
Abstract
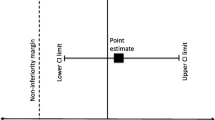
Noninferiority (NI) clinical trials have been used to assess antibacterial drug efficacy in treating nosocomial and ventilator-associated pneumonia. Previously published trials have employed prespecified NI margins of 15% or 20% based on clinical response or microbiological endpoints. However, as those studies do not describe the statistical and clinical considerations underpinning the margins selected, their scientific plausibility cannot be substantiated. In this report, a fixed NI margin of 7% with respect to all-cause mortality is determined based on the 29% cross-study difference between the two-sided 95%, confidence intervals (CI) for the placebo estimate of 62% (95% CI: 52%, 71%) and the active control estimate of 20% (95% CI: 18%, 23%) obtained from meta-analyses of various published clinical studies. After applying discounting, we estimated the active control treatment benefit to be 14%. Due to clinical concerns, 50% of the active control treatment benefit was preserved, yielding a 7% NI margin.
Article PDF
Similar content being viewed by others

References
Klevens RM, Edwards JR, Richards CL, et al. Estimating health care-associated infections and deaths in US hospitals, 2002. Public Health Rep. 2007;122:160.
Celis R, Torres A, Gatell JM, et al. Nosocomial pneumonia; a multivariate analysis of risk and prognosis. Chest. 1988;93(2):318–324.
Leone M. Garcin F, Bouvenot J. et al. Ventilator-associated pneumonia: breaking the vicious circle of antibiotic overuse. Crit Care Med. 2007; 35(2):379–385.
Kollef MH, Ward S. The influence of mini-BAL cultures on patient outcomes: implications for the antibiotic management of ventilator-associated pneumonia. Chest. 1998;113:412–420.
Torres A, Aznar R, Gatell JM, et al. Incidence, risk. and prognosis factors of nosocomial pneumonia in mechanically ventilated patients. Am Rev Respir Dis. 1990:142:523–528.
Alvarez-Lerma F, ICU-Acquired Pneumonia Study Group. Modification of empiric antibiotic treatment in patients with pneumonia acquired in the intensive care unit. Intensive Care Med. 1996;22:387–394.
Leroy O, Meybeck A, d’Escrivan T, et al. Impact of adequacy of initial antimicrobial therapy on the prognosis of patients with ventilator-associated pneumonia. Intensive Care Med. 2003;29:2170– 2173.
Rello J, Vidaur L, Sandiumenge A, et al. De-escalation therapy in ventilator-associated pneumonia. Crit Care Med. 2004;32:2183–2190.
Teixeira PJZ, Seligman R, Hertz FT, Cruz DB, Fachel JMG. Inadequate treatment of ventilator-associated pneumonia: risk factors and impact on outcomes. J Hosp infect. 2007;65:361–367.
Iregui M, Ward S, Sherman G, Fraser VJ, Kollef MH. Clinical importance of delays in the initiation of appropriate antibiotic treatment of ventilator-associated pneumonia. Chest. 2002:122: 262–268.
Luna CM. Blanzaco D, Niederman MS. et al. Resolution of ventilator-associated pneumonia: prospective evaluation of the clinical pulmonary infection scores as an early clinical predictor of outcome. Crit Care Med. 2003;31:676–682.
Luna CM, Vujacich P, Niederman MS, et al. Impact of BAL data on the therapy and outcome of ventilator-associated pneumonia. Chest. 1997; 111:676–685.
Luna CM, Aruj P. Niederman MS, et al. Appropriateness and delay to initiate therapy in ventilator-associated pneumonia. Eur Respir J. 2006; 27:158–164.
American Thoracic Society, Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388–416.
US Food and Drug Administration, Points to consider; clinical development and labeling of anti-infective drug products. 1992. Retrieved on November 4. 2009, from: https://doi.org/www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm070975.pdf.
US Food and Drug Administration. Guidance for industry—nosocomial pneumonia—developing antimicrobial drugs for treatment. 1998. Retrieved on January 6, 2010, from: https://doi.org/www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm071170.pdf.
International Conference on Harmonization. ICH E10. Choice of control group and related issues in clinical triais. Retrieved on October 26, 2009, from: https://doi.org/www.fda.gov/RegulatoryInformation/Guidances/ucm125802.htm.
US Food and Drug Administration. Guidance for industry—antimicrobial drug products: use of noninferiority studies to support approval (draft guidance). 2007 Retrieved on October 26, 2009, from: https://doi.org/www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm070951.pdf.
Temple R, Ellenberg SS. Placebo-controlled trials and active-control trials in the evaluation of new treatments. Part 1: ethical and scientific issues. Ann Intern Med. 2000;133:455–463.
Hung HMJ, Wang SJ, O’Neill R. A regulatory perspective on choice of margin and statistical inference in non-inferiority trials. Biometrical J. 2005;47(1):28–36.
Zanetti G, Bally F, Greub G, et al. Cefepime versus imipenem-cilastatin for treatment of nosocomial pneumonia in intensive care unit patients: a multicenter, evaluator-blind. prospective, randomized study. Antimicrob Agents Chemother. 2003:47(11):3442–3447.
Rea-Neto A, Niederman M, Lobo SM, et al. Efficacy and safety of doripenem versus piperacillin/tazobactam in nosocomial pneumonia: a randomized, open-label, multicenter study. Curr Med Res Opin. 2008;24(7):2113–2126.
Chastre J, Wunderink R, Prokocimer P, et al. Efficacy and safety of intravenous infusion of doripenem versus imipenem in ventilator-associated pneumonia: a multicenter. randomized study. Crit Care Med. 2008;36:1089–1096.
West M. Boulanger BR, Fogarty C, et al. Levofloxacin compared with imipenem/cilastatin followed by ciprofloxacin in adult patients with nosocomial pneumonia: a multicenter, prospective, randomized, open-label study. Clin Ther. 2003;25:485–506.
Wunderink RG, Mendelson MH, Somero MS, et al. Early microbiological response to linezolid vs vancomycin in ventilator-associated pneumonia due to methicillin-resistant Staphylococcus aureus. Chest. 2008;134:1200–1207.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–188.
Kaul S, Diamond GA. Good enough: a primer on the analysis and interpretation of noninferiority trials. Ann Intern Med. 2006;145:62–69.
Stevens RM, Teres D, Skillman J. Feingold DS. Pneumonia in an intensive care unit: a 30 month experience. Arch Intern Med. 1974;134: 106–111.
Smith IM, Champion MC, Hazard EC, Lowry L, Leaverton PE. Single and combined antibiotics in the treatment of Pseudomonas aeruginosa infections, In: Progress in Antimicrobial and Anticancer Chemotherapy: Proceedings of the 6th International Congress of Chemotherapy. Vol. 1, Baltimore. MD: University Park Press, 1970:718–724.
Rubinstein E, Cammarata SK, Oliphant TH, Wunderink RG, and the Linezolid Nosocomial Pneumonia Study Group. Linezolid (PNU-100766) versus vancomycin in the treatment of hospitalized patients with nosocomial pneumonia: a randomized. double-blind, multicenter study. Clin Infect Dis. 2001;32:402–412.
Wunderink RG, Cammarata SK, Oliphant TH, Kollef MH, and the Linezolid Nosocomial Pneumonia Study Group. Continuation of a randomized, double-blind. multicenter study of linezolid versus vancomycin in the treatment of patients with nosocomial pneumonia. Clin Ther. 2003;25:980–992.
Fink MP, Snydman DR, Niederman MS, et al. Treatment of severe pneumonia in hospitalized patients: results of a multicenter. randomized, double-blind trial comparing intravenous ciprofloxacin with imipenem/cilastatin, Antimicrob Agents Chemother. 1994;38:547–557.
Alvarez-Lerma F, Insausti-Ordenana J, Jorda-Marcos R, et al. Efficacy and tolerabilily of piperacillin/tazobactam versus ceftazidime in association with amikacin for treating nosocomial pneumonia in intensive care patients: a prospective, randomized, mullicenter trial. Intensive Care Med. 2001;27:493–502.
Brun-Buisson C, Sollet JP, Schweich H, Briere S, Petit C, and the VAP Study Group. Treatment of ventilator-associated pneumonia with piperacillin-tazobactam/amikacin versus ceftazidime/amikacin: a multicenter, randomized, controlled trial. Clin Infect Dis. 1998;26:346–354.
Joshi M, Metzler M, McCarthy M, Olvey S, Kassira W, Cooper A. Comparison of piperacillin/tazobactam and imipenem/cilastatin, both in combination with tobramycin, administered every 6 h for treatment of nosocomial pneumonia. Respir Med. 2006; 100: 1554–1565.
Schmitt DV, Leitner E, Welte T, Lode H. Piperacillin/tazobactam versus imipenem/cilastatin in the treatment of nosocomial pneumonia—a doable blind, prospective, multicenter study. Infection. 2006;34:127–134.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sorbello, A., Komo, S. & Valappil, T. Noninferiority Margin for Clinical Trials of Antibacterial Drugs for Nosocomial Pneumonia. Ther Innov Regul Sci 44, 165–176 (2010). https://doi.org/10.1177/009286151004400208
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1177/009286151004400208