


Abstract
Background: Laparoscopic adjustable gastric banding (LAGB) is considered a safe and effective treatment for severe obesity and obesity-related comorbidities. We sought to examine the outcome of LAGB delivered through a Canadian publicly funded obesity program.
Methods: We retrospectively analysed the cases of patients who underwent LAGB within a comprehensive, multidisciplinary, publically funded obesity program.
Results: A total of 178 patients underwent LAGB. Mean percentage total body weight loss at 1, 2 and 3 years was 15.8%, 20.7% and 20.3%, respectively. The most common short-term complication was postoperative nausea (19%). The medium-term complications included band migration (5.6%) and port site complications, band leakage and incisional hernia at 1% each. The reoperation rate was 4.5%. The mean surgery duration was 56 minutes and the mean length of stay was 1.4 days. The average numbers of clinic visits and band adjustments were highest in the first year. The most common investigation for postoperative symptoms was fluoroscopy (86%). An outcome comparison between the 2 generations of the REALIZE gastric band was inconclusive, requiring further data collection.
Conclusion: Publicly funded LAGB results in effective weight loss and acceptable safety over the short term. Our patients may represent a distinct population that differs from that in the private system. Long-term data are necessary to determine the cost-effectiveness of this important surgical option for severe obesity.
Laparoscopic adjustable gastric banding (LAGB) was first demonstrated successfully by Belachew and colleagues in 1995.1 Despite the early enthusiasm and an explosive growth of interest in this technique for obesity surgery, there are reports of high complication and failure rates.2,3 Over the years, with improvement of LAGB technique (transition from a perigastric to pars flaccida approach), the complication rate for LAGB has dropped to an acceptable standard.4,5 However, the current literature reports a mixture of results from the private and public systems, with no uniform long-term data. In addition, there is no consensus currently on patient selection criteria for LAGB.6,7 These controversies are reflected in that not all Canadian provinces fund LAGB as a treatment for obesity.
The publicly funded obesity treatment program at our institution is a referral-based, multidisciplinary clinic providing tertiary medical, psychological and surgical interventions. Our program recognizes obesity as a chronic disease and provides extensive preoperative multidisciplinary assessment and long-term follow-up after selecting the most appropriate patients for LAGB.
It is not known whether the current literature is representative of the outcomes that may be achieved in a Canadian, publicly funded system. We sought to examine and compare the short-term weight loss results achieved through LAGB in the publicly funded obesity program to those reported in the literature. The 2 generations of the REALIZE adjustable gastric band manufactured by Ethicon Endo-Surgery were used in this group of patients undergoing LAGB, and the difference in performance between the 2 products was also part of our investigation.
Methods
Selection criteria and study design
The study was performed in accordance with the principles in the Declaration of Helsinski, and the Human Research Ethics board approved our study protocol. Patients who attended the Weight Wise Clinic (WWC) and underwent an LAGB procedure were identified from clinic records. The patients were initially referred to the WWC if they met the eligibility criteria.8 After completion of a multidisciplinary team evaluation and the medical management component of the program, the patients were educated on all of the available surgical obesity management options, including LAGB, gastric bypass and sleeve gastrectomy. Patients at this stage had a good understanding of obesity as a disease and had undergone lifestyle, behavioural and medical treatment modifications to address this condition. The type of surgery offered was based on patient choice after individual surgical consultation unless there was absolute contraindication owing to medical or surgical history. Currently, there is no strict patient selection criteria for LAGB in our publicly funded program other than those mentioned previously8 and successful completion of the multidisciplinary preoperative program.
We performed a retrospective study involving patients who underwent LAGB during a 6-year period from 2005 to 2010. Short-term weight loss results at 1-, 2- and 3-year follow-up were analyzed. We excluded patients who underwent LAGB but had not reached at least a 1-year follow up postoperatively at our clinic from our analysis.
Outcome measurements
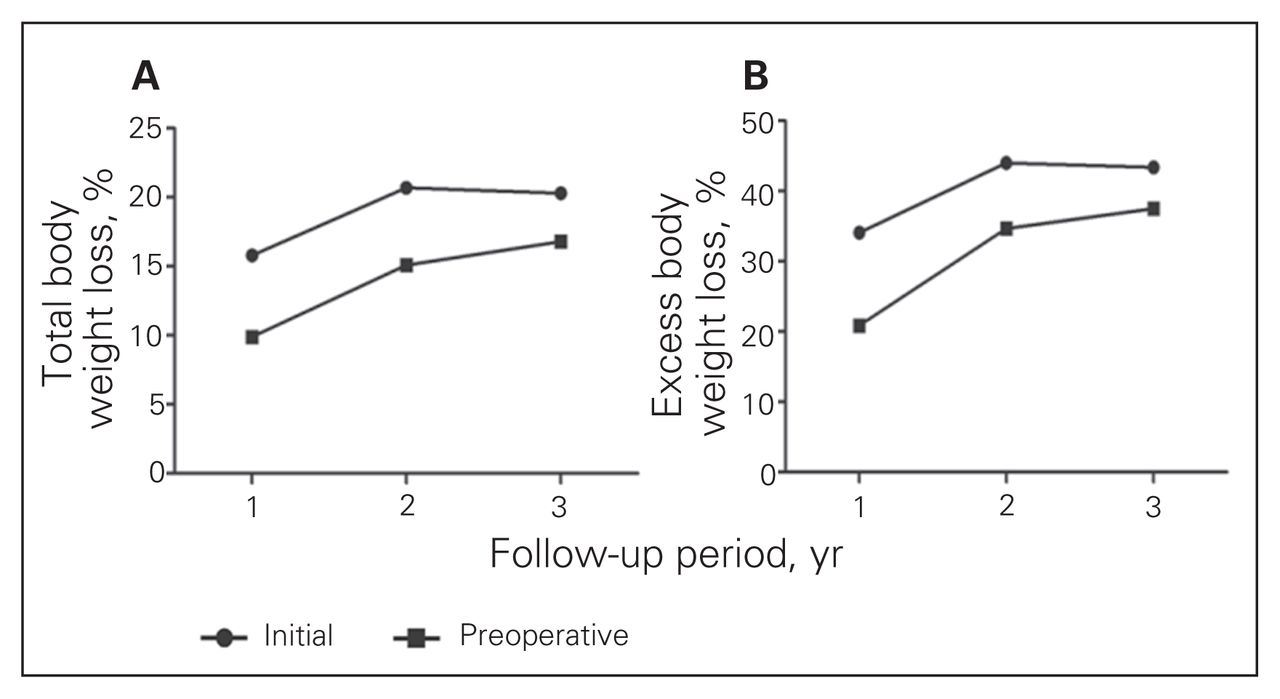
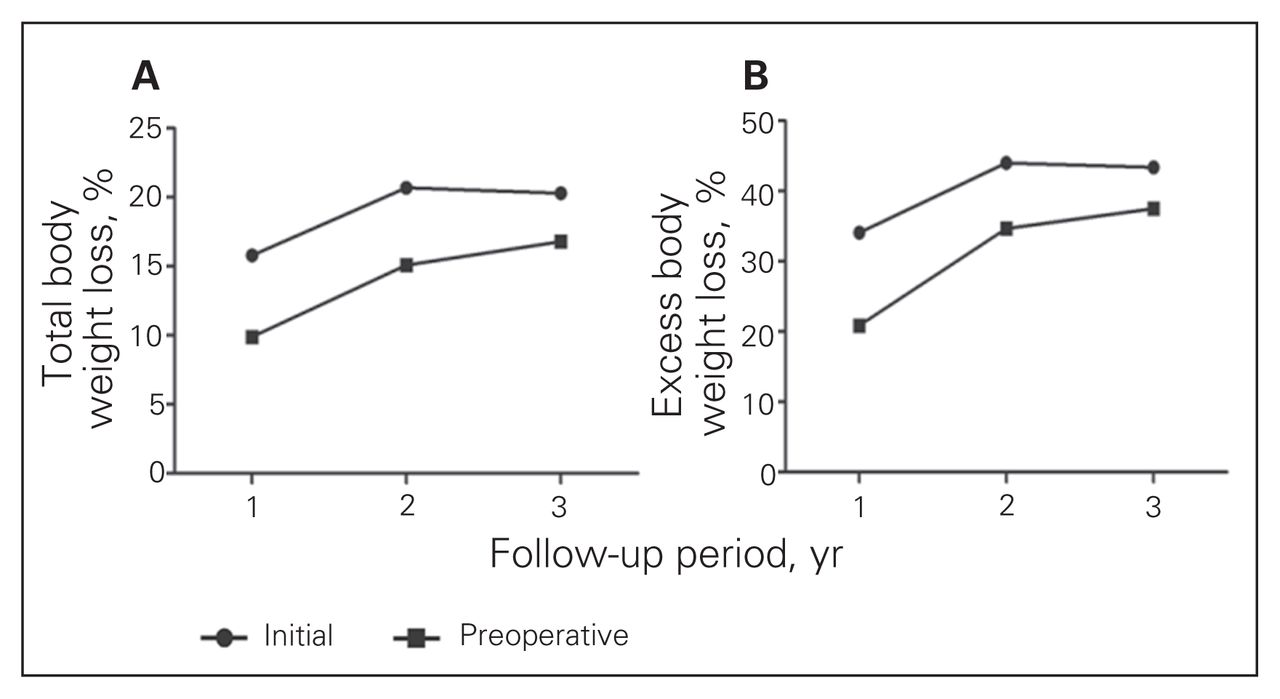
We calculated the weight loss results as both percentage total body weight loss (%TBWL) and percentage excessive body weight loss (%EBWL) based on an ideal body weight generated using a normal body mass index (BMI) of 24.9. The results were further categorized into initial and preoperative weight. Initial weight referred to follow-up weight compared to the weight recorded when the patient first arrived at the WWC. Preoperative weight referred to follow-up weight compared to the weight before surgery, typically after 12 months of lifestyle modifications and medical treatment. Comparison between the 2 data points helped to establish the effectiveness of conservative non-surgical weight management achieved at the WWC.
We separated our analysis of complications into 2 categories: short and medium term. Short term referred to the postoperative period before discharge from hospital, and medium term was the period from discharge up to 3-year follow-up. To determine the operational costs for ongoing LAGB care, we assessed the duration of surgery, length of stay (LOS), frequency of clinic visits and band fillings, and methods of investigation used during the follow-up period.
REALIZE gastric band comparison
We compared the Vrst and second generations of the REALIZE adjustable gastric band manufactured by Ethicon Endo-Surgery (Real 1 and 2). The band type was identified by specific serial number from the manufacturer, and we examined the weight loss, complication rate, operative time and LOS between the 2 groups.
Statistical analysis
Statistical analysis was performed using Stata 10 software. Results are expressed as means and standard deviations (SD) with 95% confidence intervals. We considered results to be significant at p < 0.05.
Results
Weight loss
We identified 178 patients who underwent LAGB during the study period: 153 women (86%) and 25 men (14%). The average age was 42.8 years, and the average preoperative BMI was 44.2 (SD 7). The weight loss results at 1, 2 and 3 years are presented in Table 1. The trends of weight loss over the 3 years are illustrated in Figure 1. Three patients’ weight data were not included in the weight loss analysis owing to early removal of band (n = 1) and complication or pregnancy affecting weight (n = 2) before 1-year follow-up. The preoperative conservative weight management achieved a %TBWL average of 4.4%.
Percentage total body weight loss and percentage excess body weight loss among patients who underwent laparoscopic adjustable gastric band surgery.
Postoperative compared with initial and preoperative weight loss in patients who underwent laparoscopic adjustable gastric band surgery
Safety profile
The most common short-term complications were postoperative nausea (19%) and non–surgical site infections, such as pneumonia and urinary tract infections (1%). The medium-term complication rates are presented in Table 2. The reoperation rate was 4.5%.
Medium-term complication rate from laparoscopic adjustable gastric band surgery during 3-year follow-up
Operational costs
In an analysis of operational costs, the average duration of surgery was 56 minutes, and the average LOS was 1.4 days. Clinic visits occurred most frequently in the first year, with an average of 7 visits, and dropped to 4 visits in the next 2 years. The average number of band fillings required was fills in year 1, and 1 fill only in the other 2 years. We found that 36% of our patients required at least 1 investigation postoperatively. Fluoroscopy was the most common method (86%), followed by computed tomography (9%) and upper endoscopy (4%).
REALIZE gastric band comparison
The comparison between Real 1 and 2 gastric bands is presented in Table 3. We found significant differences in pre-operative BMI, weight loss and duration of surgery. The weight loss analysis was based on 1-year follow-up data because not enough patients who received the newer Real 2 band had complete 2-year follow-up data.
Comparison between the first (Real 1) and second generation (Real 2) of the REALIZE adjustable gastric band at 1-year follow-up
Discussion
With an increasingly obese population in developed countries, bariatric surgery has been shown to be a successful treatment for obesity and its associated comorbidities.9,10 Our study demonstrates that LAGB is a safe and effective method of bariatric surgery in a Canadian system.
The weight loss achieved through LAGB in the short-term plateaued between the second and third year reaching a %TBWL of 20% and %EBWL of 44%. The %TBWL is the preferred method of discussing weight loss in our clinic, as it offers several advantages, including simplicity for patient understanding, and avoids discussion and calculations based on ideal body weight, which introduces unrealistic goals and discrepancy in reporting weight loss.11 The %TBWL achieved through our program over the 3 years was greater than the reported average of 17%.10 Looking at the 3-year %EBWL reported in the literature, which averages around 50%, our results appear to be slightly inferior.12 It is difficult to explain the apparent difference, especially when the literature data are pooled from both public and private centres with different patient selection criteria, preoperative management and follow-up processes. Calculation using %EBWL could also introduce inconsistency based on the method chosen to determine ideal weight.
One of the criticisms of LAGB is the lengthy and cumbersome follow-up, which can be difficult to maintain in a public system. The cost-effectiveness of obesity surgery has been demonstrated in moderately to severely obese patients.13 The high front-end costs can be seen in our data secondary to operation, LOS, investigations, clinic visits and band fillings. However, it is clear that the freqency of clinic visits and band fillings dropped significantly in the second and third years. The duration of surgery and LOS are among the shortest compared to other types of bariatric surgery. Many of our patients transitioned back to their family physicians for ongoing care, with stable weight established by the third year.
The high rate of postoperative nausea in our series may have resulted from multiple factors, such as anesthetic agents and tissue reaction from trauma of surgery and band placements. All of these were resolved with antiemetic agents before discharge. In severe cases, an upper gastrointestinal swallow study was conducted to rule out obstruction. With respect to safety, our complication rates were all within acceptable standards.14 The reoperation cases could mostly be attributed to band migration. The short duration of surgery, LOS, reversibility of the surgery and excellent complication profile make LAGB the least complex obesity surgery that a public system can offer.
Regarding the comparison between the first and second generations of the REALIZE gastric band, the data suggest significant differences in the duration of surgery and weight loss at 1-year follow-up. The surgery was 3 minutes longer in the newer Real 2 band group, which likely represents a small learning curve using the new product. The %EBWL was higher in the Real 1 group; however, the preoperative BMI between the 2 groups was also significantly different, with the Real 1 group having a higher BMI. Since the 2 groups’ baseline characteristics were not identical, especially with respect to preoperative weight, it is difficult to determine whether the observed difference in %EBWL is truly significant. More data collection with longer follow-up will be needed to further investigate the difference in weight loss observed between patients who received the different bands.
Conclusion
Adapting bariatric surgery in the Canadian public health care system has the potential to alleviate ongoing health care burden from obesity-related disease. Our data suggest that the weight loss achieved with LAGB in a sustainable public program is substantial and successful. The safety of the procedure has also been demonstrated clearly. Long-term data are still required to ultimately decide the true cost-effectiveness of LAGB in our system. The present study of the short-term results of LAGB in a Canadian, publicly funded program represents a realistic view of achievable weight loss through this safe and least complex obesity surgery option.
Footnotes
This study was previous presented at the 2011 Canadian Surgery Forum as an oral presentation.
Competing interests: None declared for C.J. Chiu and X. Shi. This project is financially supported by Ethicon Endo-Surgery. D.W. Birch and S. Karmali received a research grant from Ethicon Endo-Surgery to conduct this study. D.W. Birch acts as consultant for Johnson & Johnson/Ethicon Endo-Surgery, Covidien, Baxter, Bard and Olympus. S. Karmali has received a speaker’s honorarium from Ethicon Endo-Surgery.
Contributors: C.J. Chiu, D.W. Birch and S. Karmali designed the study. C.J. Chiu and S. Karmali wrote the article. All authors analyzed the data, reviewed the article and approved its publication.
- Accepted October 9, 2012.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.