Article Text

Statistics from Altmetric.com
“Crack lung” is an acute pulmonary syndrome with a spectrum of clinical and histopathological findings. Smoking crack, a potent and highly addictive crystalline form of cocaine, usually involves deep inspiration followed by the valsalva manoeuvre and coughing.
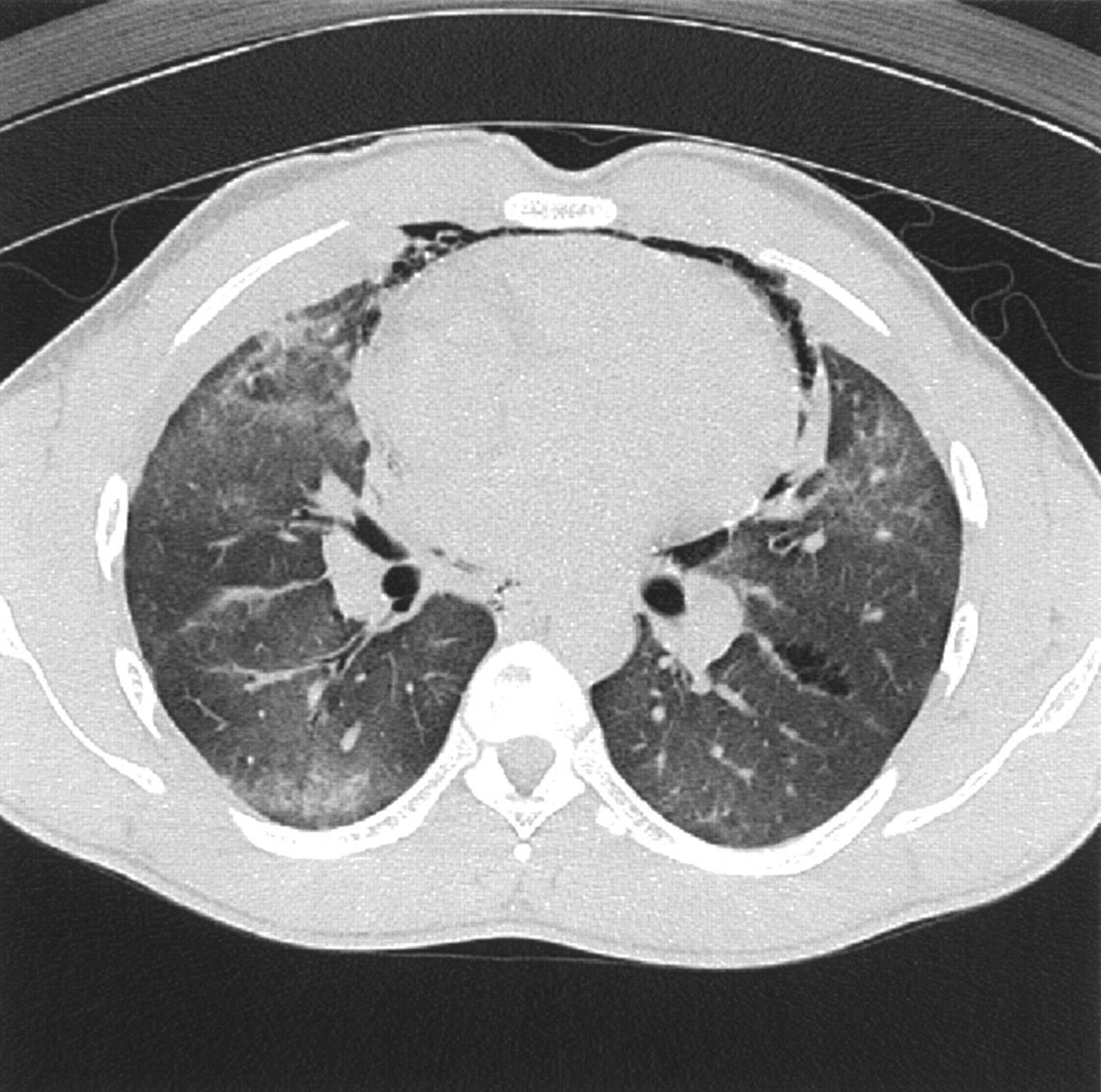
A 30 year old man presented 8 hours after smoking crack with severe chest pain and coughing. His chest radiograph showed perihilar and lower zone interstitial infiltrates and a pneumomediastinum. Computed tomography (CT) was performed. The CT image at the level of the lower lobe bronchi shows ground glass opacity in both lungs and free gas within the mediastinum, anterior to the cardiac silhouette (fig 1). There is also a focal collection of gas adjacent to a left lower lobe vessel which has an irregular border and within which small soft tissue strands can be seen, which represents an area of pulmonary interstitial emphysema due to alveolar rupture. The ground glass opacities probably reflect the presence of pulmonary oedema.
Learning points
-
Crack smoking can cause pneumomediastinum as well as pneumothorax.
-
Barotrauma of any cause (in this case, bronchospasm) can cause alveolar rupture with air tracking to the mediastinum along interstitial planes (with or without a pneumothorax).
-
Pulmonary oedema, which may not be clinically manifest (as in this case), is well reported.
The presumed sequence of events in this patient is that he developed acute injury due to inhalation of crack causing bronchospasm, increased alveolar pressure and then alveolar rupture, followed by interstitial emphysema dissecting along the vascular sheaths and connective tissue planes to the mediastinum. The patient recovered rapidly without intervention other than oxygen and his chest radiograph returned to normal after 3 days.

{kind=link}
CT scan showing free gas within the mediastinum anterior to the cardiac silhouette and ground glass opacity.