


Abstract
Background: Laparoendoscopic single site (LESS) surgery may have perceived benefits of reduced visible scarring compared to conventional laparoscopic (LAP) totally extraperitoneal (TEP) hernia repairs. We reviewed the literature to compare LESS TEP inguinal hernia repairs with LAP TEP repairs.
Methods: We searched electronic databases for research published between January 2008 and January 2012.
Results: A total of 13 studies reported on 325 patients. The duration of surgery was 40–98 minutes for unilateral hernia and 41–121 minutes for bilateral repairs. Three studies involving 287 patients compared LESS TEP (n = 128) with LAP TEP (n = 159). There were no significant differences in operative duration for unilateral hernias (p = 0.63) or bilateral repairs (p = 0.29), and there were no significant differences in hospital stay (p > 0.99), intraoperative complications (p = 0.82) or early recurrence rates (p = 0.82). There was a trend toward earlier return to activity in the LESS TEP group (p = 0.07).
Conclusion: Laparoendoscopic single site surgery TEP hernia repair is a relatively new technique and appears to be safe and effective. Advantages, such as less visible scarring, mean patients may opt for LESS TEP over LAP TEP. Further studies with clear definitions of outcome measures and robust follow-up to assess patient satisfaction, return to normal daily activities and recurrence are needed to strengthen the evidence.
Inguinal hernias are a common problem and concern in the population with more than 80 000 new diagnoses1 leading to more than 70 000 repairs between 2010 and 2011 in the UK;2 20 million repairs are performed worldwide every year.3,4 Open inguinal hernia repairs are well-established procedures5 with good postoperative outcomes. Since the early 1990s6,7 laparoscopic techniques have become more popular. Some studies report an increase from 6% in 1992 to more than 40% in 2008 of hernias being repaired laparoscopically;8 this rapid rise in use may be because of less pain, faster recovery and better long-term outcomes.9–11 Furthermore, the minimally invasive procedures (typically the transperitoneal approach, but also the extraperitoneal approach if the midline raphe is crossed) offer the ability to examine the contralateral side,12 which may reveal an incipient or obvious hernia in up to 20% of patients.13,14 The proportion of laparosopic repairs has increased markedly over the last 20 years.15 The 2 recognized types of laparoscopic approaches are totally extraperitoneal preperitoneal (TEPP) or transabdominal preperitoneal (TAPP). Although both techniques are safe16 and offer advantages, totally extraperitoneal (TEP) repairs may be associated with a lower incidence of port site hernias, bowel-related complications, less pain and greater patient satisfaction; conversely, TEP may be associated with an increased likelihood of conversion.17–19
Greater patient education and demand for better cosmesis after surgical procedures have led to increased interest in laparoendoscopic single site surgery (LESS). Initially there was reluctance to adopt the technique owing to lack of technical facilitation; however, new or innovative port types20 and newer instruments have led to its application in a variety of surgical specialities.21 Laparoendoscopic single site TEP may be performed using conventional instruments, although articulating or curved instruments are in use.22 Although patients have good outcomes after conventional laparoscopic techniques, some authors suggest that there is a preference for LESS,23 which may be because of less postoperative pain24,25 or possible better cosmesis. Some have argued there is no advantage to single port surgery.26 We hypothesized that LESS TEP may be superior to conventional laparoscopic TEP (LAP TEP) because of fewer incisions, which may lead to less pain, and because the single incision in the umbilicus may result in a hidden scar with a better cosmetic appearance.
We reviewed the literature examining the role of LESS TEP for inguinal hernias. We aimed to compare LESS TEP with LAP TEP. Our main summative outcome measures were duration of surgery, hospital stay, cosmesis and return to activity.
Methods
Searching and selection
We identified all studies examining the role of LESS TEP for hernia repairs or comparing LESS TEP with LAP TEP that were published between January 2008 and January 2012. We searched the Medline, Embase and CINAHL databases available through the National Health Service National Library of Health website, the Cochrane library and PubMed. A range of key words are available to describe LESS techniques, and we used these terms to search for relevant material.27 The main key words “single port,” “single site surgery,” “laparoendoscopic single site,” “single port access,” “single incision,” “multiport” and “totally extraperitoneal hernia repair” were used in combination with the medical subject headings “hernia” and “inguinal hernia.” Articles, reviews and meta-analyses that we considered irrelevant based on the titles and abstracts were excluded. Relevant articles referenced in these publications were obtained, and we searched the references of identified studies to identify any further studies. No language restriction was applied.
Quality assessment
Two authors (M.R.S.S. and M.K.) independently assessed the methodological quality of the trials included for meta-analysis using standardized reference tools.28–31
Data extraction
Articles were included according to our review criteria (all noncomparative studies reporting on LESS TEP, all studies comparing LESS TEP with LAP TEP for groin hernias, all comparative or randomized studies, all elective cases, trials involving adults of any sex) and were reviewed by 2 researchers (M.R.S.S. and M.K.). This was performed independently, and if any conflict arose resolution was through discussion with the authors prior to analysis. Only papers examining the role of LESS TEP for hernias in adults and studies comparing LESS TEP with LAP TEP were included.
Our main outcome measures were duration of surgery for unilateral and bilateral hernias, hospital stay, complications, pain and concerns raised at follow up.
Statistical analysis
Statistical analyses were performed using Review Manager 5.0.23 (RevMan; Cochrane Collaboration).32 A value of p < 0.05 was chosen as the significance level for outcome measures. For continuous data (duration of surgery, hospital stay, return to activity), the inverse variance method was used for the combination of standardized mean differences (SMD). Binary data (intraoperative complications and recurrence) were summarized as risk ratios (RR) and combined using the Mantel–Haenszel method.33 Heterogeneity of the studies was assessed according to Q and I2 statistics. We used a random-effects method if the heterogeneity was significant; otherwise a fixed-effects method was used. In a sensitivity analysis, 1 was added to each cell frequency for trials in which no event occurred, according to the method recommended by Deeks and colleagues.34 When standard deviations were not reported, we estimated them either from ranges or p values. Forest plots were used for the graphical display.
Results
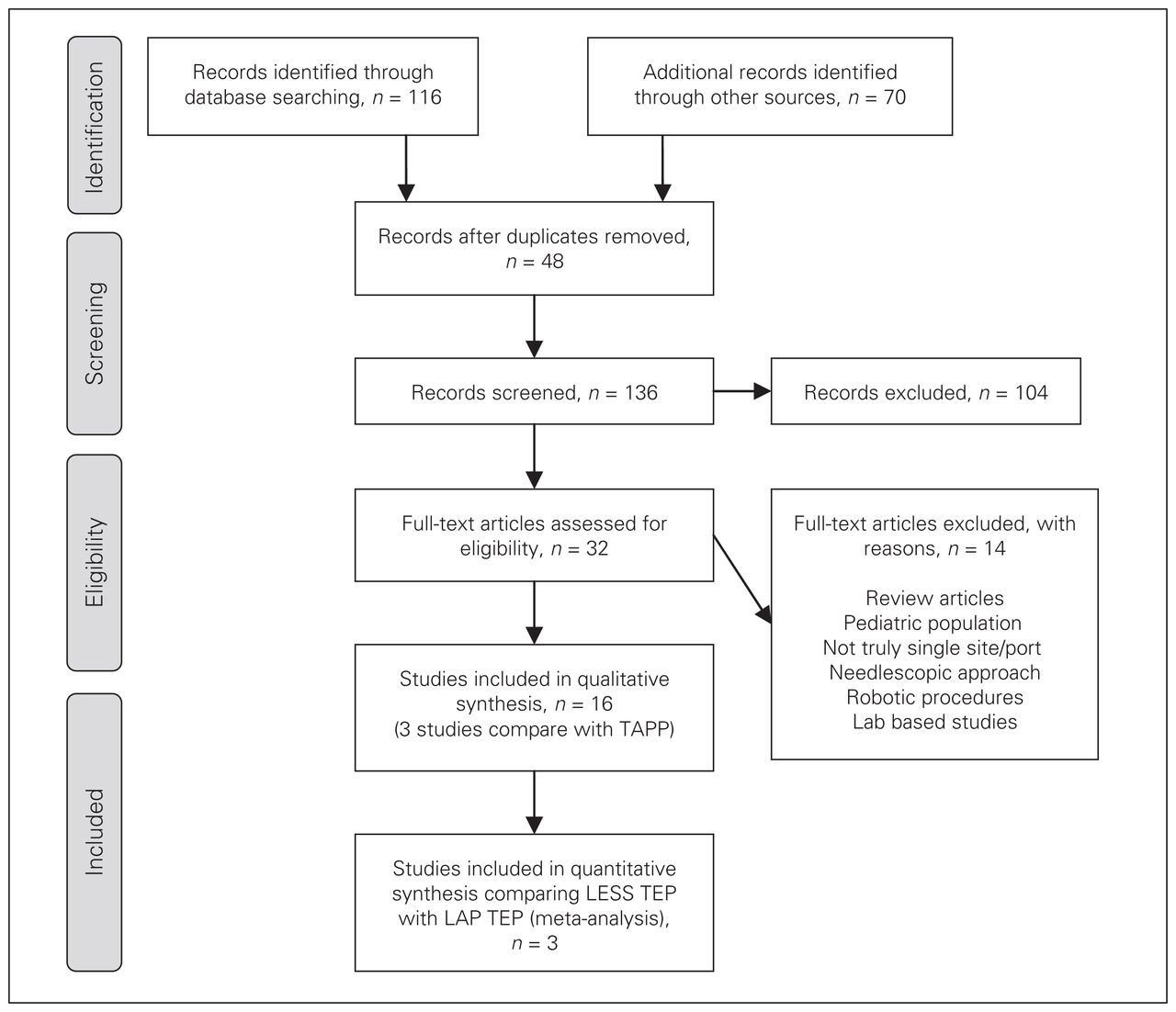
A total of 136 articles were screened for relevance. On further scrutiny, 16 articles15,19,22,35–47 were used in our literature review and 3 studies comparing LESS TEP with LAP TEP were found to have useful data for the summative outcome. One study commented on a previous report.37 Three studies22,40,45 compared LESS TEP with LAP TEP and were combined to produce a summative outcome. A flow chart of the literature search according to PRISMA guidelines48 is shown in Figure 1. Characteristics of each article are given in Tables 1 and 2.
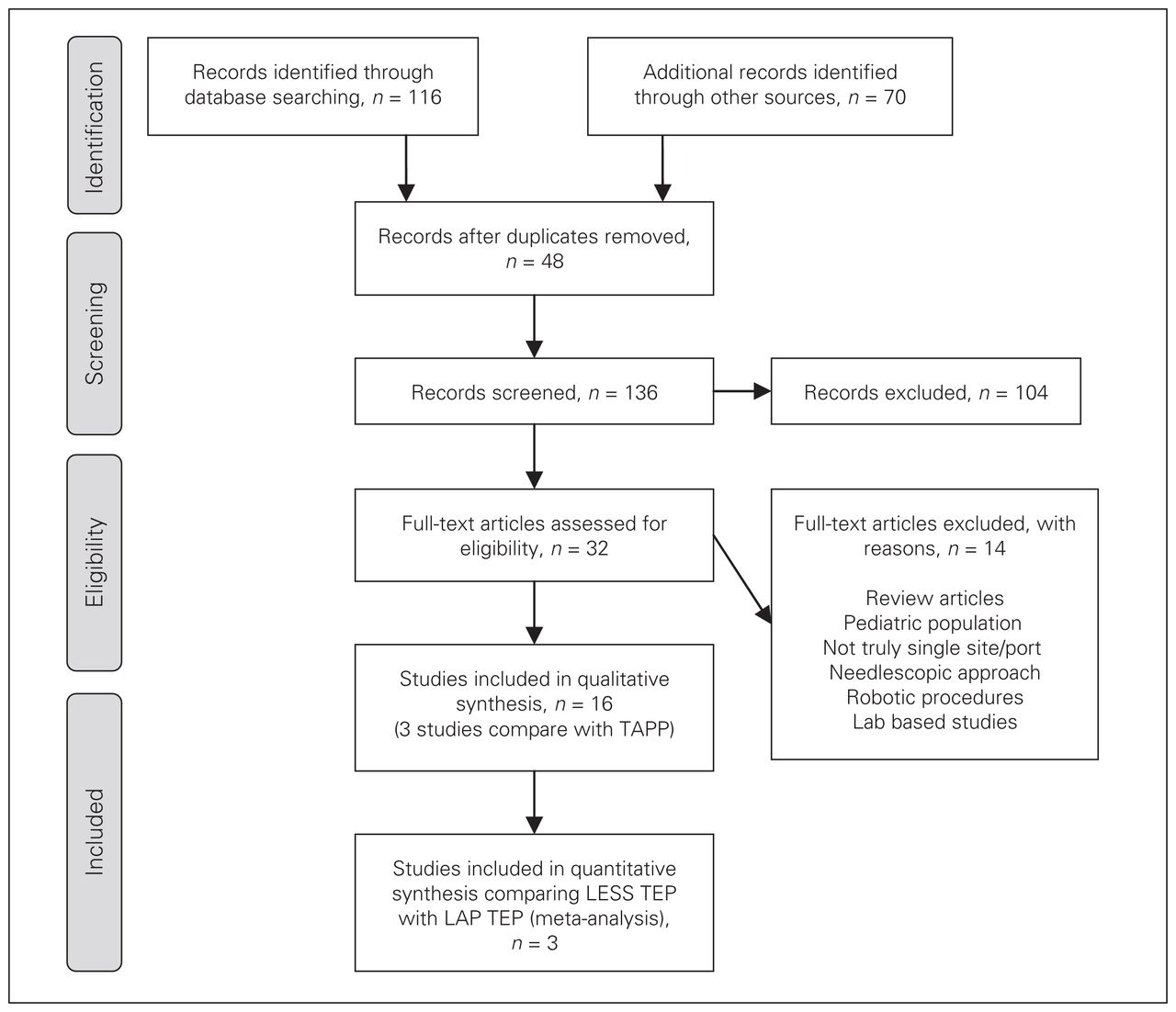
Study selection. LAP = laparoscopic; LESS = laparoendoscopic single site surgery; TAPP = transabdominal preperitoneal; TEP = totally extraperitoneal.
Characteristics of studies included in our review and meta-analysis
Characteristics of studies comparing LESS TEP with LAP TEP
Demographic characteristics of patients undergoing LESS TEP
Thirteen studies15,19,35–39,41–44,46,47 reported on 325 patients undergoing the LESS TEP procedure. The patient age range was 18–85 years,15,19,35,37–39,41–44,46 and 90% of patients were men.15,19,35,37–39,41–43,46
Surgical technique
Nine studies reported on the use of a balloon to create a preperitoneal space.15,19,35,37,38,41,42,44,47 Seven studies used a single port access device.15,19,36,38,39,41,43 Other techniques included the use of 3 ports through a single incision.35,37,42,44,46,47 A range of 0–45° cameras and straight, curved, articulating or manually bent instruments were used.15,19,35–39,41–44,46,47 Two studies36,43 did not report their mesh fixation method and 1 did not use any form of fixation.19
Outcomes after the LESS TEP approach
Perioperative data
The mean duration of surgery was 40–98 minutes for unilateral hernia repairs15,19,35–37,39,41,42,44,46,47 and 41–121 minutes for bilateral hernia repairs.15,36,38,39,41–44,46,47 Six patients required conversion, although no conversions were to a formal open procedure.15,36,41,42,46 There were only 2 reported intraoperative complications involving bleeding or a peritoneal tear.36,42 Hospital stay ranged from less than a day to 2.15 days.15,19,35,37–39,41–44,46,47 Postoperative recovery was uneventful all but 7 patients: seroma developed in 5 patients, 1 went into ileus and 1 experienced urinary retention).42,44,46,47
Follow-up
Follow-up ranged from 2 weeks to 14 months. Patients reported only minimal discomfort or ache.15,39,42,43 There were only minor complications: epididymitis, wound infection, dehiscience and seroma/hematomas.39,42 Two studies reported on return to activities after a range of 5–14 days.15,42 There were no recurrences reported up to 14 months after the operation.15,19,36,38,39,41–43,47
Comparison with LAP TEP approach
Three studies22,40,45 reported on a total of 128 patients in the LESS TEP group and 159 in the LAP TEP group.
Duration of surgery
Unilateral hernia repairs
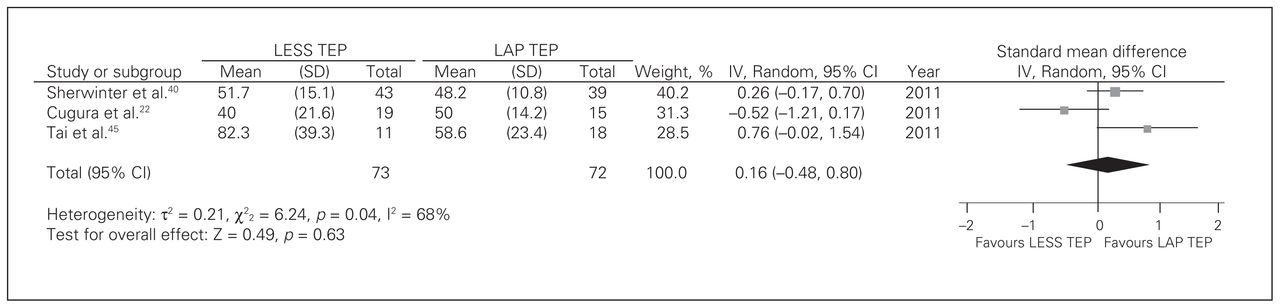
Three studies22,40,45 contributed to a summative outcome. There was significant heterogeneity among trials (Q2 = 6.24, p = 0.040, I2 = 68); therefore the fixed-effects model was inappropriate. There was no difference in duration of surgery between LESS TEP and LAP TEP (random-effects model: SMD = 0.16, 95% confidence interval [CI] −0.48 to 0.80, z = 0.49, p = 0.63; Fig. 2).
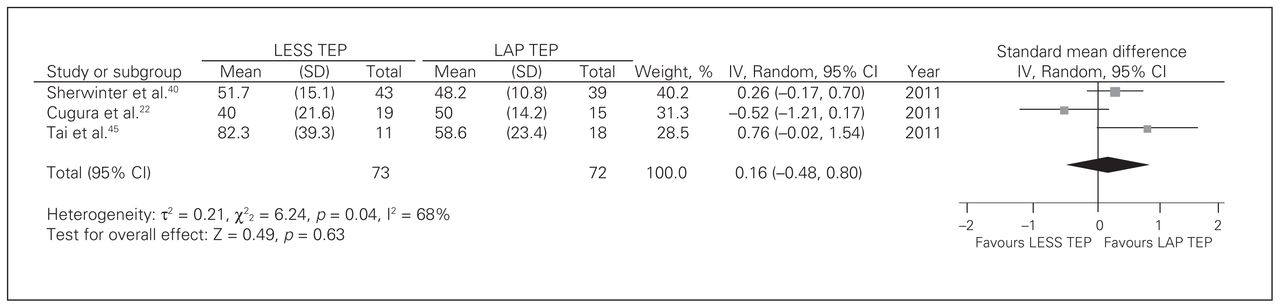
Duration of surgery for unilateral hernias. CI = confidence interval; IV = inverse variance; LAP = laparoscopic; LESS = laparoendoscopic single site surgery; SD = standard deviation; TEP = totally extraperitoneal.
Bilateral hernia repairs
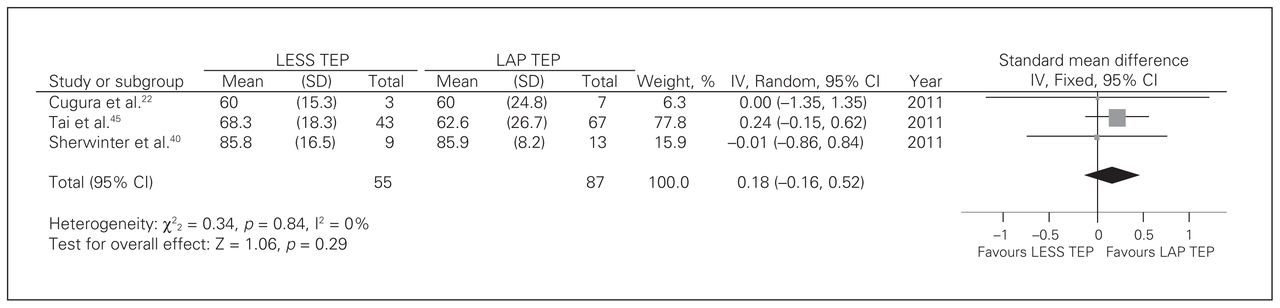
Three studies22,40,45 contributed to a summative outcome. There was no significant heterogeneity among trials (Q2 = 0.34, p = 0.84, I2 = 0). There was no difference in duration of surgery between LESS TEP and LAP TEP (fixed-effects model: SMD = 0.18, 95% CI −0.16 to 0.52, z = 1.06, p = 0.29; Fig. 3).
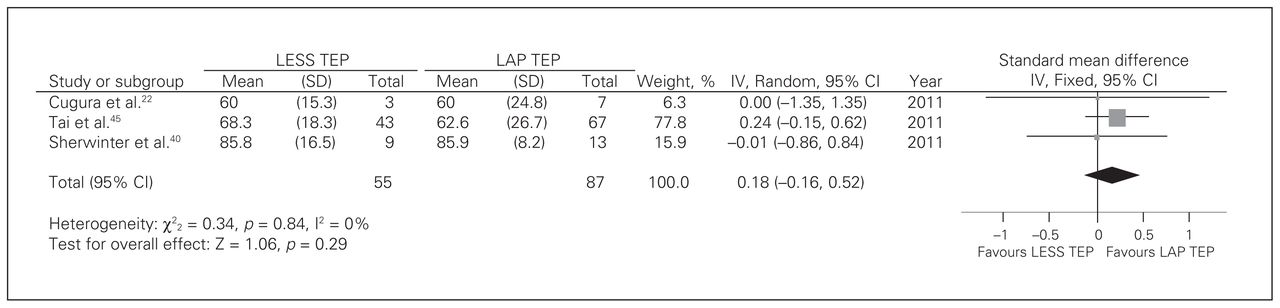
Duration of surgery for bilateral hernias. CI = confidence interval; IV = inverse variance; LAP = laparoscopic; LESS = laparoendoscopic single site surgery; SD = standard deviation; TEP = totally extraperitoneal.
Hospital stay
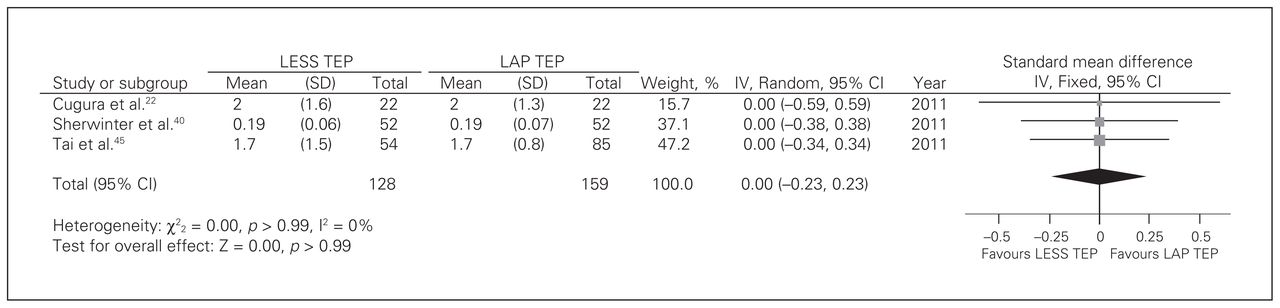
Three studies22,40,45 reported on hospital stay. There was no significant heterogeneity among trials (Q2 = 0.00, p > 0.99, I2 = 0). There was no difference between groups [fixed-effects model: SMD = 0.00, 95% CI −0.23 to 0.23, z = 0.00, p > 0.99; Fig. 4).
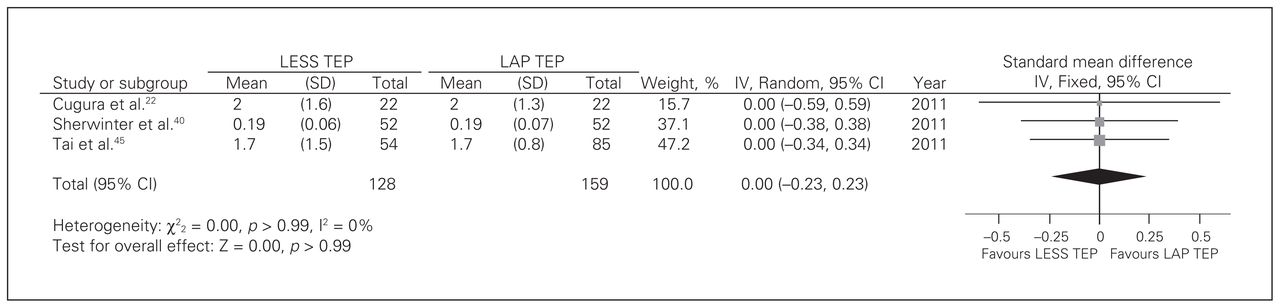
Hospital stay. CI = confidence interval; IV = inverse variance; LAP = laparoscopic; LESS = laparoendoscopic single site surgery; SD = standard deviation; TEP = totally extraperitoneal.
Intraoperative complications and conversions
There was no significant heterogeneity among trials (Q1 = 0.05, p = 0.82, I2 = 0). There was no difference between techniques according to the studies included22,45 (fixed-effects model: RR = 1.25, 95% CI 0.18–8.51, z = 0.23, p = 0.82). None of the patients required conversions.22,40,45
Cosmesis and follow-up
The length of the incision in the umbilicus was similar in both techniques (1.5–2 cm);22,45 however, the total length of all incisions was slightly less in the LESS TEP group than the LAP TEP group (2 cm v. 3.5 cm, respectively).22 This difference did not appear to translate into less satisfaction in the LAP TEP group.45
One study40 reported 5 and 6 minor complciations in the LAP TEP and LESS TEP groups, respectively. There were 4 patients with seromas and 1 patient with bladder dysfunction after LAP TEP, and there were 3 patients with seromas and 3 with bladder dysfunction after LESS TEP.
Pain
Only 1 study45 reported on pain. After 24 hours, there appeared to be no difference between techniques; however, after 1 week patients who underwent LESS TEP had significantly less pain. One study40 reported on analgesic use, and although patients undergoing LESS TEP required painkillers for less time than those in the LAP TEP group, the difference was not significant.
Return to activity
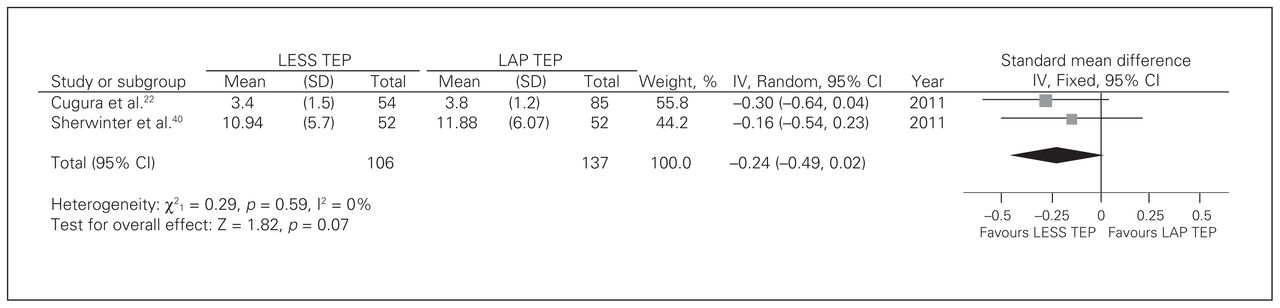
Two studies22,40 reported on return to activity. There was no significant heterogeneity among trials (Q1 = 0.29, p = 0.59, I2 = 0). Patients in the LESS TEP group restarted activity earlier, and this difference approached statistical significance (fixed-effects model: SMD = −0.16, 95% CI −0.49 to 0.02, z = 1.82, p = 0.07; Fig. 5).
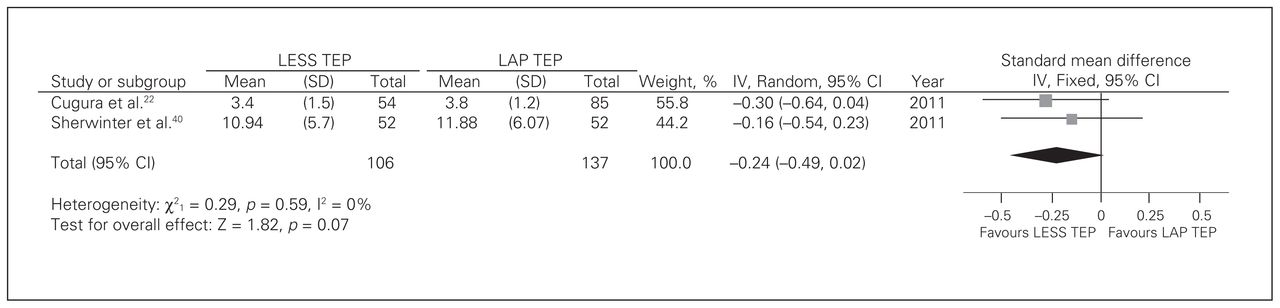
Return to activity. CI = confidence interval; IV = inverse variance; LAP = laparoscopic; LESS = laparoendoscopic single site surgery; SD = standard deviation; TEP = totally extraperitoneal.
Discussion
The nature of surgery has led to developments in techniques to reduce the postoperative stress response and improvement in cosmesis. These include robotic laparoscopy, natural orifice translumenal endoscopic surgery (NOTES) and, increasingly, minimally invasive and LESS surgery.49,50 One of the main challenges to robotic surgery is cost;51 NOTES may be unacceptable to certain groups of patients, whereas LESS may be the most preferred approach.23
Main findings
This paper examined the role of LESS TEP for inguinal hernia repairs and compared it with LAP TEP. Duration of surgery for unilateral and bilateral repairs showed a great variation but appeared comparable to conventional TEP performed by surgeons on different points of their learning curve.52,53 The conversion rate was low (0.02%) and no conversions were to a formal open technique; surgeons preferred to convert to TAPP or add further ports. Postoperative recovery was largely uneventful, and very few complications were noted. No recurrence was noted up to 14 months after surgery, and most patients returned to activity within 2 weeks.
Formal comparison with LAP TEP showed no significant difference in duration of surgery, hospital stay, intraoperative complications, conversions or recurrence. The LESS TEP procedure had a slightly smaller total incision length than LAP TEP. There are equivocal results in relation to pain and analgesic requirements. There was a trend for patients in the LESS TEP group to return to activity earlier, but the difference did not achieve statistical significance (p = 0.07); this result is consistent with the literature showing faster recovery in other settings.54
Importance
The importance of these findings is that for patients with inguinal hernias, a range of safe and effective options is available and may be used to treat dual pathologies.55 Furthermore the LESS technique may offer patients the ability to return to activity earlier, which may be especially important for those who are self-employed.56 This article also suggests that current evidence is strong enough to warrant further trials to establish the role of this technique. Although some articles suggest cosmesis may be better with LESS TEP, LAP TEP is an acceptable technique with good postoperative outcomes.57
Appraisal of evidence
Owing to investment in newer or different instruments or ports, some suggest that LESS techniques are more expensive than conventional laparoscopic techniques; however, recent studies have shown comparability between the 2 techniques.58,59 There is a learning curve associated with LESS techniques; however, it may not be as steep as initially perceived60,61 and depends on a number of factors, including the type of port used for access.62 Nonetheless, experienced surgeons ought to perform or supervise these procedures to ensure adequate training. Furthermore, in the initial stages there may be a higher rate of postoperative complications until such time that the learning curve has reached a plateau.63 Technical challenges include access,64 poor triangulation and lack of space leading to instrument clash,65 which may be overcome by the use of 30° cameras.22 Instrument control may also be less intuitive.41 One disadvantage to LAP TEP is that if complications arise conversion to either LAP TAP or open surgery may be the only options, whereas with LESS TEP conversion to conventional LAP TEP is also an option.
Future advances include robotic surgery; however, recent studies have shown similar durations of surgery, and although remote operating is a definite advantage, costs may be prohibitive.51
From a patient perspective, single incision surgery is more appealing presumably owing to potential cosmetic benefits; however, this should be in the context of an appropriate safety profile.66 The cosmetic concern may be greater in children, with recent studies showing good outcomes.67,68 One factor regarding cosmesis is the position of the scar, with some reports suggesting an intraumbilical or crescenteric incision giving the best outcomes.15,22
Heterogeneity
The literature varied greatly in terms of specifics involved with the LESS TEP technique. In our literature review, some authors used a balloon15,19,35,38,41,42,44,47 to create the preperitoneal space, whereas others used blunt dissection.25,39,43,46 A range and combination of straight or curved and articulating instruments and 0°–45° cameras were used. Only 1 study reported no mesh fixation.19
In our pooled analysis comparing LESS TEP with LAP TEP, there was significant heterogeneity in the duration of surgery for unilateral repairs. This may be related to slightly different technique variations and differences in learning curve. This finding is in keeping with the lack of heterogeneity in duration of bilateral repair, reflecting progression in the number of procedures performed. However, most of the included studies did not state where the bilateral hernias were in relation to their learning curve. There was no significant heterogeneity in relation to hospital stay, recurrence, intraoperative complications or return to activity, which probably reflects similar clinical and follow-up protocols among the centres. Although there was no significanct heterogeneity, there were some clinical differences in the type of technique used (Table 2). For example, some authors used a homemade port,45 some used different cameras and 1 group did not fix the mesh in all patients.22 Only 1 study reported the type of analgesics used and their discharge protocols.40 The activities to which patients returned were not clearly identified, and convalescence may have been very different depending on age, sex and type of employment.56 Other limitations to our study include the use of assessments of the papers according to set criteria. Although this may give an indication to the strength of the study, it may not highlight potential weaknesses, including detailed differences that were not documented in the studies, such as site of pain (umbilical v. pubic due to tacks) or sequelae of complications.
The degree of clinical heterogeneity means firm conclusions for practice need to be made with caution.
Quality assessment
We did not formally assess the quality of the studies included in our initial review. This was generally because of the small numbers in the series and because of the relative paucity of studies in the literature. In our early meta-analysis there was only 1 study22 that stated it was a randomized controlled trial of moderate quality; however, the study did not detail sample size calculations, allocation concealment or analysis based on intention to treat, which may lead to significant bias in reporting outcomes. Furthermore, this same trial did not specifically state it was double-blind. The remaining 2 studies were comparative studies, and 1 was a comparison with a historical cohort, which presents inherent weaknesses. One study45 did not report inclusion or exclusion criteria; the other study40 did not state clearly their diagnostic criteria or identify standardized outcome forms. It is too early to comment on publication bias.
Future studies
Further prospective randomized studies focusing on cosmesis, postoperative pain, analgesic requirements and return to activity are required to assess whether LESS TEP has an advantage over LAP TEP.69 Clear definitions of pain and return to activity should be given with examination of the type of job conducted, as it may be that LESS TEPP may benefit particular groups of workers. Studies should consider the learning curve of the surgeon to ensure appropriate comparisons with LAP TEP in relation to duration of surgery and hospital stay. Our review highlights the need for a multicentre randomized controlled trial with appropriate follow up.
Conclusion
The LESS TEP hernia repair is a relatively new technique and appears to be safe and effective. Advantages, such as less visible scarring, mean patients may opt for LESS TEP over LAP TEP. Further studies with clear definitions of outcome measures and robust follow up to assess patient satisfaction, return to normal daily activities and recurrence are required to strengthen the evidence.
Footnotes
Competing interests: None declared.
Contributors: M.R.S. Siddiqui, M. Kovzel, O. Priest, S.R. Preston and Y. Soon designed the study. M.R.S. Siddiqui and M. Kovzel acquired the data, which M.R.S. Siddiqui, M. Kovzel and S. Brennan analyzed. M.R.S. Siddiqui and M. Kovzel wrote the article, which all authors reviewed and approved for publication.
- Accepted May 21, 2013.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools





