
Abstract
Extract: Two patients with cataracts and a defect in galactose metabolism were studied. A hemolysate of erythrocytes respired well on galactose-1-phosphate. Galactose-1-phosphate uridyltransferase activity in red cells was normal and uridine diphosphogalactose 4-epimerase was also active. Erythrocyte galactokinase activity was completely absent in both patients (fig. 1). Only insignificant amounts of 14CO2, were formed from galactose-1-14C by the patients' hemolysates (table I).
After a breakfast containing 850 ml of milk was taken by one patient, the galactose level in blood rose from 7.6 to a maximum of 44.9 mg/100 ml at 60 minutes and was still at 32.1 mg/100 ml 1 ½ hours later, while that of glucose rose from 90 to 136 mg/100 ml at 60 minutes and then dropped (fig. 2).
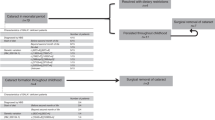
In the hour preceding the load, the patient excreted 0.36 g of galactose, 0.63 g of galactitol and 0.04 g of glucose; within 150 minutes after breakfast he excreted 1.90 g, 0.83 g and 0.72 g respectively. Galactose and galactitol concentrations were remarkably high in the one hour portion before the load (0.45 and 0.77 g/100 ml respectively).
One patient drank 3 liters of milk a day over a period of 5 days. Total urinary output was 191.51 g of galactose and 47.97 g of galactitol which together are almost equivalent to  of the ingested galactose from milk (table III). The daily ranges of urinary loss of these two compounds were remarkably narrow and the ratio of urinary galactitol to urinary galactose was 1:4 and constant.
of the ingested galactose from milk (table III). The daily ranges of urinary loss of these two compounds were remarkably narrow and the ratio of urinary galactitol to urinary galactose was 1:4 and constant.
Within the same time 2.4 g of glucose were excreted in a total of 9980 ml of urine. Amino acid excretion was normal. During this 5 day study period, daily urinary excretion of total nitrogen was 19.6-22.3 g while that of α-amino nitrogen was 124.3-191.1 mg, both considered to be at the upper limit of the norm. Creatinine excretion ranged from 882 mg to 1139 mg per day.
The parents of the patients were related (fig. 3). The youngest brother of the patients and his family as well as the 4 living children of the oldest patient and their families were studied for galactokinase activity. A group of one hundred normal subjects served as controls (table IV).
In normal subjects galactokinase activity ranged from 0.138 to 0.359 with an average of 0.257 (2 σ = 0.083) μmoles galactose phosphorylated/ml RBC/hr.
In the family of the patients (fig. 4) the results of the enzyme assays fell into 3 groups : the 2 patients with virtually complete enzyme deficiency; some of their relatives with intermediary values; and others within a wide range above 0.240 μmoles/ml/hr. The 4 children of the oldest patient, 26 to 38 years of age, had activities of 0.131 to 0.145 μmoles/ml/hr, and the youngest brother of the patients, at the age of 38 years, had an activity of 0.154, values clearly below those of the members of the control group (fig. 5). One grandchild of the oldest patient as well as four of the six children of her youngest brother, aged 11 to 16 years, also had low activities.
In the blood cells of the 2 patients studied here a virtually complete absence of galactokinase activity was demonstrated. After milk ingestion, extraction of galactose from the blood in the youngest patient was extremely slow. Thus, one would assume that galactokinase activity in the liver of this patient was absent or at least reduced to a minimum.
The results of the assays of erythrocyte galactokinase in the family of the patients are consistent with inheritance of the defect as an autosomal recessive trait.
The deficiency or the heterozygous state may be factors related to the formation of cataracts beyond infancy and childhood.
Speculation: The study of patients with galactokinase deficiency will provide new insights into the intermediary galactose metabolism in man.
Prevention of cataract formation due to galactokinase deficiency must be sought; it may be attained by the screening of the newborn population for hypergalactosemia and by the immediate removal of all galactose from the diet.
Similar content being viewed by others

Article PDF
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Gitzelmann, R. Hereditary Galactokinase Deficiency, a Newly Recognized Cause of Juvenile Cataracts31. Pediatr Res 1, 14–23 (1967). https://doi.org/10.1203/00006450-196701000-00002
Issue Date:
DOI: https://doi.org/10.1203/00006450-196701000-00002
Keywords
This article is cited by
-
Richard Gitzelmann (23rd February 1930–31st October 2013)
European Journal of Pediatrics (2014)
-
Features and outcome of galactokinase deficiency in children diagnosed by newborn screening
Journal of Inherited Metabolic Disease (2011)
-
Congenital cataract: The history, the nature and the practice
Eye (1998)
-
Assignment of congenital cataract Volkmann type (CCV) to chromosome 1p36
Human Genetics (1995)
-
Gonadal function in galactosemics and in galactose-intoxicated animals
European Journal of Pediatrics (1995)
