and progression-free survival (PFS). We evaluated circulating lymphocyte repertoire in serial peripheral blood samples and tumor infiltrating lymphocytes (TILs) from on-treatment biopsies as pharmacodynamic markers.
Results Eighteen patients were randomized to arms A and B (n=9 each): median age 70 years; 41.2% women. The median PFS and ORR were 2.1 months and 0% in arm A and 3.3 months and 28.6% in arm B. The median overall survival (OS) was 2.8 months in arm A and 5.7 months in arm B (p=0.3772). Pooled efficacy of D/T±SBRT in 15 Response evaluation criteria in solid tumors (RECIST) evaluable patients across both arms showed the best ORR in terms of partial response in 13.3%, stable disease in 26.6% and progressive disease in 60.0%; the overall median PFS and OS were 2.76 and 3.9 months. The most common adverse events were grade 1 fatigue (66%) and grade 1 elevated amylase (56%) in arm A, and grade 1 fatigue (56%) and pain (44%) in arm B. There was a significant increase in activated CD8(+)ICOS+ T cells (p=0.048) and a reduction in naïve T cells (p=0.0454) in peripheral blood following treatment, along with a significant amount of activated CD8+ICOS+ T cells in TILs from responders.
Conclusions The D/T combination with and without SBRT was safe but did not show sufficient efficacy signal in relapsed SCLC. Changes in peripheral blood lymphocyte and TILs were consistent with an immunologic response.
Trial registration number NCT02701400.
- lung neoplasms
- clinical trials
- phase II as topic
- immunotherapy
- programmed cell death 1 receptor
- radioimmunotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- lung neoplasms
- clinical trials
- phase II as topic
- immunotherapy
- programmed cell death 1 receptor
- radioimmunotherapy
Introduction
Effective salvage therapy for small cell lung cancer (SCLC) remains a challenge and an area of great need yet unmet.1 There is a strong rationale for testing immune checkpoint inhibitors in SCLC. It is already well established that the development of effective antitumor immunity manifesting as paraneoplastic syndrome in patients with SCLC is associated with prolonged and durable disease control in contrast to that in patients without paraneoplastic syndrome.2 Similarly, high levels of suppressor T reg and low levels of effector T cells in peripheral blood were associated with progression of disease in SCLC.3 Single-agent nivolumab, atezolizumab and pembrolizumab have been tested and showed encouraging but modest clinical benefit of pharmacologic blockade of programmed cell death protein 1 (PD-1) or its ligand (PD-L1) in relapsed SCLC.4–7 Moreover, the addition of ipilimumab, a cytotoxic T lymphocyte-associated protein 4 (CTLA-4) inhibitor, to nivolumab showed greater benefit over nivolumab alone in a subset of SCLC defined by high tumor mutation burden.8 Nonetheless, only a third of patients derived any clinical benefit from this combination therapy strategy. In the absence of a reliable biomarker for patient enrichment, a complementary therapeutic intervention that can enhance antitumor efficacy of immune checkpoint blockade (ICB) without increasing toxicity will expand the benefit of immune checkpoint inhibitors to a larger proportion of patients.
Limited institutional experience and large randomized studies suggested a survival benefit with the use of consolidation radiation therapy in extensive-stage SCLC.9 10 In preclinical models, ionizing radiation can induce PD-L1 expression on tumor and stromal cells along with an increase in myeloid-derived suppressor cells.11–13 Also the release of tumor-associated antigens following radiation-induced cell death may be highly immunogenic, leading to potentiation of antitumor efficacy of systemic immunotherapy agents even at distant tumor sites.13–15 The combination of an anti-PD-L1 inhibitor and radiation was shown to be synergistic in xenograft models of pancreatic, colon and breast cancer.13–15
The biologic premise behind the strategy of combining immune-modulating agent and radiation is the expectation that the tumor-antigen release induced by localized radiation will activate adaptive immune response directed against tumor-specific antigens.11 12 This response can be further enhanced by pharmacologic stimulation by checkpoint inhibitors. Thus, while radiation induces local response at the radiated site, it can also indirectly improve disease control at distant sites outside the radiation field through the so-called abscopal effect.16
This study was designed to explore whether combined ICB with or without radiation will have meaningful efficacy signal in relapsed SCLC. The study design also allowed the assessment of the safety of the combination of irradiation along with combined ICB.
Methods
The primary objective of this phase II trial was to determine the efficacy of the combination of durvalumab and tremelimumab with or without stereotactic body radiation therapy (SBRT) in relapsed SCLC using primary endpoints of progression-free survival (PFS) and overall response rate (ORR). All subjects provided written informed consent prior to undergoing any study-related procedures. The study was registered at www.clinicaltrials.gov.
Study design
The study was a randomized, two-arm, non-comparative phase II clinical trial designed to study the efficacy of durvalumab and tremelimumab with or without SBRT in patients with relapsed SCLC.
Eligibility
Patients were eligible for this trial if they were aged 18 years or older with pathologic diagnosis of SCLC that had progressed after not more than two prior lines of treatment, including a platinum doublet chemotherapy. Other eligibility criteria included the presence of at least one site of measurable disease according to the Response evaluation criteria in solid tumors (RECIST) version 1.1 criteria; good performance status (Eastern Cooperative Oncology Group 0–2); and adequate organ function as indicated by absolute neutrophil count (ANC) ≥1.5×109/L, platelet count ≥100×109/L, hemoglobin >9 gm/L, serum bilirubin ≤1.5× upper limit of normal (ULN), serum transaminase ≤2.5× ULN, and serum creatinine clearance >40 mL/min by the Cockcroft-Gault or the Modification of Diet in Renal Disease (MDRD) formula or by 24-hour urine collection for determination of creatinine clearance. Exclusion criteria included prior treatment with a PD-1, PD-L1 or CTLA-4 inhibitor; current or prior use of immunosuppressive medication within 28 days before the first dose of durvalumab or tremelimumab, with the exception of intranasal and inhaled corticosteroids or systemic corticosteroids at physiologic doses not exceeding 10 mg/day of prednisone or an equivalent corticosteroid; active or prior documented autoimmune disease within the past 2 years; and history of primary immunodeficiency or allogeneic organ transplant.
Treatment
Durvalumab was administered at a standard dose of 1500 mg once every 4 weeks for 12 months and tremelimumab at 75 mg every 4 weeks for up to four doses per cycle. Patients with ongoing clinical benefit may continue durvalumab for 12 additional months. Patients remained on treatment until evidence of disease progression, intolerable toxicity, or withdrawal of consent.
Stereotactic body radiation therapy
Patients randomized to arm B underwent standard radiation planning procedures for LINAC-based SBRT delivery systems. The prescribed dose was 9 Gy in three fractions, delivered every other day to a single non-target lesion 1 week prior to initiation of durvalumab and tremelimumab. Lesion selection was at the discretion of the radiation oncologist based on extracranial location, evidence of progression and the safe delivery of SBRT, and not the same as the primary target lesion(s) followed for response by the RECIST criteria. Prior to treatment delivery, a cone beam CT was obtained to verify accurate target localization. All treatments were delivered with 6–10 MV photons. CT simulation was performed with robust immobilization, including Civco abdominal compression body frames for targets within the thorax and Medical Intelligence immobilization for abdominal tumor targets including liver or adrenal lesions. Four-dimensional CTs were required for treatment planning. Motion management for moving targets included creation of an internal target volume (ITV) inclusive of the tumor during all phases of the respiratory cycle, or if target motion was >1 cm phase gating was used during treatment planning and delivery. Standard expansions of 5 mm were used from the ITV to the planning target volume (PTV). Dose coverage of the PTV was mandated at 95% of the PTV receiving 100% of the prescribed dose. Heterogeneity within the PTV was required to range between 110% and 140%.
Efficacy
Treatment effect was assessed on non-irradiated measurable disease according to RECIST 1.1 criteria using cross-sectional anatomical imaging scans obtained at baseline within 4 weeks of starting treatment and at the end of every two cycles of treatment until progression or withdrawal from study. Efficacy was classified as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). PFS was calculated from treatment initiation to the time of disease progression or death, while overall survival (OS) was calculated from treatment initiation until date of death or censoring.
Correlative analysis
Image-guided tumor biopsies from consenting patients were obtained at baseline prior to initiation of treatment and at after 2 cycles of durvalumab and tremelimuab just prior to cycle 3. Samples were immediately dissociated into suspensions of individual cells by mechanical agitation through sieve with a plunger. The sieved suspension material was washed in RPMI medium with 10% fetal bovine serum (FBS) and stored until ready for flow cytometric analysis. Enumeration of lymphocyte subsets in paired blood samples and tumor biopsies was performed by flow cytometry using approximately 200–300 µL of red blood cells-lysed samples stained with specific antibodies along with controls as previously described.17 18
Statistics
All patients meeting the eligibility requirements were randomly assigned to one of two treatment groups (arm A or arm B) using block randomization generated by the study statistician, with block size of 2 to guarantee each group will have an equal number of 10 patients. Descriptive statistics were employed to summarize baseline subject characteristics, tumor types, and adverse event experience. Subjects who received any dose of study drugs were eligible for inclusion in the safety analysis. Efficacy was assessed in patients who completed at least two cycles of D/T and had two imaging scans available for comparisons. With the assumption of a median PFS of 3 months if no improved efficacy over current standard treatment with topotecan versus a high efficacy threshold of 7 months of median PFS, a sample size of 10 patients treated in each arm of the study provides 87% power to demonstrate the hypothesized efficacy improvement at a one-sided 10% alpha level test. Statistical analysis was conducted using SAS V.9.4. Kaplan-Meier plot and log-rank test were performed for OS, PFS and other relevant covariates. Statistical analysis was conducted using SAS V.9.4 and SAS macros developed by the Biostatistics and Bioinformatics Shared Resource at Winship Cancer Institute. We used paired two-tailed t-test to compare differences in circulating lymphocyte subsets measured in blood samples collected at baseline and on treatment using GraphPad Prism V.6.0.
Results
Patient and tumor characteristics
The study enrolled a total of 18 patients (9 patients per arm) with relapsed, progressive SCLC who were eligible for initiation of salvage therapy. Details of patient demographics and disease characteristics at the time of registration, by treatment arm, are summarized in table 1. Patient distribution across the two arms was comparable by ethnicity, gender, line of treatment and platinum sensitivity (table 1). There were no patients remaining on active treatment and only one patient was still alive at the time of manuscript writing. Due to the increased use of immune checkpoint agents as part of standard front line and salvage regimens for relapsed SCLC, accrual on study was slow, leading to early termination prior to planned target enrollment.
Patient demographics, tumor characteristics and treatment efficacy across both arms of the study
Efficacy
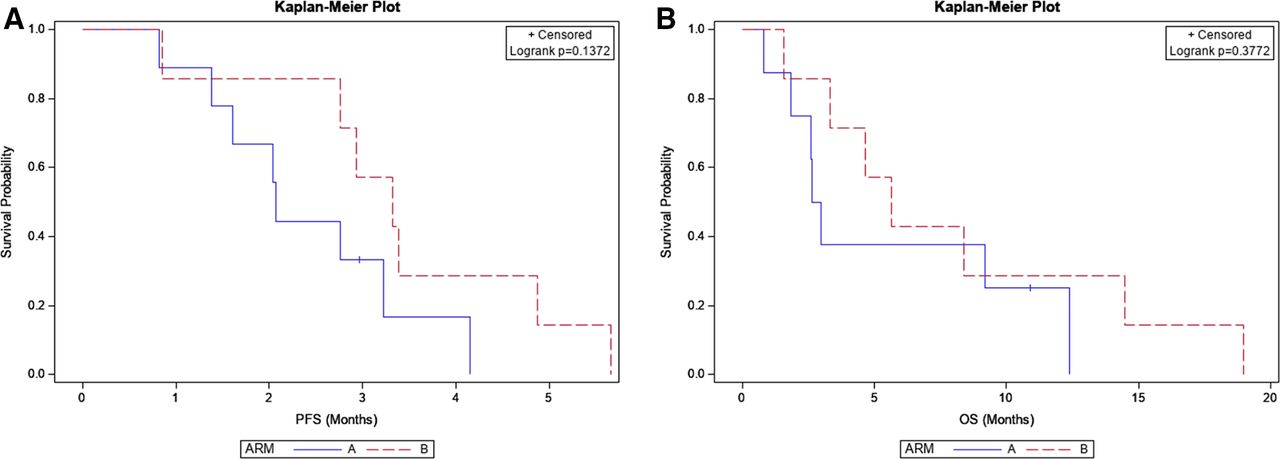
Two patients in arm B did not receive immunotherapy and were completely excluded from efficacy analysis. There were two objective responses by RECIST criteria, both in patients in arm B treated with SBRT along with durvalumab and tremelimumab. The two patients with confirmed response, one with platinum-sensitive disease and the other with platinum-refractory relapse, experienced deep PR in non-irradiated lesions in the liver and lymph nodes. Notably, there was a near CR in a suprahilar mass that received SBRT per protocol (online supplemental figure S1). The following were the response classifications in arms A and B of the study, respectively: CR: 0% and 0%; PR: 0% vs 28.6%; SD: 25% and 14.3%; and PD: 75% and 57.1% (table 1). The median PFS for the pooled sample across both arms was 2.76 months. There was a numerical increase in median PFS for arm B compared with arm A (3.3 (0.9, 4.9) vs 2.1 (0.8, 3.2) months, respectively; p=0.1372) (figure 1). Similarly, the pooled median OS was 3.9 months. This was numerically longer for patients enrolled in arm B versus arm A (5.7 (1.6, 14.5) vs 2.8 (0.8, 12.4) months, respectively; p=0.3772) (figure 1).
Supplemental material
Supplemental material

Non-comparative Kaplan-Meier curves for progression-free survival (PFS) and overall survival (OS) in arm A and arm B of the study.
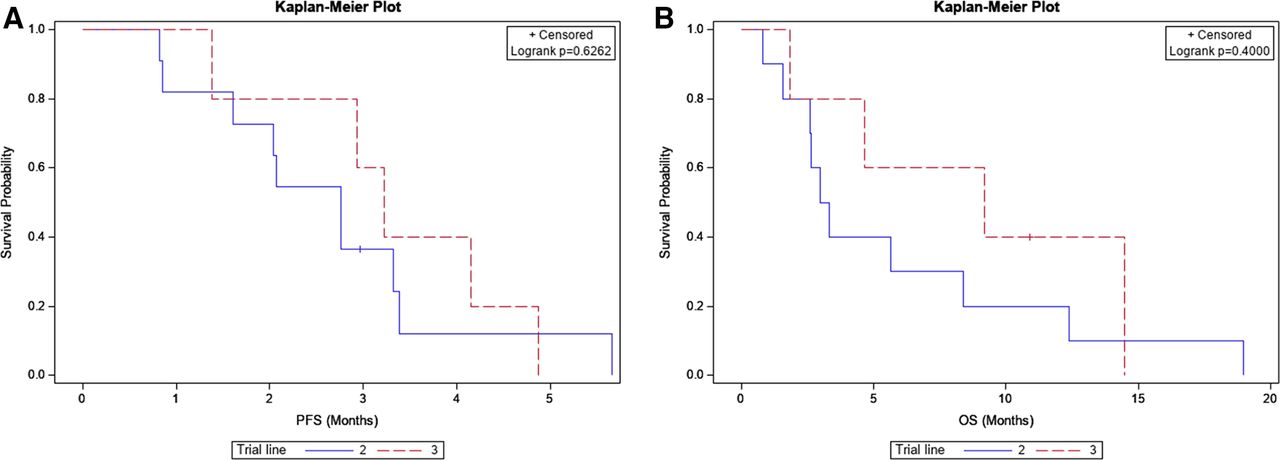
Exploratory efficacy analysis for durvalumab and tremelimumab in the combined population of patients across both arms showed no significant difference in efficacy between patients with platinum-sensitive and platinum-refractory disease both for PFS (p=0.7760), although there was a trend in OS favoring patients with platinum-sensitive disease (4 (0.8–8.4) vs 9.2 (1.8–19); p=0.1360) (figure 2). Similarly, PFS and OS were comparable between patients treated with durvalumab and tremelimumab as second-line versus third-line therapy (figure 3).
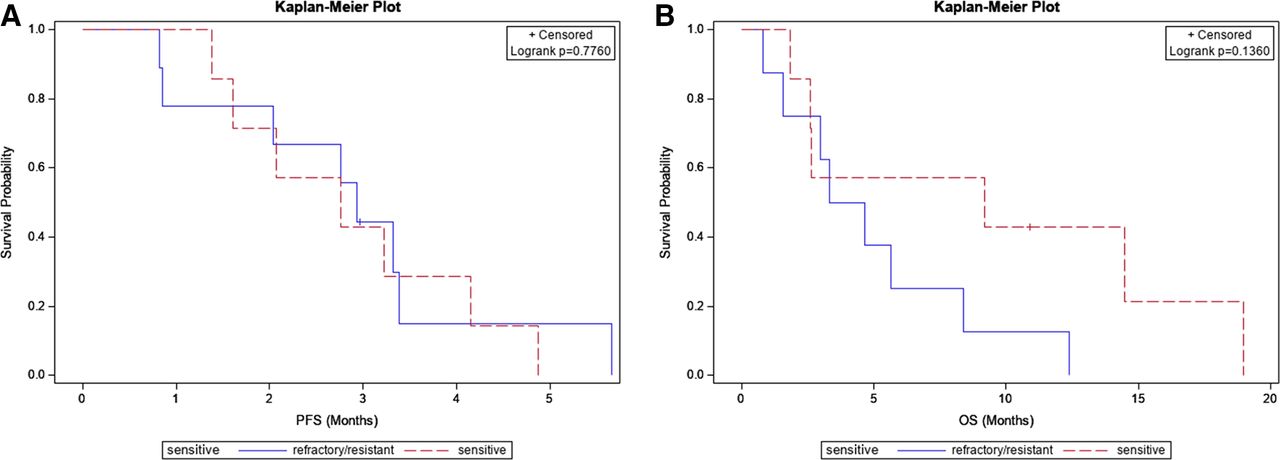
Kaplan-Meier curves for progression-free survival (PFS) (left) and overall survival (OS) (right) for combined data across both arms for platinum-sensitive and resistant relapse.
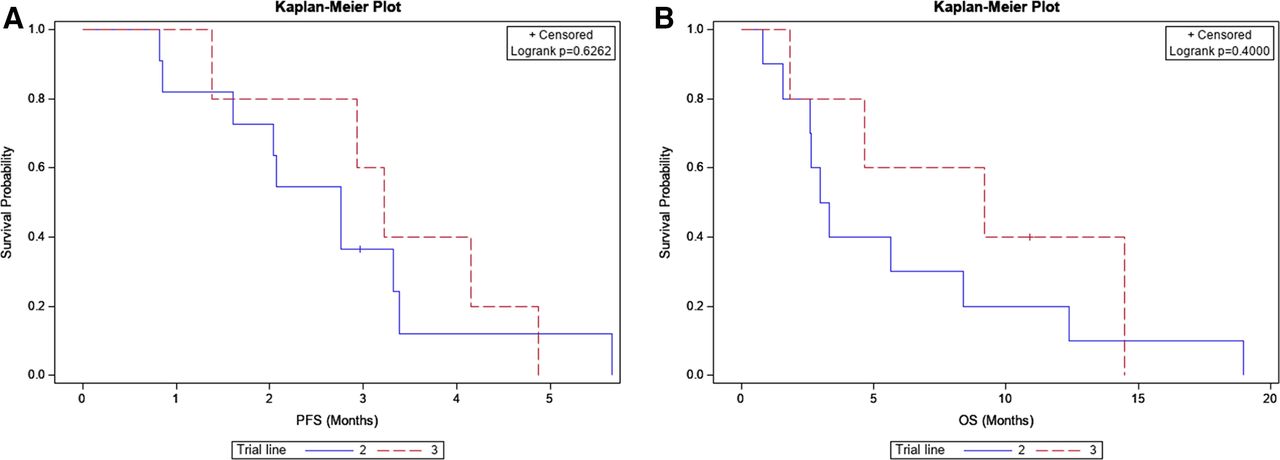
Kaplan-Meier curves for progression-free survival (PFS) (left) and overall survival (OS) (right) with combined data across both arms for patients treated with second-line versus third-line therapy.
Adverse events
The most frequently reported treatment-emergent adverse events regardless of attribution or causality were grade 1 in severity. The most frequent adverse events in arm A were grade 1 fatigue (66%), grade 1 elevated amylase (56%) and grade 2 dyspnea (33%). In arm B, the most frequent adverse events were grade 1 fatigue (56%), grade 1 pain (44%), grade 3 diarrhea (33%), and grade 1 thrombocytopenia (33%) (table 2).
Type, grade and frequency of adverse events regardless of attribution across the two arms of the study
Correlative analysis
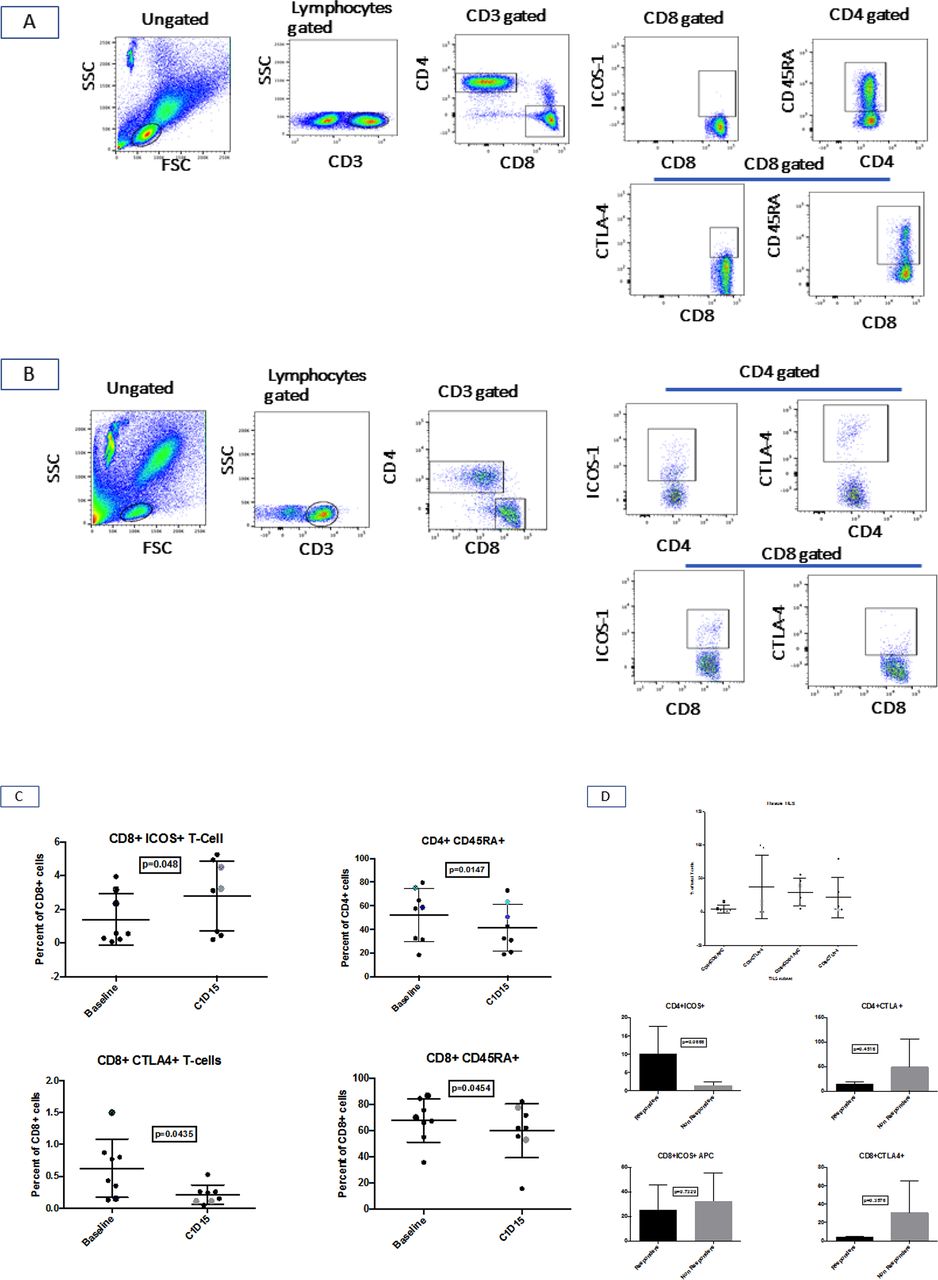
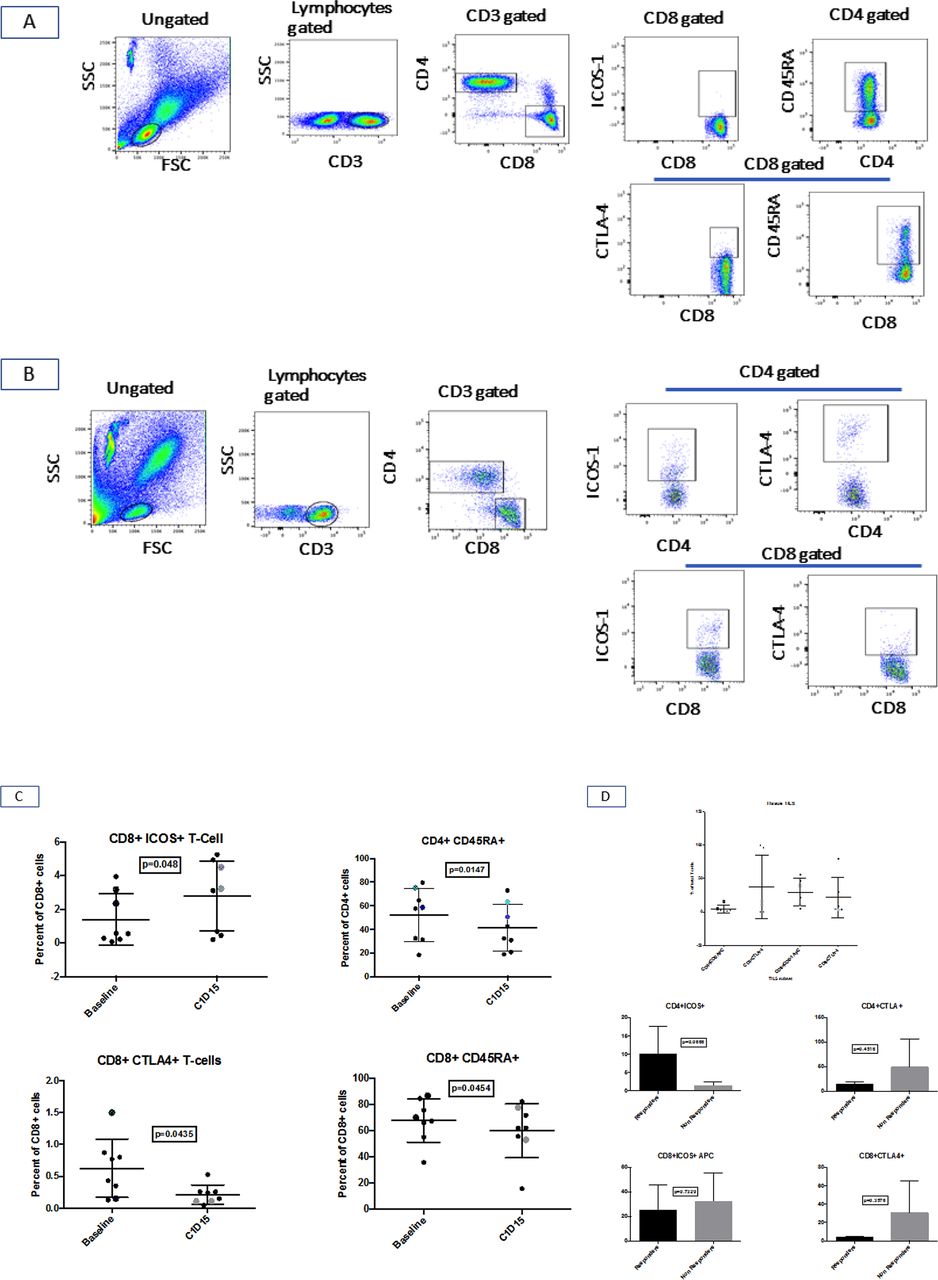
Analysis of peripheral blood samples collected from patients at baseline and on treatment (day 15 of cycle 1) using standard gating approaches (figure 4A,B) showed a general decrease in naïve CD4+CD45RA+ T cells, CD+CD45RA+ T cells and CD8+CTLA-4+ T regs, along with an increase in activated CD8(+)ICOS+ T cell subset (figure 4C). On-treatment biopsy obtained after one cycle of treatment in consenting patients showed distribution of tumor infiltrating lymphocytes (TILs) subsets retrieved from tumor biopsies. There was an activated immune phenotype with higher proportion of activated CD8+ICOS+ T cells and lower proportion of CTLA-4+ subsets of both CD4 and CD8+ T lymphocytes (figure 4D).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Representative flow cytometric gated populations of red blood cells-lysed white cells. (B) Flow cytometric gated populations of TILs from biopsy samples. (C) Comparison of lymphocyte subsets in peripheral blood samples collected at baseline versus on treatment on day 15 of cycle 1 with reduced proportion of naïve CD4+ and CD8+ T cells, increased activated CD8+ICOS+ T cells and reduced levels of CD8+CTLA-4+ cells. (D) TIL distribution in tumor biopsies showed higher proportion of activated CD8+ICOS+ T cells and lower proportion of CTLA-4+ subsets of both CD4 and CD8+ T lymphocytes; colored hatched symbols highlight the two patients with objective response by RECIST 1.1 criteria. CTLA-4, cytotoxic T lymphocyte-associated protein 4; FSC, forward scatter; SSC, side scatter; TILs, tumor infiltrating lymphocytes.
Discussion
Preclinical models suggested that the addition of immunogenic doses of radiation may result in improved efficacy of checkpoint agents targeting the PD-1 and CTLA-4 pathways.13 15 We conducted this study seeking to demonstrate that such a strategy will be safe and likely to result in improved efficacy in patients. The high efficacy threshold set for this exploratory study to be considered worthy of further evaluation was not met. The median PFS of 2.1 and 3.3 months in the two arms of this study are in the same range as previously reported with immune checkpoint inhibitors in patients with relapsed SCLC.19 We noted a trend in efficacy signal with the addition of SBRT to the combination of durvalumab and tremelimumab, where the median PFS and median OS were numerically higher. One potential confounder is the schedule of restaging scan, which was not fixed but based on completed treatment cycles. Delayed treatment for whatever reason could have led to a delay in obtaining restaging scan, thereby leading to a false conclusion of increased PFS in the affected arm of the study. However, there was no significant delay in obtaining restaging scan on schedule in this study and therefore not an alternative explanation for the numerically longer PFS in arm B. Moreover, other efficacy endpoints showed a consistent trend in favor of arm B, including OS and the two patients with objective tumor response. The 1-year OS rate was similar in both arms at 29.2% (4.2%, 61.9%) vs 28.6% (4.1%, 61.2%) for arm A and arm B, respectively. This is comparable with the 1-year survival rates ranging between 27% and 34% reported from other studies of checkpoint inhibitors in unselected patients with relapsed SCLC.4–6
A major challenge with immunotherapy across all tumor types is the fact that only a subset of patients benefit from this treatment. However, a reliable biomarker to select such patients remains elusive. PD-L1 expression, which is the best validated and most widely used predictive biomarker for PD-1 targeted checkpoint inhibitors, is expressed in a minority of SCLC.20–22 Moreover, PD-L1 expression did not associate with efficacy of nivolumab, although it was predictive of improved efficacy with pembrolizumab.4 19 Patients were enrolled in this study without biomarker selection, which could potentially have increased the chances of showing an efficacy signal. Correlative analysis comparing baseline blood sample with repeat sample after treatment revealed evidence of immunologic response. There were increased levels of activated circulating CD8+ICOS+ T lymphocyte subset in peripheral blood and higher proportion of activated T cells in TILs from biopsy samples. Our result is consistent with prior studies in patients with non-small-cell lung carcinoma and other tumor types in which dynamic changes with increased levels of activated T lymphocytes in the peripheral blood were associated with efficacy.23 24 This is an interesting finding that could be employed to further adapt the use of checkpoint inhibitor therapy in this patient population.
This phase II trial demonstrated the safety of the combination of durvalumab and tremelimumab in relapsed SCLC. This is consistent with a similar study in melanoma testing the safety of irradiation along with nivolumab and ipilimumab.25 In addition, the incorporation of SBRT did not result in increased toxicities in this patient population. The SBRT doses used in this study were modest doses intended to be immunogenic rather than ablative to the radiated target. Immune-related adverse events were somewhat less frequent than the rate reported for a different combination of CTLA-4 and PD-1 targeted antibody, ipilimumab and nivolumab, in this patient population. The reason for this observation could be related to the fact that the study of ipilimumab in relapsed SCLC employed a higher dose of 3 mg/kg, which is associated with a heightened rate of immune-related adverse events as observed also in patients with melanoma.19
Although we were unable to demonstrate a clear signal of improved efficacy with the addition of SBRT to combined ICB in relapsed SCLC, this question remains relevant for future studies. Importantly, we successfully established the safety of the combination of SBRT with dual ICB. Welsh et al 26 also recently reported the safety of the addition of pembrolizumab to conventional thoracic radiation as consolidation following induction chemotherapy for extensive-stage SCLC, as well as the combination of pembrolizumab with definitive chemoradiation in patients with limited-stage SCLC.27 The safety profile established in this study will facilitate our follow-up study that is designed to evaluate whether SBRT to primary non-responsive site will impact the efficacy of chemoimmunotherapy in the front-line treatment of patients with extensive-stage SCLC. We envisage that such a strategy will further improve the modest impact already achieved with front-line chemoimmunotherapy in this disease.28–30
In conclusion, this study failed to show a strong signal of efficacy required for the combination of durvalumab and tremelimumab with or without SBRT to be deemed worthy of further exploration in relapsed SCLC. Future studies that leverage radiation and immunotherapy synergy in an earlier line of treatment for this disease, along with enrichment strategies for patients who are likely to benefit from immunotherapy, should be pursued.
Acknowledgments
We thank the patients and family members and are grateful to Anthea Hammond, PhD, for editorial assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @teekayowo
Contributors Study conception and design: TKO and KH. Acquisition of data: SP, KH, CS, GZ, SW, MSH, BN, EKW, SR and TKO. Data analysis: ZC, CZ, MSH, EKW and TKO. Manuscript writing and approval: all authors.
Funding This work was supported by AstraZeneca with funding and free supply of durvalumab and tremelimumab to all enrolled patients. Research reported in this publication was also supported in part by the Biostatistics and Bioinformatics Shared Resource of Winship Cancer Institute of Emory University and the National Cancer Institute at the National Institutes of Health under award number P30CA138292.
Competing interests AstraZeneca provided funding for this study and is manufacturing the products being evaluated in the research described in this paper. TKO and KH served as paid consultants to AstraZeneca and personally received compensation for these services. The terms of this arrangement have been reviewed and approved by Emory University in accordance with its conflict of interest policies.
Patient consent for publication Not required.
Ethics approval The study was approved by the Emory University IRB. The study was performed in accordance with the Declaration of Helsinki and with the ethical standards enshrined in the US Common Rule.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository, deposited at www.clinicaltrials.gov. Detailed de-identified participant data are available upon reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.