


Abstract
This review is intended to raise awareness of placing a pelvic mesh to prevent perineal hernias in cases of minimally invasive (MIS) abdominoperineal resections (APR) and, in doing so, causing internal hernias through the mesh. In this article, we review the published literature and present an illustrative series of 4 consecutive cases of early internal hernia through a pelvic mesh defect. These meshes were placed to prevent perineal hernias after laparoscopic or robotic APRs. The discussion centres on 3 key questions: Should one be placing a pelvic mesh following an APR? What are some of the technical details pertaining to the initial mesh placement? What are the management options related to internal hernias through such a mesh?
Postoperative perineal hernia is a rare complication after abdominoperineal resection (APR), proctectomy, or pelvic exenteration.1 A perineal hernia can be defined as a protrusion of intra-abdominal contents through a defect in the pelvic floor. It may contain small bowel, large bowel, bladder, uterus and omentum. The first case of postoperative perineal hernia after proctectomy for rectal cancer was reported in 1939 by Yeoman.2 Since then many other case reports and case series have been published. The duration between surgery and hernia formation usually reported is 4–14 months.3–6 The most common presenting symptoms are perineal pain, dragging sensation and discomfort on standing or sitting. However, to our knowledge, there are no reported early postoperative internal hernias through a mesh defect after laparoscopic or robotic APR related to attempts at perineal hernia prevention. We present a series of 4 isolated and clustered cases of immediate postoperative obstructing and strangulated internal hernias after a laparoscopic or robotic APR. All hernias developed though a mesh that was laid down high on the pelvic brim to prevent perineal herniation. The hernias were managed laparoscopically as detailed in the section that follows. This case series was pooled from 4 different surgeons with varying surgical training who adopted the practice of placing a prophylactic mesh at different time points.
Case series presentation
All patients presented in this case series were treated with preoperative chemoradiation therapy for distal rectal cancer. During standard robotic or laparoscopic cylindrical APR surgery, attention was paid to avoid any spillage of intestinal content in the abdominal cavity. After having ascertained that the operative field was not contaminated, a nonabsorbable composite mesh was sutured high at the pelvic brim to the periostium of the sacrum, around the pelvic side walls, and to the bladder wall (males) or vaginal wall (females) using intracorporeal interrupted number 2–0 prolene horizontal mattress sutures separated from each other by about 1.5 cm. A perineal closed suction drain was then placed above the sutured gluteal folds. All patients received 7 days of postoperative antibiotics.
Case 1
A 60-year-old man underwent daVinci robot-assisted APR for rectal cancer. The distal margin of the tumour was approximately 1 cm from the anal verge (AV). The carcinoma was classified as differentiated adenocarcinoma and staged as ypT2N0M0 with Mandard grade III. Eight days after the operation, the patient experienced symptoms of intestinal obstruction. The computed tomography (CT) scan showed intestinal obstruction due to internal hernia (Fig. 1). On laparoscopy, there was an anterior defect involving previously sutured mesh through which protruded a strictured and fibrotic small bowel loop (Fig. 2). The incarcerated pelvic hernia was approached by carefully separating the herniated small bowel from the mesh and by reducing it from the pelvic cavity. The original mesh was then removed. Finally, the defect was repaired using a new sheet of composite mesh; however, anchoring sutures were placed more closely, about 0.5 cm apart.

Case 1: Computed tomography scan featuring a small bowel loop deep in the pelvic cavity with proximal small bowel loop dilatation.

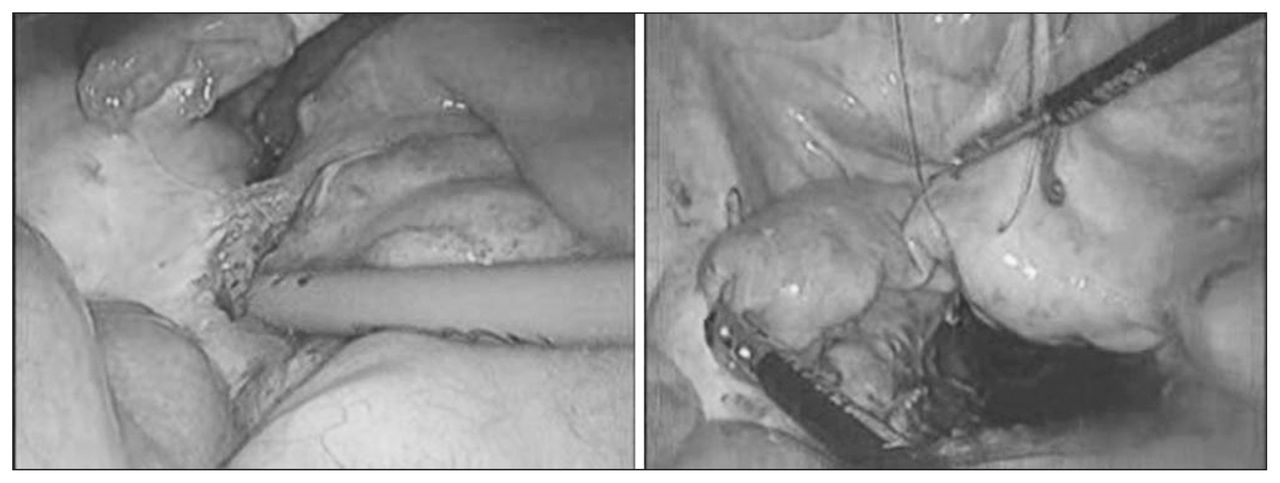
Case 1: Laparoscopic view of the internal hernia before and after small bowel reduction.
Case 2
A 58-year-old man underwent laparoscopy-assisted APR for rectal cancer (approximately 3 cm from the AV). The carcinoma was classified as differentiated adenocarcinoma and staged as ypT3N0M0 with Mandard grade IV. Seven days after the operation, the patient experienced symptoms of intestinal obstruction. A CT scan featured an intestinal obstruction due to internal hernia. As the patient became hypotensive and fever, abdominal pain and leukocytosis developed, emergency laparoscopic exploration was performed. On laparoscopy, there was a complete disruption of the previously sutured mesh where fibrotic small bowel loops protruded through multiple anterior and posterior defects. The complex hernia was managed by carefully mobilizing the herniated small bowel from the mesh and reducing it from the pelvic cavity. Since one of the reduced small bowel loops showed signs of ischemia, segmental resection with primary anastomosis was performed. The original mesh was removed. No attempt was made to obliterate the pelvic cavity as the pelvic floor was judged to be well solidified and rather shallow.
Case 3
A 63-year-old woman underwent daVinci robot-assisted APR for rectal cancer (approximately 3 cm from the AV). The carcinoma was classified as differentiated adenocarcinoma and staged as ypT2N0M0 with Mandard grade III. Ten days after the operation, the patient experienced symptoms of intestinal obstruction. A CT scan revealed a pelvic internal hernia containing a small bowel transition point. On laparoscopy, there was an anterior defect of previously sutured mesh through which protruded a loop of fibrotic small bowel. The hernia was approached by carefully mobilizing the herniated small bowel from the mesh and then by reducing it from the pelvic cavity. Despite careful handling of the incarcerated small bowel loop, a rather sizable enterotomy was inadvertently made. Segmental resection with primary anastomosis was therefore performed, and the original mesh was subsequently removed. The pelvic floor was obliterated by suturing the uterine wall to the periosteal tissue of the sacrum with anchoring sutures placed about 0.5 cm apart (Fig. 3).

Case 3: Laparoscopic view of the internal hernia before small bowel reduction and during hernia apposition with the uterus.
Case 4
An 81-year-old woman underwent laparoscopy-assisted APR for rectal cancer (approximately 6 cm from the AV). The carcinoma was classified as differentiated adenocarcinoma and staged as ypT3N0M0 with Mandard grade IV. Ten days after the operation, the patient experienced symptoms of intestinal obstruction, and a CT scan revealed a pelvic small bowel transition point. At laparoscopy, there was once again an anterior defect involving the previously placed mesh with fibrotic small bowel protruding into this defect. The hernia was dealt with similarly by careful mobilization of the herniated small bowel from the mesh and by reduction of the enteric content from the pelvic cavity. Because this small bowel loop also showed signs of ischemia, segmental resection with primary anastomosis was performed. The original mesh was removed, and no attempt was made to obliterate the pelvic cavity as the pelvic floor was judged to be well solidified and rather shallow.
Discussion
Perineal hernia is a rare complication of major pelvic surgery, such as APR, proctectomy and pelvic exenteration. The incidence, anatomy and technique of basic repair have been recently well reviewed and summarized.7,8 Radiologic, mildly symptomatic, but not necessarily requiring surgery, perineal hernias following APR have a reported prevalence of up to 7%;9 perineal hernias requiring surgical intervention have a reported prevalence of 0.2%–0.6%;10,11 and perineal hernias after pelvic exenteration have been reported more frequently, with an incidence of about 3%, reflecting the magnitude of the operation.12,13
In most cases, the perineal hernias are asymptomatic, but often enough, a dragging feeling and discomfort in the perineum, urinary symptoms and bowel compromise can occur.2–6 Despite the lack of evidence in the literature, some surgeons feel compelled to reinforce the surgically weakened pelvic floor after APR to prevent these complications. Multiple tissue as well as mesh techniques have been described to reinforce a weakened floor post–pelvic surgery.14–19 If sufficient levator muscle tissue remains, the pelvic floor is reapproximated with multiple absorbable sutures. Other ways of reinforcing the pelvic floor in cases where musculature cannot be closed include myocutaneous flaps and mesh techniques.
Multiple case reports and case series have been published on actual perineal hernia repairs. Transabdominal, perineal and combined abdominoperineal approaches as well as laparoscopic transabdominal repairs with mesh have been described. The defect in the pelvic diaphragm can be obliterated either with suturing of remaining muscle tissue or by using autogenous tissues or mesh depending on the surgeon’s expertise and local conditions, such as the lack or presence of contamination.7–11
We present 3 viable laparoscopic options for the management of internal hernias through previously placed reinforcing mesh, depending on patient-specific conditions: 1) hernia reduction with removal of original mesh without any further intervention if the pelvic floor appears well healed and intact; 2) hernia reduction with mesh removal followed by technically improved placement and fixation of new mesh in noncontaminated pelvis with weak pelvic floor; and 3) hernia reduction, resection of compromised bowel and removal of original mesh followed by suture of bladder or vagina to presacral fascia in cases with possible contamination.
Although not yet scientifically scrutinized, several issues need to be considered when contemplating reinforcing the pelvic floor after a laparoscopic or robotic procedure, such as APR. One consideration is whether reinforcing is really necessary in a particular case. It might just be that in cases with a shallow, somewhat supported pelvic floor, the benefits of not performing any additional reinforcement could outweigh possible complications, such as internal hernias and infection. With respect to our series, the cases were pooled from 4 different surgeons with varying surgical training and who adopted the practice of placing a prophylactic mesh at different time points. No statistical risk–benefit conclusions can therefore be made based on this report alone.
As illustrated by the 4 presented cases, if one still chooses to perform a similar reinforcement, some technical details need to be considered. An option is placing a mesh much lower beyond the pelvic brim and fixing it with closely spaced tacks or sutures. This might be an option in some cases especially because this technique allows for very dense placement of anchoring material without damaging autonomic nerve structures. Complete elimination of the small bowel from the pelvis should probably be reserved for patients in whom postoperative radiotherapy is anticipated to decrease the incidence of radiation enteritis. In such cases, an alternative in the form of a silicone rubber prosthesis used to fill the pelvic cavity has also been described.20
Another point to be considered is the fact that 3 of the reported hernias in our series appeared in the anterior region. Since this area is already out of the way of major autonomic nerve structures, one can just place an emphasis on reinforcing this area.
The risk for intra-abdominal infection should be taken into account in all surgical cases where resection of the bowel is performed. Synthetic mesh was used during the initial APR surgeries as no open bowel was handled intraperitoneally. If accidental contamination of the operative field occurs during surgery, we have an even lower threshold to avoiding the use of a mesh altogether or we use a biological mesh.
Finally, there is an issue of placing drains. Although this issue has not been systematically studied in this setting, most surgeons tend to leave a deep pelvic drain. If personal practice is to place a transabdominal drain through a reinforcing mesh, the surgeon must realize that such a drain could leave a potential site for an internal hernia. If a decision is made to leave a deep pelvic drain, we would therefore recommend that the drain be placed transgluteally rather than transabdominally.
Conclusion
In no way do we advocate routine use of a mesh for prevention of a perineal hernia. The goal of our review was to generate further discussion on the topic and to allow others to learn from our mistakes.
Footnotes
↵* These authors contributed to this work equally.
The information in this report was presented at the Canadian Association of General Surgeons (CAGS) annual conference held in Calgary, Alta., Sept. 13–16, 2012. Ideas generated during the presentation have been incorporated in this report.
Competing interests: None declared.
Contributors: All authors designed the study. G. Melich and D. Lim acquired and analyzed the data, which N. Kim also analyzed. G. Melich, D. Lim, G. Arena and P. Gordon wrote the article, which all authors reviewed and approved for publication.
- Accepted October 21, 2015.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.