


Abstract
Background: Occupational injuries and hazards have gained increased attention in the surgical community in general and in the orthopedic literature specifically. The aim of this study was to assess prevalence and characteristics of musculoskeletal disorders among orthopedic trauma surgeons and the impact of these injuries on the surgeons’ practices.
Methods: We sent a modified version of the physical discomfort survey to surgeon members of the Orthopaedic Trauma Association (OTA) via email. Data were collected and descriptive statistics were analyzed.
Results: A total of 86 surgeons completed the survey during the period of data collection; 84.9% were men, more than half were 45 years or older and 40.6% were in practice for 10 years or more. More than 66% of respondents reported a musculoskeletal disorder that was related to work; the most common was low back pain (29.3%). The number of body regions involved and disorders diagnosed was associated with increasing age and number of years in practice (p = 0.033). Time off work owing to these disorders was associated with working in a private setting (p = 0.045) and working in more than 1 institute (p = 0.009).
Conclusion: To our knowledge, our study is the first to report a high percentage of orthopedic trauma surgeons sustaining occupational injuries some time in their careers. The high cost of management and rehabilitation of these injuries in addition to the related number of missed work days indicate the need for increased awareness and implementation of preventive measures.
Occupational injuries and hazards have gained increased attention in the surgical community in general and in the orthopedic literature specifically. Different aspects of occupational hazards have been investigated, including radiation, chemical, psychological and musculoskeletal injuries. The orthopedic surgical environment has been the main culprit behind most of these hazards.1 A 25-fold increase in thyroid cancer incidence in spine surgeons has been reported and is most likely attributed to the increased exposure to radiation.2 In addition, polymethylmethacrylate cement, which has been in use in orthopedics since the 1950s, has been shown to have toxic effects on the skin and on the respiratory and nervous systems.3 Also, smoke inhalation from electrocautery causes greater exposure than second-hand smoking.4 Psychologically, loss of sleep and work demands were found to have a detrimental effect on the emotional health of physicians.5,6
Orthopedic surgeons work in an environment that puts a high demand on their bodies, especially the musculoskeletal system. Repetitive movements while using tools, prolonged standing and operating in sustained and nonergonomic positions all contribute to this increased load on the bones and muscles.1 Studies have shown increased incidence of musculoskeletal complaints in orthopedic surgeons compared with other specialists.7 Most of the complaints included the neck, back and upper extremities.7 Although guidelines for a more ergonomic environment in the operating room are available, lack of awareness and difficulty applying these guidelines contribute to their ineffectiveness.8–10
One of the orthopedic specialties with increased workload on the musculoskeletal system is orthopedic trauma. In a study by Davis and colleagues,11 who examined the prevalence and impact of musculoskeletal injuries on orthopedic surgeons in general, it was highlighted that orthopedic trauma surgeons had a higher rate of injuries than other specialists, but owing to the small number of trauma surgeons among their respondents this subgroup could not be analyzed.
In the present study, we assessed the musculoskeletal injury data from a survey of orthopedic trauma surgeons in North America and examined the impact of these injuries on the surgeons’ practices.
Methods
Survey
After review board approval, a modified version of the physical discomfort web-based anonymous survey was posted on the Orthopaedic Trauma Association (OTA) website, and we sent a link to the survey to the OTA’s 595 active surgeon members via email. The first email was sent in July 2014, and a reminder email was sent in October 2014. The survey was closed in December 2014 and data collection commenced.
The web-based survey was divided into the following sections: demographics (age, sex and hand-dominance), type of institution, average number of cases per year and number of years in practice. Musculoskeletal disorders were classified according to body region (neck, shoulder, elbow/forearm, wrist/hand, hip, knee, foot/ankle and low back). In each section participants were asked about diagnosis, treatment required (if any) and time off work required. This survey was piloted among 20 volunteers to assess length, ease of navigation and comprehensibility.
Statistical analysis
Data were collected and descriptive statistics were analyzed. For data analysis, we performed a-way analysis of variance (ANOVA) and Fisher exact tests, as appropriate, to compare the variables. We considered results to be significant at p < 0.05.
Results
Participant demographics and descriptive data
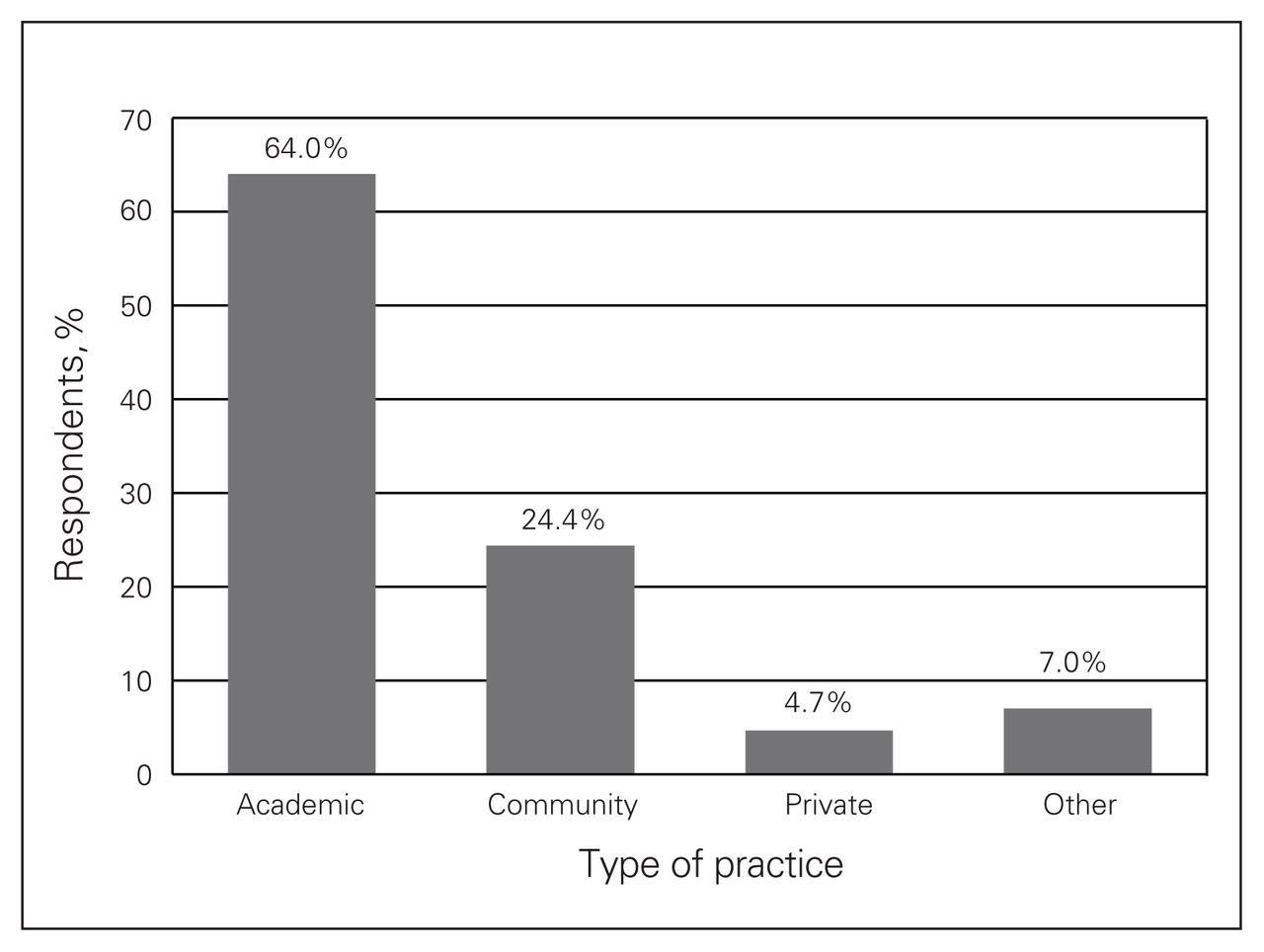
A total of 86 surgeons completed the survey during the period of data collection, resulting in a response rate of 14.5%. Of the respondents, 84.9% were men and more than half were 45 years or older (Table 1 and Fig. 1). The majority of respondents had been in practice for 10 years or longer and worked in academic institutions (Fig. 2 and Fig. 3). Of note, 5.9% of respondents worked in more than 1 institution. Overall, 66.7% of responding surgeons reported a work-related musculoskeletal disorder, of which 26.7% required time off work because of their injuries (Fig. 4, Table 2 and Table 3).
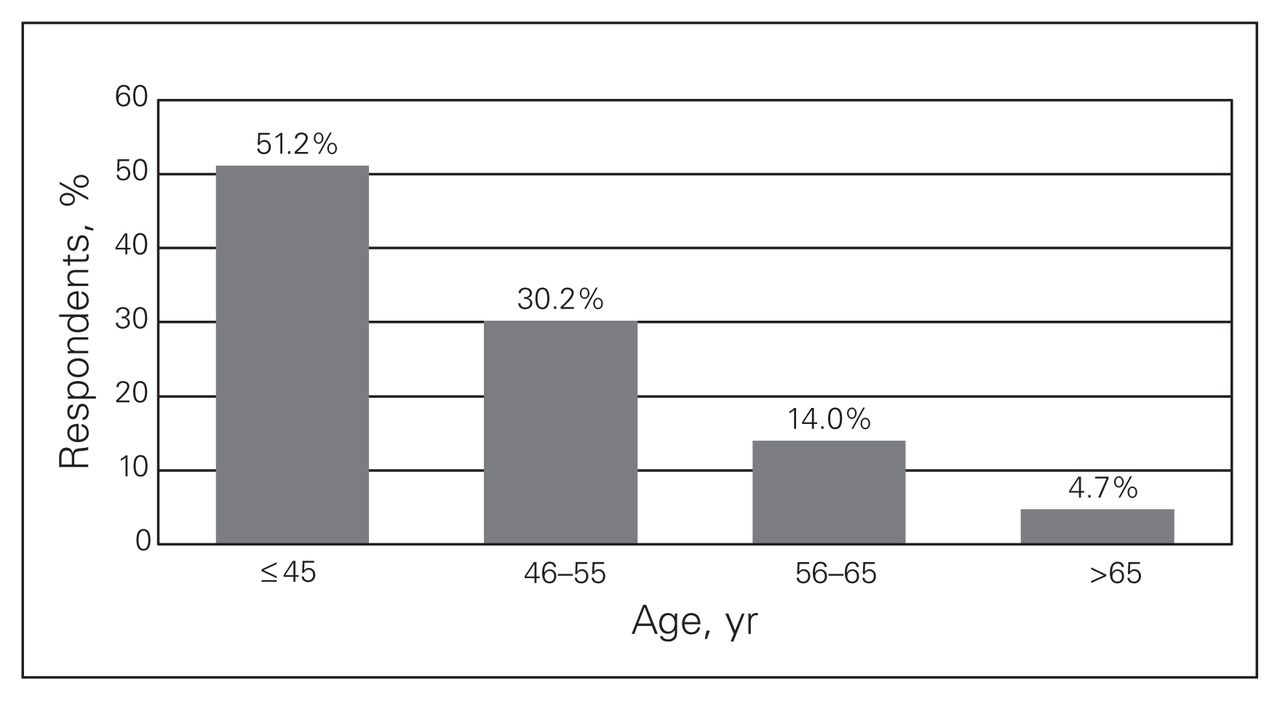
Age distribution among survey participants.
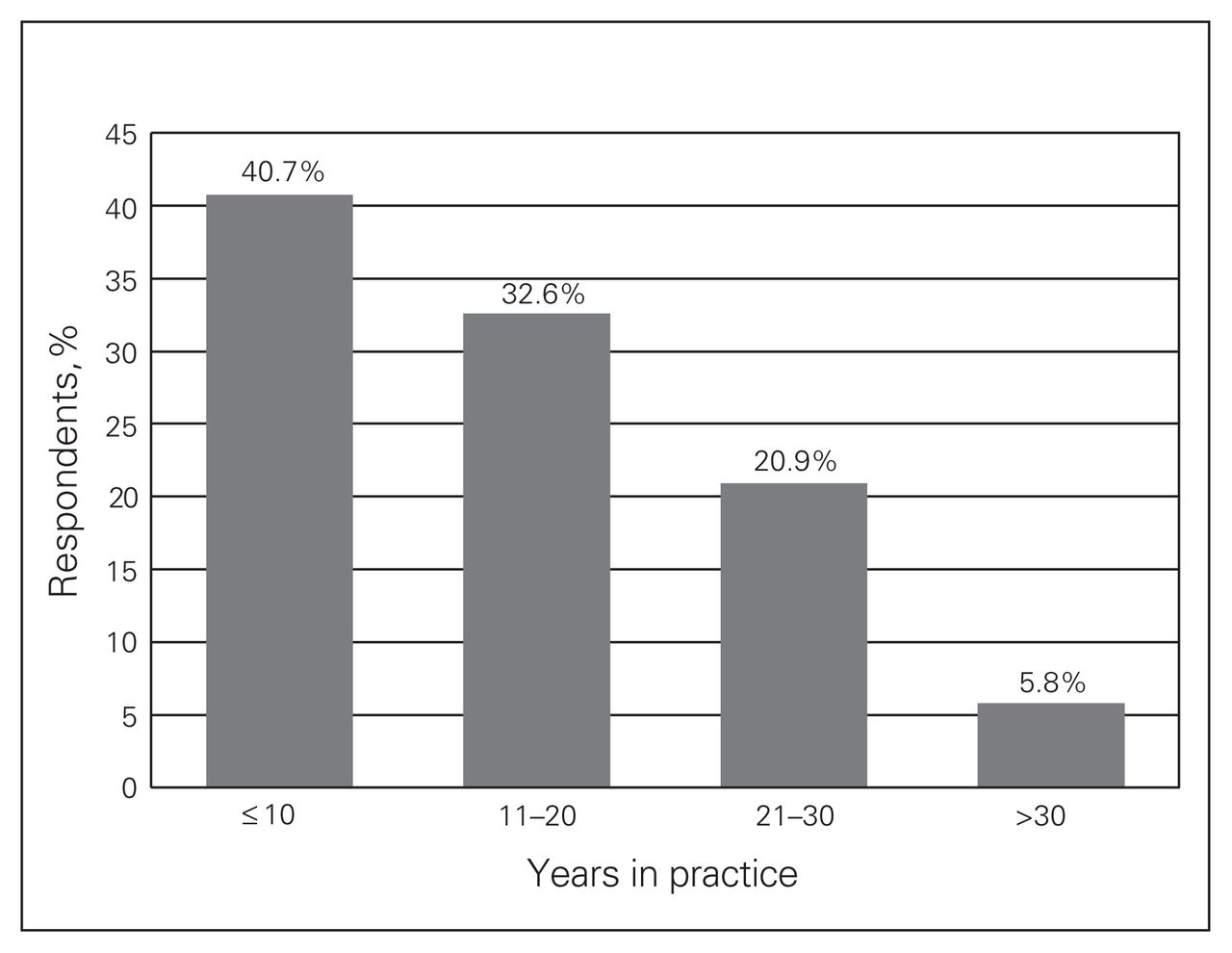
Distribution of years in practice among survey participants.
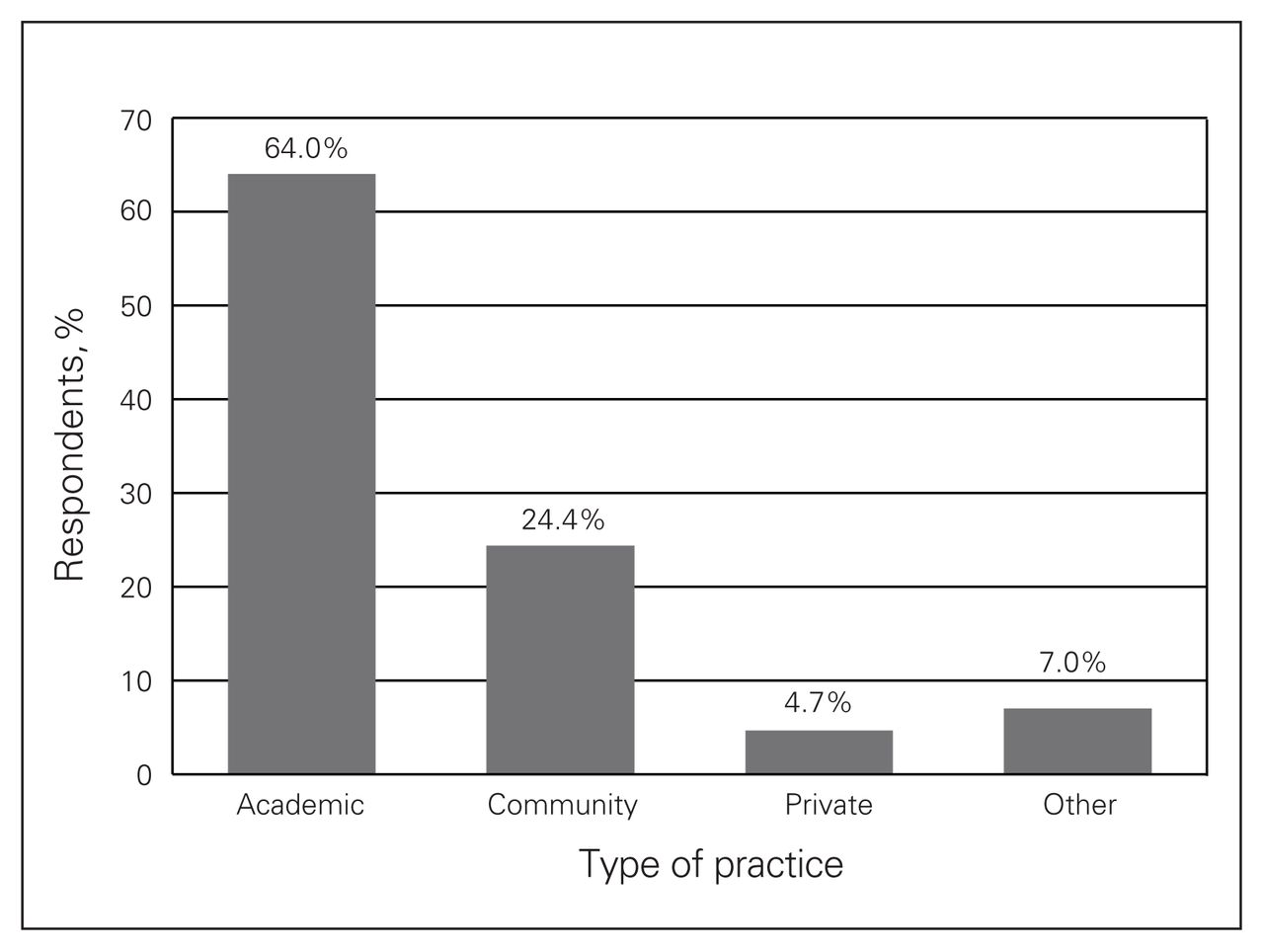
Distribution of type of practice among survey participants.
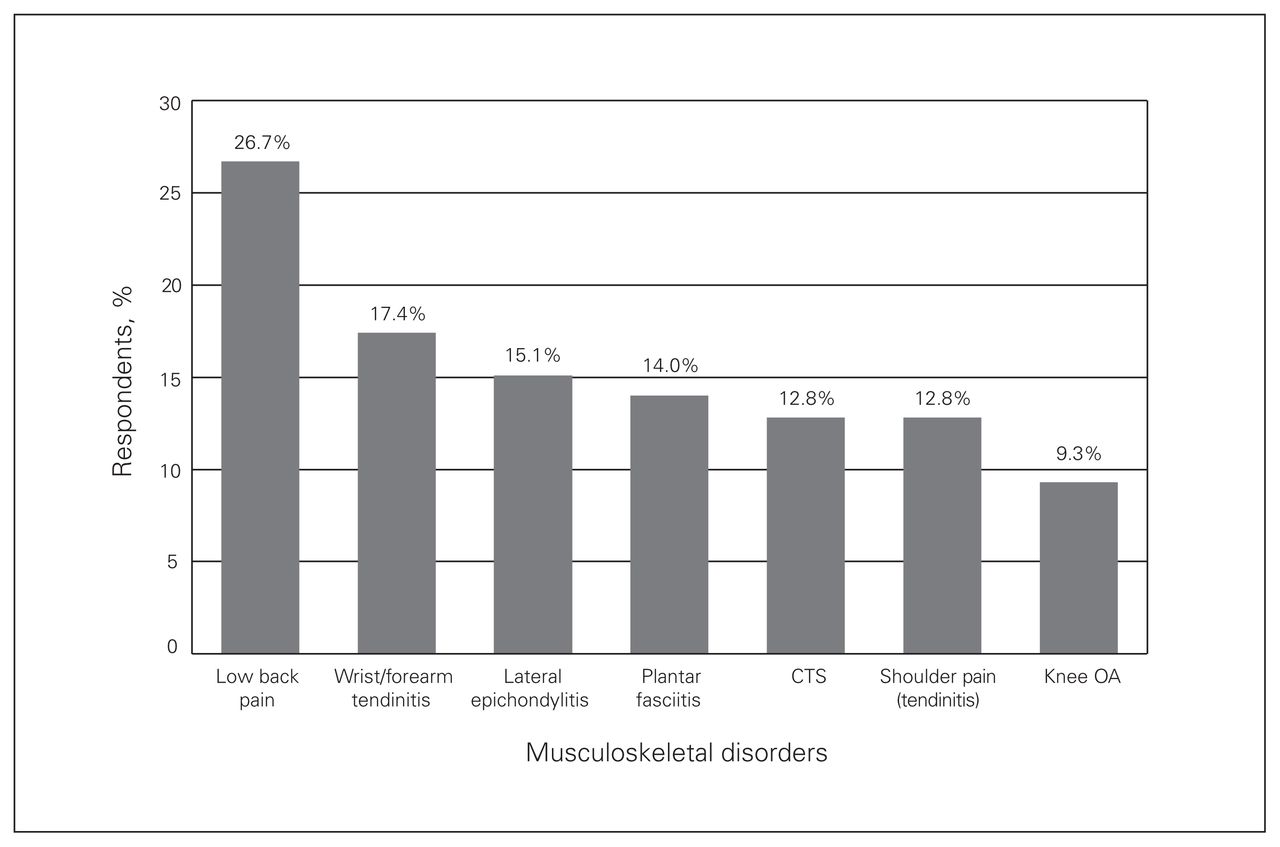
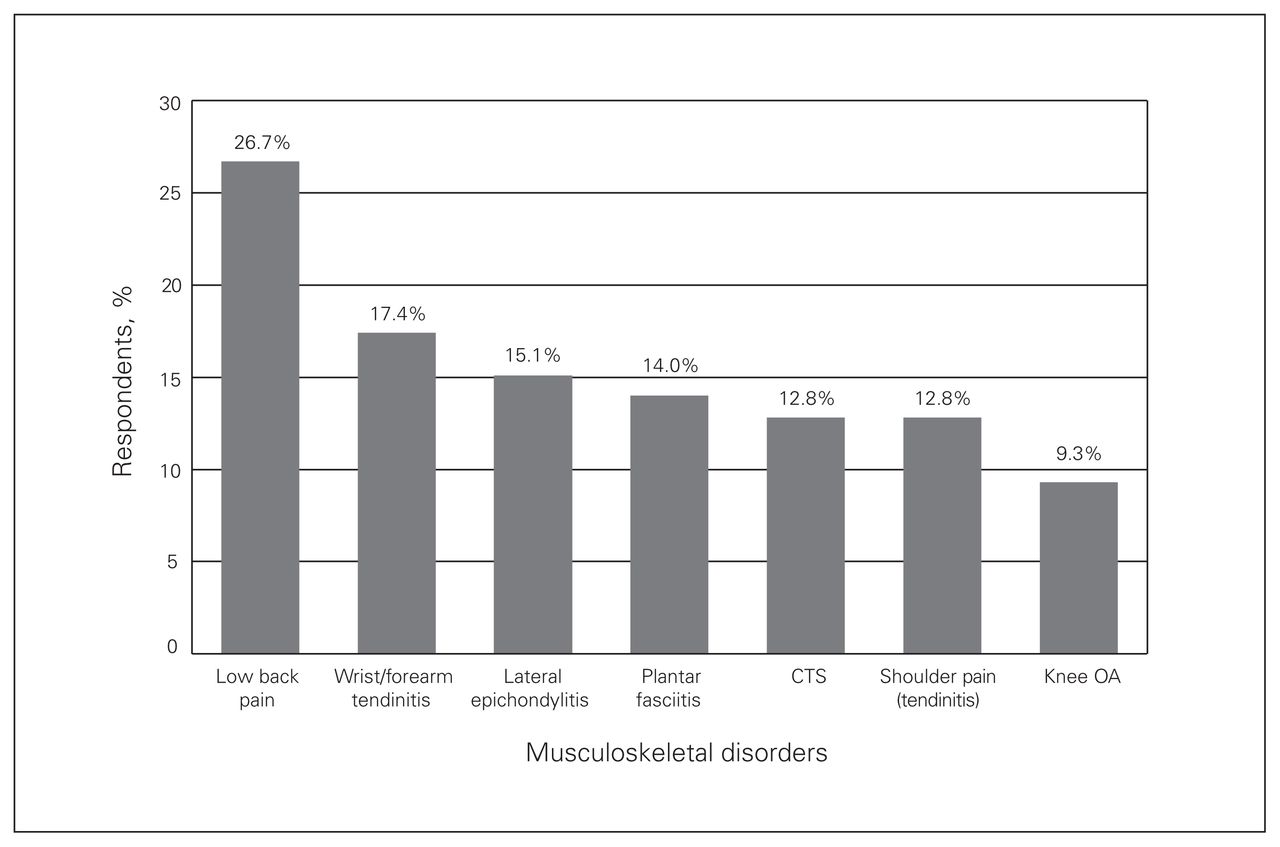
Musculoskeletal disorders and complaints among survey participants. CTS = carpal tunnel syndrome; OA = osteoarthritis.
Sex and hand dominance of surveyed trauma surgeons (n = 86)
Number of surveyed trauma surgeons with disorders and their requirement of time off work according to sex, age, hand dominance, type of practice and number of institutions
Number of surveyed trauma surgeons with disorders and their requirement of time off work according to annual case load and number of years in practice
Area injured
The majority of musculoskeletal complaints and disorders were low back pain (26.7%), wrist or forearm tendinitis (17.4%), elbow lateral epicondylitis (15.1%), plantar fasciitis (14.0%), carpal tunnel syndrome (12.8%), shoulder pain or tendinitis (12.8%) and knee osteoarthritis (9.3%) (Fig. 1). Varicose veins (5.9%), inguinal hernia (4%), hearing problems (4%) and cataracts (2.6%) were the most commonly reported non-musculoskeletal disorders.
Sex, age and hand dominance
The sex of the surgeon was not associated with the number of disorders or regions involved; however, increasing age of the surgeon was associated with an increased number of body regions involved (p = 0.033). Neither the sex nor the age of the surgeons surveyed showed a significant association with the presence of a disorder or with requiring time off work because of the disorder. Interestingly, right-handed surgeons were more likely to report the presence of at least 1 musculoskeletal disorder (p = 0.034; Table 2).
Type of practice
When a musculoskeletal disorder was diagnosed, surgeons working in a private setting (p = 0.009) and surgeons working in more than 1 institute (p = 0.009) were significantly more likely to require time off work. Conversely, the surgeons’ type of practices had no influence on the presence of a disorder, the number of disorders, or the regions involved (Table 2).
Annual caseload
The surgeons’ caseload per year was not associated with the presence of a disorder, the number of disorders, the regions involved, or the need for time off work (Table 3).
Years in practice
When data were grouped according to number of years in practice, the results showed a significant difference between the groups. Being in practice more than 10 years was associated with an increased number of regions involved (p = 0.045). Years in practice did not influence the surgeons’ need for time off work, nor did it have an effect on the presence of a disorder (Table 3).
Number of disorders and regions involved
Our results showed that both an increased number of regions involved (p < 0.001) and an increased number of musculoskeletal disorders (p < 0.001) were independently associated with a greater likelihood of surgeons needing time off work.
Discussion
A number of studies in the surgical literature have identified an increased prevalence of occupational injuries in surgeons in general and specifically in orthopedic surgeons.7,11,12 Davis and colleagues11 found a 44% prevalence of injuries in surveyed orthopedic surgeons, with orthopedic trauma surgeons reporting more injuries than the other subspecialists.11 The same was true in our study, with a 65% prevalence of injuries among the respondents. The most commonly injured areas in all subspecialists reported by Davis and colleagues11 were the hand, low back, neck and shoulder, whereas in a study by Auerbach and colleagues12 involving spine surgeons low back and neck pain were the most commonly reported injuries. This group also reported a high prevalence of shoulder, elbow and wrist injuries.12 In our study of orthopedic trauma surgeons, the most commonly reported injured region was the low back, followed by the wrist, elbow and foot. This resemblance among studies in reported injuries can be attributed to the surgeons’ tendency toward prolonged periods of standing and sustaining constant positions (bending the head and back), especially during lengthy surgeries, thus exposing the neck and low back to increased mechanical stress. In addition, the use of repetitive movements when operating instruments and tools may have a role in increased prevalence of upper limb tendinitis, especially of the elbow and the wrist.13 Forst and colleagues14 reported an increased prevalence (up to 3 times) of carpal tunnel syndrome in surgeons who frequently use a Kerrison rongeur.14
In the study by Davis and colleagues11 there was a higher prevalence of musculoskeletal disorders in surgeons who had been in practice for 20–30 years, whereas Auerbach and colleagues12 found no such association. Our results revealed no association between number of years in practice and reporting of an injury; however, we found that the number of regions involved increased when a surgeon was in practice for more than 10 years.
Surprisingly, the surgeons’ age and caseloads had no association with the prevalence of a musculoskeletal injury in our study or in previously conducted surveys.11,15 Interestingly, in our study we found that right-handed surgeons were more likely to report an injury and that surgeons in a private setting were more likely to require time off work because of their disorders.
Our results indicate that attention should be directed toward making the operating room more surgeon-friendly in terms of more ergonomically safe postures and movements. Improvements can include using body support, taking stretch breaks, using the microscope rather than surgical loops (more neutral neck position) and using power to insert long screws, to name a few.1,12,16 More research is required to identify methods of improving the surgical setting and their effectiveness.
Limitations
Limitations of our study include the use of a self-reported measure, the validity and reliability of which have not been established. Recall bias is another limitation, as the disorders were surgeon-reported injuries.
Conclusion
To our knowledge, our study is the first of its kind reporting that a high percentage of orthopedic trauma surgeons sustain occupational injuries at some point in their careers. The cost of management and rehabilitation of these injuries in addition to the number of missed work days because of these injuries indicate that they have a significant economic burden on the health care system. Increased awareness may help with the early detection of these injuries and with the implementation of preventive measures.
Acknowledgements
The authors thank all the surgeons who participated in this survey and the OTA for making this study possible.
Footnotes
↵* These authors contributed equally to this work.
Competing interests: E.J. Harvey is the Chief Medical Officer of Greybox Healthcare (Montreal) and Chairman of the Board of NXT-Sens Inc. (Montreal). No other competing interests declared.
Contributors: All authors designed the study. S. AlQahtani and M. Alzahrani acquired the data, which M. Alzahrani analyzed. S. AlQahtani and M. Alzahrani wrote the article, which all authors reviewed and approved for publication.
- Accepted December 7, 2015.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.