


Abstract
Background: Trauma is a leading contributor to the burden of disease in Canada, accounting for more than 15 000 deaths annually. Although caring for injured patients at designated trauma centres (TCs) is consistently associated with survival benefits, it is unclear how travel time to definitive care influences outcomes. Using a population-based sample of trauma patients, we studied the association between predicted travel time (PTT) to TCs and mortality for patients assigned to ground transport.
Methods: Victims of penetrating trauma or motor vehicle collisions (MVCs) in Nova Scotia between 2005 and 2014 were identified from a provincial trauma registry. We conducted cost distance analyses to quantify PTT for each injury location to the nearest TC. Adjusted associations between TC access and injury-related mortality were then estimated using logistic regression.
Results: Greater than 30 minutes of PTT to a TC was associated with a 66% increased risk of death for MVC victims (p = 0.045). This association was lost when scene deaths were excluded from the analysis. Sustaining a penetrating trauma greater than 30 minutes from a TC was associated with a 3.4-fold increase in risk of death. Following the exclusion of scene deaths, this association remained and approached significance (odds ratio 3.48, 95% confidence interval 0.98–14.5, p = 0.053).
Conclusion: Predicted travel times greater than 30 minutes were associated with worse outcomes for victims of MVCs and penetrating injuries. Improving communication across the trauma system and reducing prehospital times may help optimize outcomes for rural trauma patients.
Injury is one of the largest public health concerns in Canada, accounting for 15 000 deaths and more than $20 billion in direct and indirect costs annually.1 In response to this substantial disease burden, trauma systems have been established to match patient needs with appropriate health facility resources.2 Preferentially triaging severely injured patients directly to specialized trauma centres (TCs) has been shown to reduce mortality.3 Although regionalization of trauma care services reduces trauma-related mortality,4 it has significant access implications because of the concentration of specialized resources in few discrete geographic locations. Distance to a TC correlates with time to definitive care, and there is evidence that shorter prehospital times are associated with increased survival.5–9
Health care access, defined as the degree of fit between patient needs and the health care system, is a relevant concept to policy-makers, as poor access may negatively impact health care utilization.10 Access has classically been distilled into 5 dimensions: availability, accessibility, accommodation, affordability and acceptability.10–12 Furthermore, access can be categorized by spatial (accessibility, availability) and non-spatial factors (affordability, acceptability, accommodation). 13 The importance of the spatial relationship between patients and health care services becomes clear when access is framed, in part, as a geographic construct. Although patient transport time can be used to analyze access to care, these times may be biased by various factors, including transport urgency and local triage practices. An alternative approach to determine the influence of geography on trauma patient outcomes is to estimate transport time from injury location to a TC using geospatial analysis.
Predicted travel time (PTT) is a measure of spatial access to definitive trauma care. Given that significant resources are invested to maintain TC readiness, understanding how PTTs influence patient outcomes may help improve the equity and efficiency of trauma care delivery by informing changes to trauma system organization.14 One Canadian study has previously shown that greater PTTs to trauma care result in lower TC utilization rates following major injury.15 Variability in PTTs to Canadian TCs has also been reported.16,17 However, the relationship between PTTs to TCs and mortality following major trauma remains unclear. The objective of our study was to evaluate the association between mortality and PTT to TCs for patients assigned to ground transport by the Emergency Health Services (EHS) system using a population-based sample of trauma patients in Nova Scotia and linking injury location with data from a provincial trauma registry.
Methods
Setting
Nova Scotia is the second most densely populated province in Canada with an average population density of 18 persons/km2.18,19 Notably, most of the population resides outside the only census metropolitan area; thus, rural traumas are commonly seen across the province. Trauma care in Nova Scotia is available at 8 level-III TCs, 1 adult level-I TC, and 1 pediatric level-I TC.17 All level- III TCs in Nova Scotia are capable of performing emergency, life-saving surgical services (e.g., trauma laparotomy). Emergency Health Services provide ground-based prehospital transport using a comprehensive network of ground ambulances. Although aeromedical transport is also available, these assets are used in fewer than 5% of scene responses and are therefore not the focus of this study. If paramedics are within 30 minutes of a level-I or level-III TC (including estimated extrication time), the patient is taken to the highest-level TC. In cases where paramedics are not within 30 minutes of a level-I or level- III TC, the destination and launch decision is made on a case-by-case basis by paramedics and air medical transport (AMT) personnel based on patient condition, response time of AMT (i.e., EHS LifeFlight), transport time by ground ambulance to the nearest emergency department (ED) compared with the nearest TC, capability of the nearest ED, and the level of care available by paramedics (present and from a possible intercepting crew).20
Study design and data collection
This observational geospatial analysis used data obtained from the Nova Scotia Trauma Registry (NSTR). The NSTR is a provincial population-based trauma registry under the Nova Scotia Department of Health & Wellness that captures demographic and clinical data on all major traumas occurring in the province.21 Emergency Health Services (or the police in cases of scene deaths) record the coordinates of the pickup location of all victims using global positioning systems (GPS). These data are abstracted into the NSTR.
We limited our study to trauma patients who were injured in a motor vehicle collision (MVC) or by a penetrating mechanism, as these are known to be time-sensitive cases requiring rapid transport to the nearest TC. All traumas with an Injury Severity Score (ISS) greater than 11 related to MVCs (ICD-10 V01 to V99) or penetrating mechanisms (ICD-10 W25, W26, W32–34, W45, X72–74, X78, X93–95, X99, Y22–24) between Jan. 1, 2005, and Dec. 31, 2013, were eligible for inclusion. Individuals who were missing GPS coordinates or whose pickup location was inconsistent with the injury location were excluded. We excluded any trauma cases that were solely air transport cases or that involved a combination of ground and air transport. All duplicate entries were removed before analysis.
The locations of TCs and the provincial road network used in the spatial analyses were obtained from a commercially available data set (CanMap, DMTI Spatial). We used commercially available geographic information system (GIS) software (ArcMap, Esri) for all geospatial analyses.
Cost distance analysis
Cost distance analyses were performed to model travel times from all points in Nova Scotia to the nearest TC. This validated method calculates the accumulated travel cost in minutes associated with travelling across a surface from any point in the study area to specified destinations (i.e., TCs). For use in these analyses, we constructed a 100 m2 gridded cost surface using the provincial road network and each road segment’s corresponding speed limit. Cells without a road were assigned a value corresponding to a travel speed of 5 km/h−1 (i.e., the average speed of walking). As prehospital transport is expected to use established road networks predominantly, other barriers, such as hydrologic features, were not incorporated into the cost surface. The final output was a continuous surface where each pixel corresponded to the time required to travel from that geographic location to the nearest TC. Further details on the model development and validation for emergency transport in Nova Scotia are discussed elsewhere.22
Predicted travel time to trauma care
Overlaying the point locations of major traumas related to MVCs or penetrating mechanisms over the cost distance outputs allowed us to estimate PTT to trauma care for a cohort of patients from the NSTR. The PTT corresponding to the point location of each injury was extracted from the cost distance outputs and incorporated into the statistical models.
Statistical model building
Logistic regression models of mortality risk among penetrating trauma victims and MVC-related trauma victims were estimated using time to TC care (< 10 minutes [reference], 10–20 minutes, 20–30 minutes, > 30 minutes), age (continuous), sex (female [reference], male), socioeconomic status (SES; high SES [reference], low SES), and ISS (continuous) as covariates. All covariates were defined a priori based on previously identified associations. We defined SES using the Vancouver Area Neighbourhood Derivation Index (VANDIX) of the patient’s residential location.23 For cases where residential postal codes were unavailable, injury location was used as a proxy for place of residence. The most deprived quintile was defined as low SES. The outcome of interest was death, either in-hospital or before arrival. Bivariate comparisons were performed using the Student t test or χ2 test, where appropriate. Adjusted analyses were performed, including and excluding scene deaths, to better delineate potential impacts of postinjury care on observed associations. Scene deaths included patients who died from their injuries before the arrival of police or EHS as well as patients who died at the scene while being cared for by EHS. Spatial autocorrelation of model residuals was excluded using the Global Moran’s I statistic. We performed a sensitivity analysis of PTTs only to level-I TCs in Nova Scotia (i.e., excluding level-III TCs) to evaluate the consistency of observed results. Statistical analyses were performed using Stata software version 14 (StataCorp).
Results
Selection and characteristics of the study population
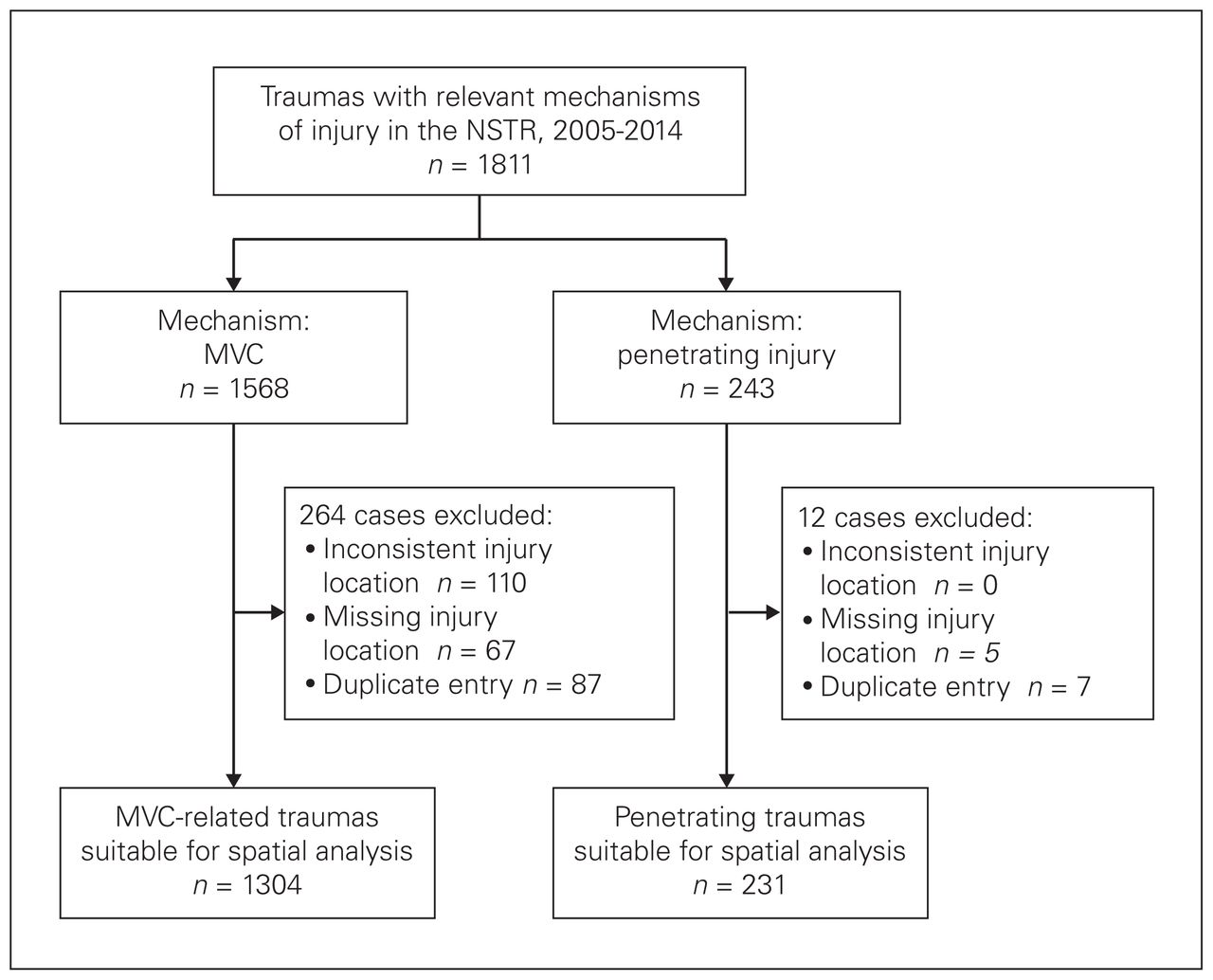
Between Jan. 1, 2005, and Dec. 13, 2013, a total of 1568 MVC-related traumas and 243 penetrating traumas were eligible for inclusion. Excluded from this study were 1675 major traumas from all other mechanisms. Following the exclusion of duplicates and entries with missing or inconsistent injury locations, 1304 cases of MVC-related trauma and 231 cases of penetrating trauma remained for spatial analysis (Fig. 1). All TCs were successfully geolocated. Most MVC-related traumas (64.0%) and penetrating injury cases (57.0%) occurred in locations outside of Halifax Regional Municipality, which is the sole urban area in the province.

Selection of study participants. MVC = motor vehicle collision; NSTR = Nova Scotia Trauma Registry.
The general characteristics of the study population are described in Table 1. Victims of both injury mechanisms were predominantly young and male. Among victims of penetrating injuries, 67.0% of trauma cases were related to firearms, while the rest were caused by sharp objects, most commonly knives. Mortality among patients injured in MVCs was 25.0%, compared with 56.3% in patients with penetrating trauma. In both groups, patients who died had a higher mean ISS, and a greater proportion of these patients had low SES.
Characteristics of patients with MVC-related or penetrating traumas
Predicted travel time to trauma care in Nova Scotia via ground transport
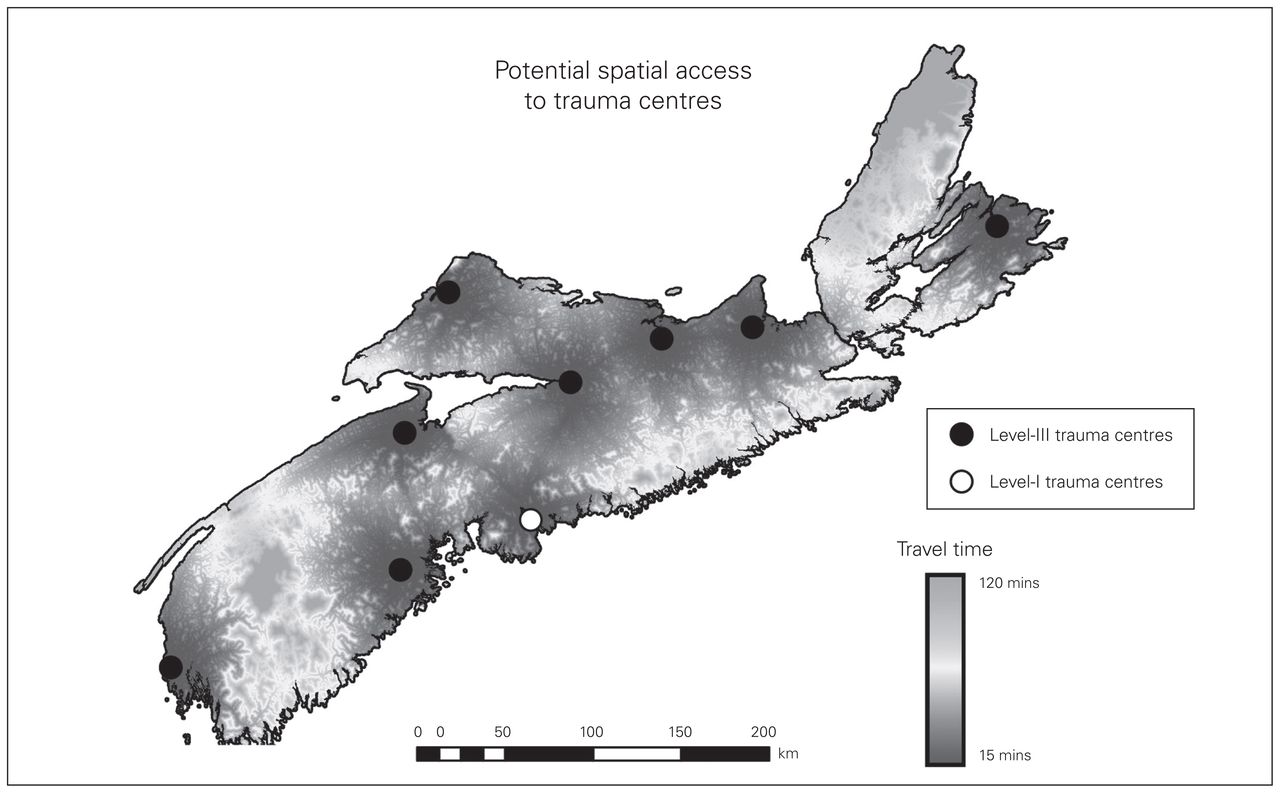
The cost distance analysis of ground-based travel time to trauma care in the province of Nova Scotia is illustrated in Figure 2. This analysis showed regional variation in TC accessibility, but most points in the province were found to have access to a TC within 30 minutes of driving time. Overall, 29.7% of MVC-related traumas were located more than 30 minutes away from a TC (median time to TC 19.3 minutes), and 26.8% of penetrating traumas were located more than 30 minutes away from a TC (median time to TC 15.3 minutes).

Results of cost distance analysis showing predicted travel times to trauma care in Nova Scotia.
Comparison of trauma cases by predicted driving time from a trauma centre
Using bivariate analyses, we compared the characteristics of patients with MVC-related and penetrating traumas who were located 30 minutes or less of PTT from a TC with those of patients located more than 30 minutes away (Table 2). For MVC-related traumas, the unadjusted mortality was higher for individuals injured more than 30 minutes away from a TC (30.2/100 persons v. 22.8/100 persons, p = 0.005). Pre-, post- and on-scene intervals were all higher in the group injured more than 30 minutes away from a TC (all p < 0.001). The probability of scene death was also higher for individuals injured more than 30 minutes away from a TC (20.9% v. 12.2%, p < 0.001). Finally, individuals injured more than 30 minutes away from a TC were 52% more likely to be ejected from the vehicle (p < 0.001).
Patient characteristics and predicted travel time to a trauma centre
For penetrating traumas, the unadjusted mortality was significantly higher for individuals injured more than 30 minutes away from a TC (75.8/100 persons v. 49.1/100 persons, p < 0.001). Individuals injured more than 30 minutes away from TCs were also more likely to be older, to experience longer prehospital intervals, and to have low SES (all p < 0.01).
Influence of predicted travel time to trauma care on mortality
We conducted logistic regression analyses to determine the influence of PTT to trauma care on mortality (Table 3). Among patients with MVC-related traumas, lack of PTT to TC care within 30 minutes was found to be associated with a 66% increased risk of death after adjustment for the confounding variables of age, sex, ISS and SES identified a priori (odds ratio [OR] 1.66, 95% confidence interval [CI] 1.09–2.52, p = 0.018). Importantly, this association was lost when scene deaths were excluded from the analysis (OR 0.93, 95% CI 0.58–1.46, p = 0.78,). In addition, the likelihood of death in these patients was associated with male sex (OR 1.45, p = 0.034), increasing age (OR 1.02, p < 0.001), and increasing ISS (OR 1.11, p < 0.001).
Logistic regression analysis on influence of predicted travel time on mortality
In cases of penetrating trauma, a PTT greater than 30 minutes from a TC was associated with increased likelihood of death (OR 3.43, 95% CI 1.37–8.59, p = 0.039). Notably, after scene deaths were excluded from the analysis, this association remained and approached significance (OR 3.48, 95% CI 0.98–14.5, p = 0.053). Risk of death was also associated with increasing age (OR 1.06, p < 0.001) and increasing ISS (OR 1.07, p < 0.001) in these patients. Results were similar following a sensitivity analysis of PTTs only to level-I TCs in the province. There was no difference in the likelihood of death between patients taken to a level-I TC and those transported to a level-III TC.
Discussion
Owing to the high prevalence of rural trauma in Canada, it is important to understand the impact of trauma care accessibility on the outcomes of injured patients. By combining spatial analyses with more traditional statistical models, our study shows that trauma patients injured in areas with higher PTTs to TCs have increased risk of death. The magnitude of this association and the potential explanations underlying it are modified by the mechanism of injury. Greater likelihood of ejection following MVCs in more remote areas suggests that behavioural patterns, such as seatbelt use, may be at least partly responsible for this association. In cases of penetrating trauma, higher PTTs to trauma care also increased the risk of death, and this association remained following exclusion of scene deaths, suggesting that differences in postinjury care or prolonged postscene transport times may explain this result. Patients injured in areas with poorer access to trauma care were more likely to experience longer prehospital intervals; thus, reducing prehospital times for patients injured in remote locations may improve their outcomes.
In Nova Scotia, prehospital time depends on triage practices as well as transport urgency and is therefore an inherently biased variable. In our data set there was an inverse relationship between recorded prehospital time and probability of survival for MVC victims, providing evidence that analyzing prehospital time alone is inadequate for complex trauma systems. Access is an independent variable determined exclusively by injury location and the location of TCs. As such, geospatial analysis is a superior way to study the influence of geography on patient outcomes than using actual transport times. To serve system decision-makers better, our method of analysis could be adapted to focus on subpopulations with specific needs and timelines to care, such as patients with traumatic brain injuries.24
It has been demonstrated consistently that caring for injured patients in a designated TC is associated with higher survival rates.5,25 Accordingly, field triage guidelines have been developed that stipulate that an injured patient should be transported directly to a designated TC irrespective of its proximity to the injury location.26 Several studies have identified significant survival benefits in trauma patients with shorter prehospital times.5–9 Longer prehospital times are typical for rural trauma patients,27–29 suggesting a potential disadvantage for those injured in remote areas, which is consistent with our results. In contrast to our findings, however, some have found that prehospital time has no effect on patient mortality,30 while others report decreased overall mortality as the prehospital time interval increased.31 In their comparison of rural and urban trauma patients in Oregon and Washington, Newgard and colleagues32 found that mortality was not significantly different for rural and urban patients; however, a greater proportion of rural deaths occurred shortly after injury. Prehospital time may be more important for certain subgroups of trauma patients. In a systematic review of 20 studies, Harmsen and colleagues9 found that shorter prehospital intervals conferred survival benefits only for patients with central nervous system injuries and hemodynamically unstable patients injured by penetrating mechanisms, presumably because of the high prevalence of life-threatening surgical lesions in these populations. Importantly, Brown and colleagues33 showed that not all prehospital time is equal. The authors reported increased risk of death in patients with prolonged scene time, while prolonged response time and transport time were not associated with mortality. Furthermore, Roisilen and colleagues34 showed that the estimated effect of transport time to hospital care varies depending on the choice of statistical model.
Few Canadian studies have examined the impact of PTTs to trauma care on patient outcomes. Lawson and colleagues17 reported increased unadjusted mortality for patients injured more than 60 minutes of driving time from level-I or level-II trauma care. Although the authors used residential postal codes as a surrogate for injury location, this surrogate could be inaccurate in trauma systems dominated by blunt mechanisms.35 In addition, the unadjusted nature of the statistical analysis limited their ability to elucidate any potential explanatory or confounding factors underlying their findings. This is important, given the potential for individuals injured in rural locations to have additional risk factors, such as lower SES or more severe injuries, for adverse outcomes.29,36 Some of the first trauma-related spatial analyses that incorporated multivariable statistical models were conducted by Crandall and colleagues37 in urban Chicago. After adjusting for several relevant confounding variables, the authors reported that victims of firearm-related penetrating trauma had 23% increased odds of death if they were injured farther than 5 minutes of PTT from a TC. However, the urban setting and specific population of this study provides little generalizability to a rural trauma system.
Minimizing the time interval between injury and provision of definitive care, a concept popularized as the “golden hour,” has been a central tenet of postinjury care for decades.38 Several studies have reported improved survival for rural trauma patients transported by air compared with ground transport,39,40 including 2 previous studies performed in Nova Scotia.41,42 While EHS Life-Flight is able to land at or near the scene of an emergency, this occurs relatively infrequently, which is why we limited our analysis to ground transport. At the time of the study, EHS LifeFlight did not autolaunch; these services had to be requested by ground paramedics. As early activation of EHS LifeFlight is critical to getting the patient to definitive care, better communication across the trauma system may improve patient outcomes. Outcomes could also be improved by having advanced paramedics on rural EHS services. Finally, increased educational efforts may improve outcomes in rural trauma cases. The Rural Trauma Team Development Course (RTTDC) is based on the concept that in most situations, rural facilities can form a trauma team consisting of at least 3 core members,43 and there is evidence that participation in RTTDC can significantly improve prehospital times.44,45 In Nova Scotia, the provincial trauma program (Trauma Nova Scotia) began offering RTTDC in 2012. Further research is warranted to determine whether implementation of RTTDC training in Nova Scotia has had an effect on outcomes in rural trauma patients.
Limitations
Our study has several limitations. First, it is subject to the known limitations of retrospective data collection. The accuracy of injury location data collected by EHS has not been externally validated and relies on personnel manually indicating when they arrive on scene. There is, however, an available field that denotes the reliability of the coordinates, which helped to avoid the inclusion of inaccurate data in the analysis. Second, the analysis was limited to data from a single provincial trauma system. Although the epidemiology of injuries in Nova Scotia is comparable to that in other provinces, systemic differences in postinjury care remain possible; thus, our results will need to be replicated in a geographically and politically distinct region. Third, patients who required transport from the scene by EHS LifeFlight were excluded from the analysis. These patients tend to be more severely injured and would likely benefit the most from rapid transport times. It should be noted that the TC-level designations did not change over the study period, but it is likely that there were a number of major trauma care advances (both pre-hospital and in-hospital) during this time. Finally, residual confounding by unidentified factors is possible, though unlikely, as there was no spatial autocorrelation of the model residuals.
Conclusion
In our study of cases of MVC and penetrating injury assigned to ground transport by the EHS system, we found that injury in a location with a PTT greater than 30 minutes to a TC was associated with poor patient outcomes. Efforts to improve communication within the trauma system and reduce prehospital time may improve outcomes for patients injured in remote locations.
Acknowledgements
Data used in this research were made available by Trauma Nova Scotia at the Nova Scotia Department of Health and Wellness. Any opinions expressed by the authors do not necessarily reflect the opinions of the Nova Scotia Department of Health and Wellness or Trauma Nova Scotia.
Footnotes
Competing interests: None declared.
Contributors: G. Tansley, N. Schuurman, M. Bowes, M. Asbridge and N. Yanchar designed the study. G. Tansley acquired and analyzed the data, which N. Schuurman, M. Erdogan, R. Green and M. Asbridge also analyzed. G. Tansley, M. Erdogan and M. Asbridge wrote the article, which all authors reviewed and approved for publication.
- Accepted August 28, 2018.
References

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.