


Abstract
Background: With the introduction of resident duty hour restrictions and the resulting in-house trainee shortages, a long-term solution to ensure safe and efficient patient care is needed. One solution is the integration of nurse practitioners (NPs) and physician assistants (PAs) in a variety of health care settings. We sought to examine the use of NPs and PAs on surgical/trauma services and their effect on patient outcomes and resident workload.
Methods: We performed a systematic review of EMBASE, Medline, CINAHL, and the Cochrane Central Register of Controlled Trials. We included studies (all designs) examining the use of NPs and PAs on adult surgical and trauma services that reported the following outcomes: complications, length of stay, readmission rates, patient satisfaction and perceived quality of care, resident workload, resident work hours, resident sleep hours, resident satisfaction, resident perceived quality of care, other health care worker satisfaction and perceived quality of care, and economic impact assessments. We excluded studies assessing nonsurgical/trauma services or pediatrics and review articles.
Results: Twenty-nine articles met the inclusion criteria. With the addition of NPs and PAs, patient length of stay decreased, and morbidity and mortality were unchanged. In addition, resident workload decreased, sleep time increased, and operating time improved. Patient and health care worker satisfaction rates were high. Several studies reported cost savings after the addition of NPs/PAs.
Conclusion: The addition of NPs and PAs to surgical/trauma services appears to be a safe, cost-effective method to manage some of the challenges arising because of resident duty hour restrictions. More high-quality research is needed to confirm these findings and to further assess the economic impact of adding NPs and PAs to the surgical team.
With the introduction of resident duty hour (RDH) restrictions and the resulting shortages of in-hospital trainee availability, a long-term solution to ensure safe and efficient patient care is needed. One of the most well-researched solutions is the integration of nurse practitioners (NPs) and physician assistants (PAs) in a variety of health care settings. These NPs and PAs, often called “midlevel practitioners,” “nonphysician providers,” or “physician extenders” (PEs), have been shown to be a safe and effective addition to health care teams1,2 To avoid the negative connotation associated with the term “midlevel practitioners,” we prefer to use the term PEs to refer to NPs and PAs.
These practitioners differ in the training they have undertaken and in their background education. Nurse practitioners are registered nurses (RNs) who have met the requirements for working as bedside nurses and have then completed a graduate degree and training program. Physician assistants have an undergraduate education in a variety of disciplines, including life sciences and health care. They complete a PA training program and may or may not complete a graduate degree, depending on the requirements of their jurisdiction of practice. Both types of practitioners have the ability to prescribe, diagnose and perform medical procedures. The difference between the 2 types is that NPs can work autonomously and are registered under the College of Nurses of a specific jurisdiction, whereas PAs work under a physician or group of physicians and are registered under the respective College of Physicians.1 Both NPs and PAs have been shown to be valuable members of the health care team in a variety of settings.3
With increasing physician workload and decreasing availability of in-house trainees, the use of NPs and PAs has become increasingly popular.1 Surgical services have been shown to value the importance of NPs and PAs, and evidence has shown the “value added” of having these practitioners on a surgical team in a variety of settings.4 These providers have been shown to improve access to care, decrease wait times, promote wellness and preventative care, provide continuity of care, foster interprofessional collaboration, improve followup, and decrease costs and readmission rates.5,6
We performed a systematic review to examine the use of NPs and PAs on surgical/trauma services and their effect on patient outcomes and resident workload.
Methods
Following the PRISMA checklist (www.prisma-statement.org), we performed a systematic review of the literature on EMBASE, Medline, CINAHL, and the Cochrane Central Register of Controlled Trials in May 2015.
Inclusion criteria
Randomized controlled trials (RCTs), cross-sectional studies, cohort studies, case series and surveys
Studies examining the use of NPs and PAs on adult surgical and trauma services
Studies reporting patient-related outcomes, including complications, length of stay (LOS), readmission rates, satisfaction and perceived quality of care
Studies reporting resident-related outcomes, including workload, work hours, sleep hours, satisfaction and perceived quality of care.
Studies reporting other health care worker–related outcomes, including satisfaction and perceived quality of care.
Economic assessments of the use of NPs and PAs on adult surgical and trauma services
Exclusion criteria
Studies evaluating NPs and PAs in nonsurgical or nontrauma services
Studies pertaining to pediatric patient services
Studies not examining the aforementioned outcomes
Review articles
Commentaries or letters to the editor
Search strategy
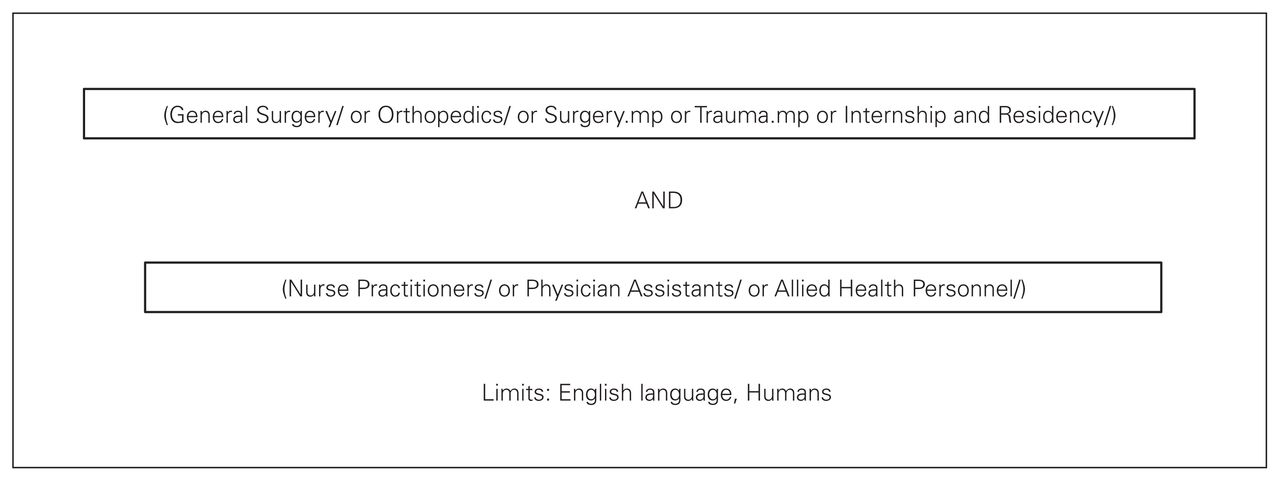
An example of the search strategy used when querying Medline can be seen in Figure 1. We queried each database and compiled the results, removing duplicates. Both of us then reviewed the titles independently, followed by abstract review. At both of these stages disagreement led to inclusion. Each of us then reviewed the full manuscripts of the selected abstracts, at which point consensus was necessary for inclusion. The reason for exclusion at the manuscript review stage is documented in Table 1.
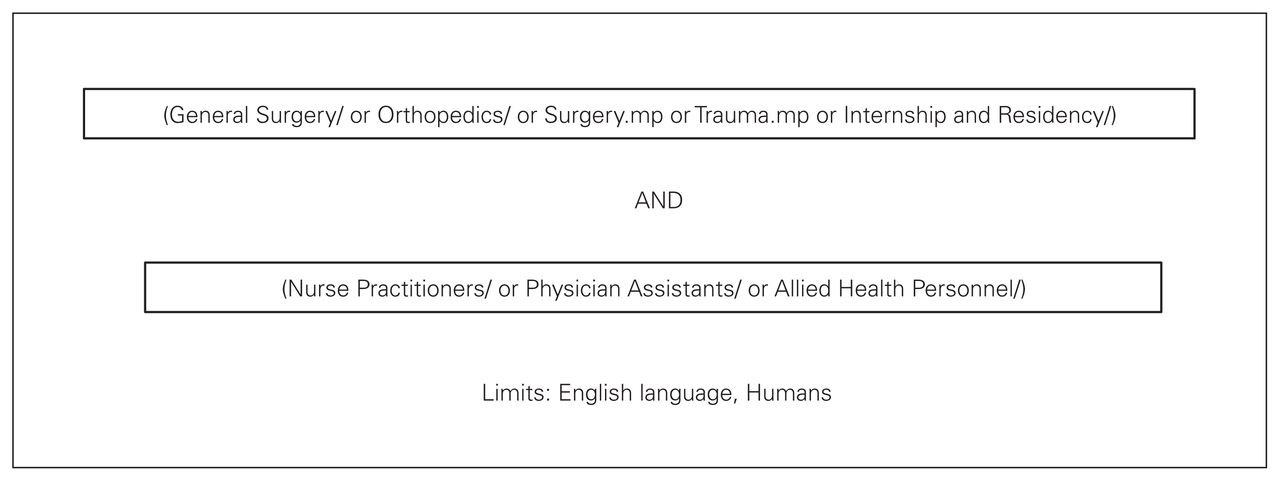
Example of the search strategy used when querying Medline.
Excluded studies
One of us collected data relating to the specified outcome measures. Generic data, such as title, authors, study design, journal and year of publication, were recorded. Specific data relating to the outcomes described in the inclusion criteria were also recorded.
We assessed risk of bias of all included manuscripts (at the study level) using the Cochrane Collaboration’s assessment tool. Given the retrospective design of most of the included studies, a strong risk of bias exists. Most importantly, a strong risk of selective outcome reporting is present in all studies.
Heterogeneity and the qualitative nature of many of the outcomes precluded statistical analysis of the results.
Results
Included manuscripts
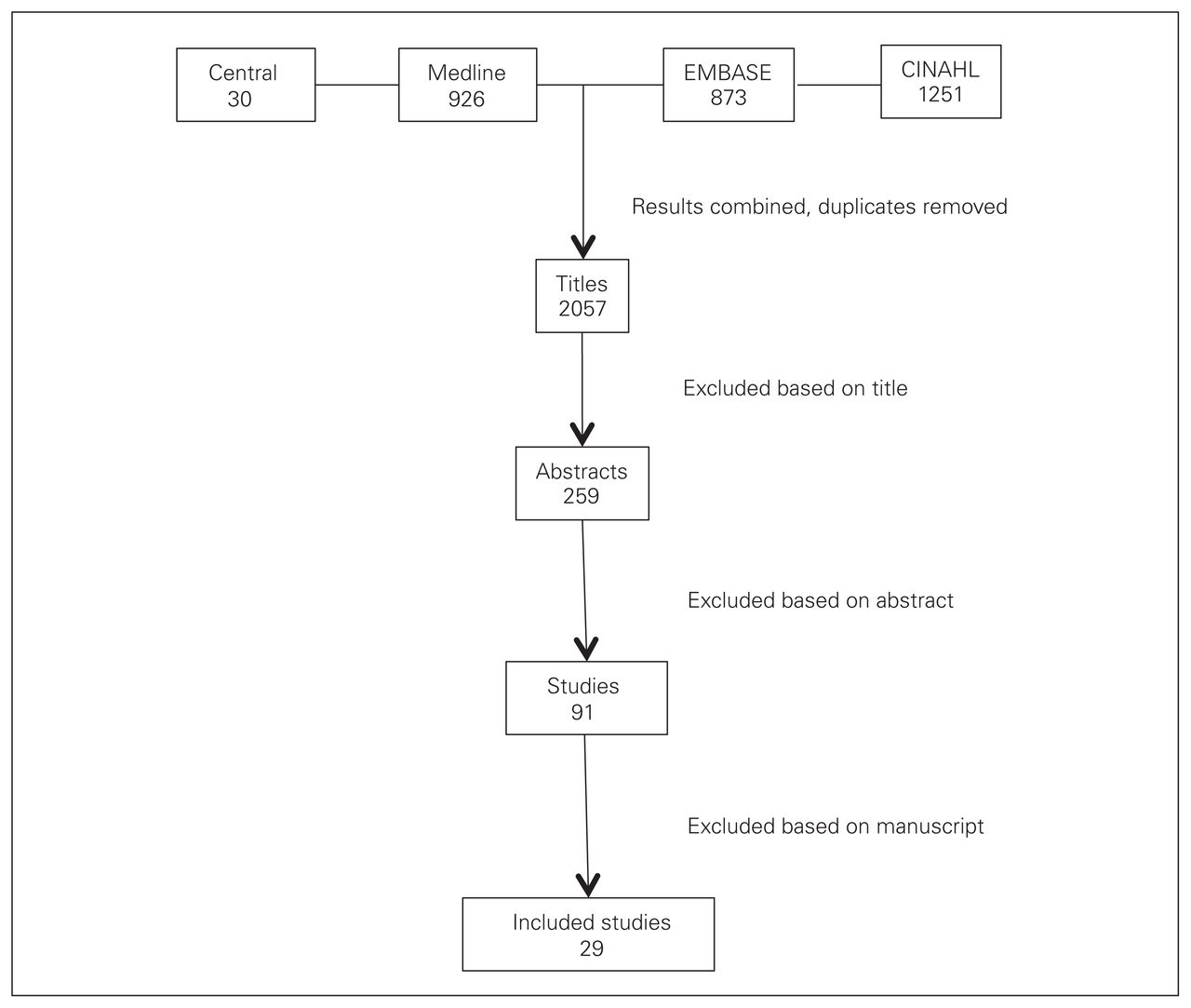
Twenty-nine articles from 29 different first authors met our inclusion criteria (Table 2 and Fig. 2). The most prevalent journal was the Journal of Trauma, having published 10 of the articles. Publication dates ranged from 1990 to 2014; however, 21 of the articles were published in the past 10 years. There were 15 case–control articles, 5 retrospective reviews, 8 surveys and only 1 RCT. Specialties included in the 29 articles were trauma service (11), cardiac/cardiothoracic/cardiovascular surgery (7), general surgery (4), orthopedic surgery (3), urology (1) and neurosurgery (1); 2 articles encompassed multiple surgical specialties. Most studies were case–control studies (15) or surveys (8). Overall the methodological quality and level of evidence of the included articles was low, with only 1 level-1 and 1 level-2 study included (Table 2). Notably, a risk of selective outcome reporting existed for all studies.
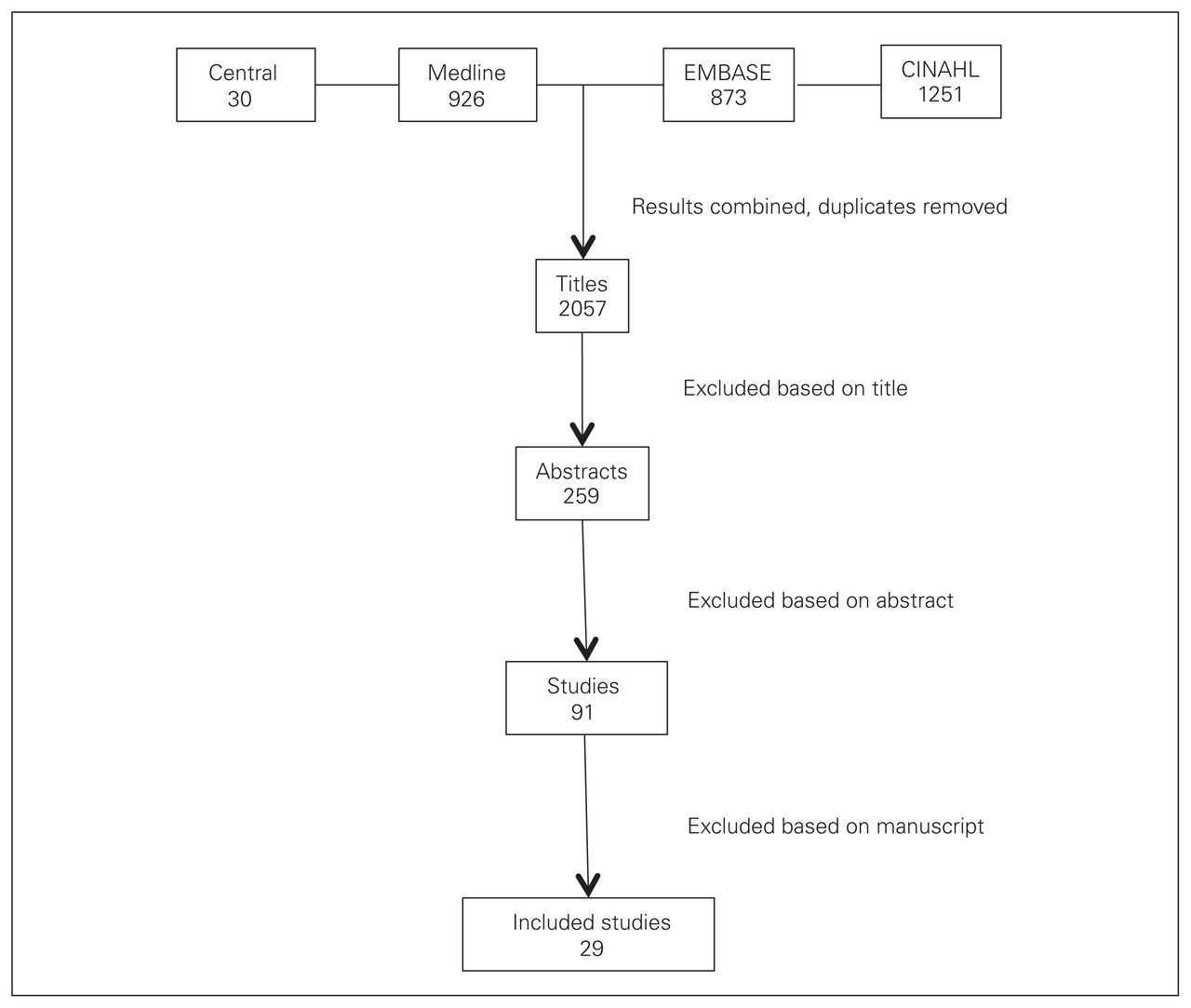
Study selection process. Central = Cochrance Central Register of Controlled Trials.
Included studies
Length of stay
Of the 8 articles that examined patient LOS as an outcome, 7 (88%) found that LOS decreased after the addition of PEs to the service.7–14 One paper found the LOS unchanged. Six articles reported actual LOS improvements, which ranged from 0.25 to 2 days (Table 3). Three of the included papers also demonstrated a decrease in intensive care unit LOS.
Decrease in patient length of stay after the addition of PEs
Morbidity and mortality
None of the included studies demonstrated an increase in morbidity or mortality with the addition of PEs to the service in question. Two studies found that complication rates were decreased.12,15 One study found an increase in the rate of diagnosis of deep vein thrombosis after PEs became involved in patient care.13
Procedures
Two articles specifically reviewed procedures performed by PEs.16,17 Bevis and colleagues16 reviewed thoracostomy tube placement in trauma patients, comparing procedures performed by PEs to those performed by trauma surgeons. They found no difference in complication rates when PEs performed the procedure. Young and Bowling17 examined intracranial pressure monitor placement by PEs and found no significant difference in complication rates when compared with monitors placed by neurosurgeons. In addition, Sirleaf and colleagues18 found no difference in complication rates between procedures performed by residents or PEs, including arterial lines, central venous catheters, thoracostomy tubes, bronchoalveolar lavage, percutaneous endoscopic gastrostomy and tracheotomies.
Effect on residents
Nine papers examined the effect of PEs on surgical residents.7,9,19–25 The main effects documented included a decrease in overall resident work hours, increased operating room time, reduced number of pages, increased time for educational activities and increased sleep time. Victorino and Organ22 demonstrated decreased resident workload and stress levels and improved resident morale after the addition of PEs.
Satisfaction
Six studies found either improved or high patient satisfaction rates with the addition of PEs. None of the included articles demonstrated a decrease in patient satisfaction. Nine articles examined satisfaction rates of surgeons, residents and nursing staff and found overall high satisfaction rates.4,7,8,23,26–30 Improvements to patient care, continuity of care, communication with families, improved clinical documentation and reduced workload for other health care workers were all reported as reasons for the high satisfaction rates.
Cost
Five papers reported cost outcomes (Table 4).10,14,15,25,29 All 5 reported cost savings with the addition of PEs; however, cost savings varied dramatically depending on the study. Decrease in the LOS of patients was responsible for significant cost savings in 2 articles. Bohm and colleagues29 demonstrated similar total costs with the addition of PEs; however, surgical volumes increased by 42%, and surgical wait times decreased after PEs were involved.
Manuscripts reporting cost savings
Discussion
In surgical specialties, the volume of work can often exceed the capacity of the surgeons, trainees and nursing staff. This can lead to overworked and overwhelmed health care workers. With resident duty hours increasingly under the microscope of regulatory bodies, this problem has the potential to worsen dramatically. Patient safety and continuity of care continue to be highlighted as key issues in the discussion on work hour reform. These issues will persist at both teaching and nonteaching institutes until a sustainable model of care is developed.
Many hospitals have turned to NPs and PAs to help resolve the discrepancy between workload and already overworked employees.2,3,14,15,21,23,27,30,31 It is important that we critically examine the effect that these changes have on the hospital work environment, and most importantly on patient care, before advocating widespread adoption.
Our systematic review of the literature was undertaken to investigate the integration of PEs into surgical specialties and their effect on patients, surgical residents and other health care workers. Our results demonstrate over-whelmingly positive experiences among surgical services using PEs. Overall, patients and other health care workers report high satisfaction rates.4,7,8,23,26–30 Significant reductions in hospital and intensive care unit LOS have been reported after the addition of PEs to surgical or trauma services.7–14 Morbidity and mortality remain stable, and some studies have shown a reduction of in-hospital complication rates. An overall improvement in quality of care and continuity of care, as judged by health care workers, is a frequent theme in the studies we reviewed.
In addition, substantial cost savings were reported in several studies. Two groups reported savings of more than $5000 per patient.10,14 Bohm and colleagues29 reported increased surgical volumes and reduced wait list times without changes in expenditure. The studies reporting financial outcomes originated from 3 different health care systems (Canada, United States, United Kingdom), which decreases the generalizability of the results. None of the articles described in detail the funding sources for PEs. The study by Bohm and colleagues29 — the only Canadian study examining costs — reported that funding for the PEs came directly from the provincial health authority. Their cost savings came from eliminating the need for fee-for-service PAs, who are also paid directly by the health authority, in the operating room. This finding could potentially be generalizable to other Canadian health authorities. Given the complexity of hospital budgets, a funding model would likely have to come from the government level in most Canadian centres. Further detailed reports on cost-effectiveness and funding models are needed to help institutions advocate for and implement changes.
With resident duty hours being increasingly regulated, it would be prudent to maximize residents’ educational experiences while they are in hospital. For surgical residents, this means maximizing exposure to the operating room and clinics and minimizing administrative duties. Several studies have demonstrated that the addition of PEs to surgical services helps to accomplish those goals.7,9,19,21–25 Fewer pages and administrative duties have also been shown to increase resident sleep time and to reduce resident workload and stress levels, which may further maximize residents’ educational opportunities. Some institutions in Canada have increased the number of clinical fellows to address resident shortages. Some clinical fellows can fund their positions by billing as a surgical assistant, which eliminates the financial limitations for some institutions. This model runs the risk of degrading both resident and fellow learning experiences by overcrowding the operating room and clinic. We do not believe this is a stable, long-term solution to the problems at hand.
Any changes to current care models should take continuity of care into consideration. Any transition away from the reliance on residents and other trainees (at academic institutions) and 24-hour call shifts has the potential to increase the number of patient handovers between providers.32 Increased handovers may be a source of miscommunication or noncommunication of important patient issues.32,33 Appropriate, detailed handovers and the use of electronic charting/handovers may help minimize these issues.33 Handover of patients should be kept to a minimum; however, the current care models are becoming unsustainable. Our review demonstrates no difference in patient morbidity or mortality when PEs are included in the health care team, although the impact on handover processes have not been well described. Further reports detailing the ideal methods of integrating PEs (e.g., scheduling, handovers, provider roles) would be beneficial to institutions considering a transition to PEs.
Limitations
The main limitation of this review is the heterogeneity of the included studies, which makes the analysis of the results challenging. We attempted to present the important themes highlighted in the literature. In addition, the overall methodological quality of the included studies was low, which increases the risk of bias within the studies. We would advocate for further high-quality studies in this field to confirm the results of our review. As with any systematic review, important articles can be missed. By including a search of 4 major databases, we believe that risk was minimized.
Conclusion
The addition of NPs and PAs to surgical/trauma services appears to be a safe, cost-effective method to manage some of the challenges arising due to resident duty hour restrictions. Further high-quality research is needed to confirm these findings and to further assess the economic impact of adding NPs and PAs to the surgical team.
Footnotes
Competing interests: None declared.
Contributors: A. Dodd designed the study. Both authors acquired and analyzed the data, wrote and reviewed the article and approved the final version for publication.
- Received April 1, 2017.
- Accepted November 10, 2016.
References
In this issue

{kind=link}
{kind=link}
Article tools





