


Abstract
Background: Knee and hip arthroplasty constitutes a large percentage of hospital elective surgical procedures. The Blaylock Risk Assessment Screening Score (BRASS) was designed to identify patients in need of discharge planning. The purpose of this study was to evaluate whether the BRASS was associated with length of stay (LOS) in hospital following elective arthroplasty.
Methods: We retrospectively reviewed the charts of individuals undergoing primary elective arthroplasty for knee or hip osteoarthritis who had a documented BRASS score.
Results: In our study cohort of 241, both BRASS (p < 0.001) and replacement type (hip v. knee; p = 0.048) were predictive of LOS. Higher BRASS was associated with older patients (p < 0.001), higher American Society of Anesthesiologists score (p < 0.001) and longer LOS (p < 0.001). We found a specificity of 83% for a BRASS greater than 8 and a hospital stay longer than 5 days and a specificity of 92% for a BRASS greater than 10.
Conclusion: The BRASS represents a novel and significant predictor of LOS following elective arthroplasty. Patients with higher BRASS are more likely to stay in hospital 5 days or more and should receive pre-emptive social work consultations to facilitate timely discharge planning and hospital resources.
Osteoarthritis (OA) is among the most common conditions affecting elderly individuals.1 As a result, hip and knee arthroplasty have become widely performed elective procedures for patients with degenerative joint disease. These relatively low-risk procedures provide patients with improved mobility, reduced pain and substantially improved quality of life. Owing to the aging population, the number of hip and knee arthroplasty procedures performed in developed countries has been increasing steadily over the past decade.2 Advancements in provision of care have reduced the average length of stay (LOS) in hospital.3 However, in some cases, patients may encounter a delay in discharge. Factors that contribute to prolonged hospital stay include pre-existing medical comorbidities, unforeseen perioperative medical events and poor or unsafe discharge disposition. Unanticipated postponed discharge not only decreases efficiency, but also delays future elective procedures owing to the scarce availability of post-surgical beds. Effective discharge planning is critical to the timely discharge of patients and greatly facilitates the efficiency of hospital resource and bed management.
The need for effective discharge planning has led to a demand for an effective preoperative screening tool to identify such patients before admission. Ideally, this tool would identify patients at risk for increased postoperative LOS and allow staff to pre-emptively take measures that would facilitate a safe postoperative course and appropriate discharge destination without substantially increasing the expected postoperative LOS. This would ultimately increase the efficiency of both patient care and hospital resource allocation.
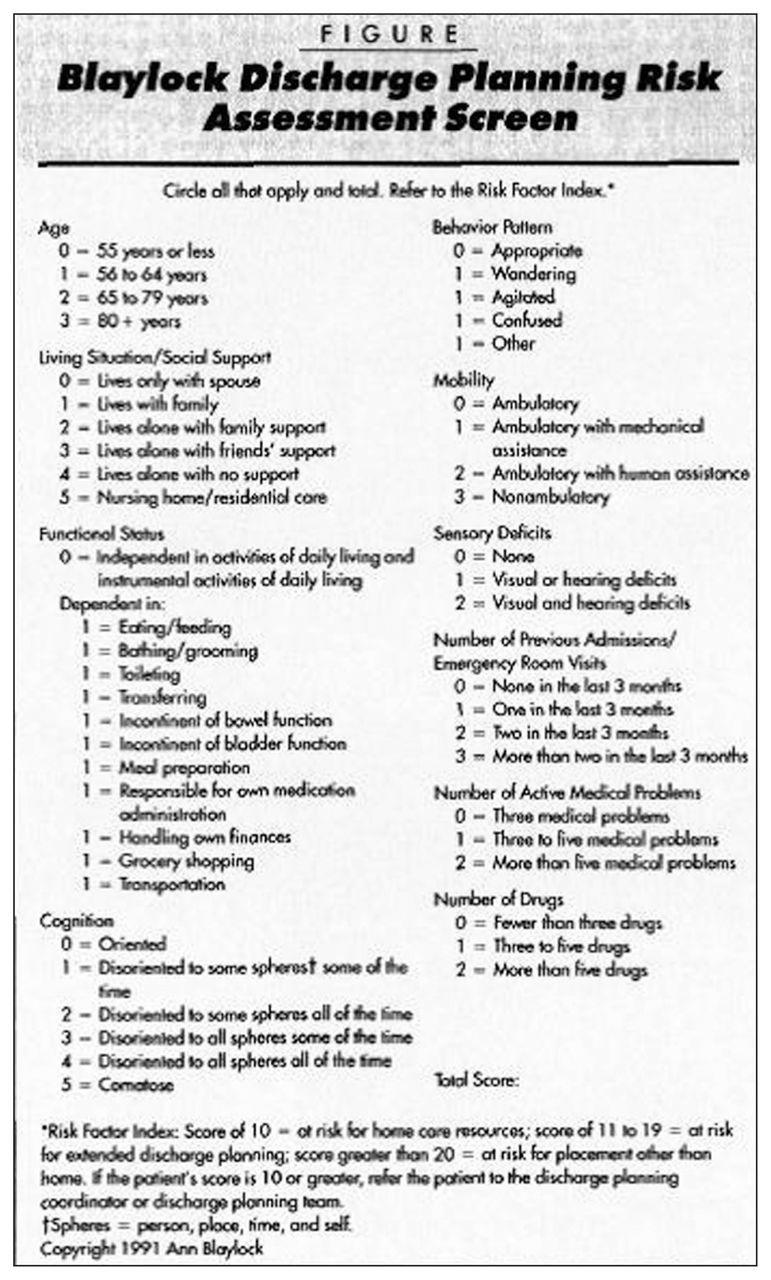
The Blaylock Risk Assessment Screening Score (BRASS) is a presurgical screening tool that can be used to identify patients who may require a more comprehensive discharge plan.4 A copy of the BRASS is shown in Figure 1. In brief, it comprises a 10-item scale that derives a score between 0 and 40, with a higher score correlating with a greater likelihood of discharge complications and LOS. The 10 items that are used to derive the BRASS score are the patient’s age, living situation/social support, functional status, cognition, behavioural pattern, mobility, sensory deficits, number of previous admissions/emergency department visits, number of active medical problems and number of drugs.4
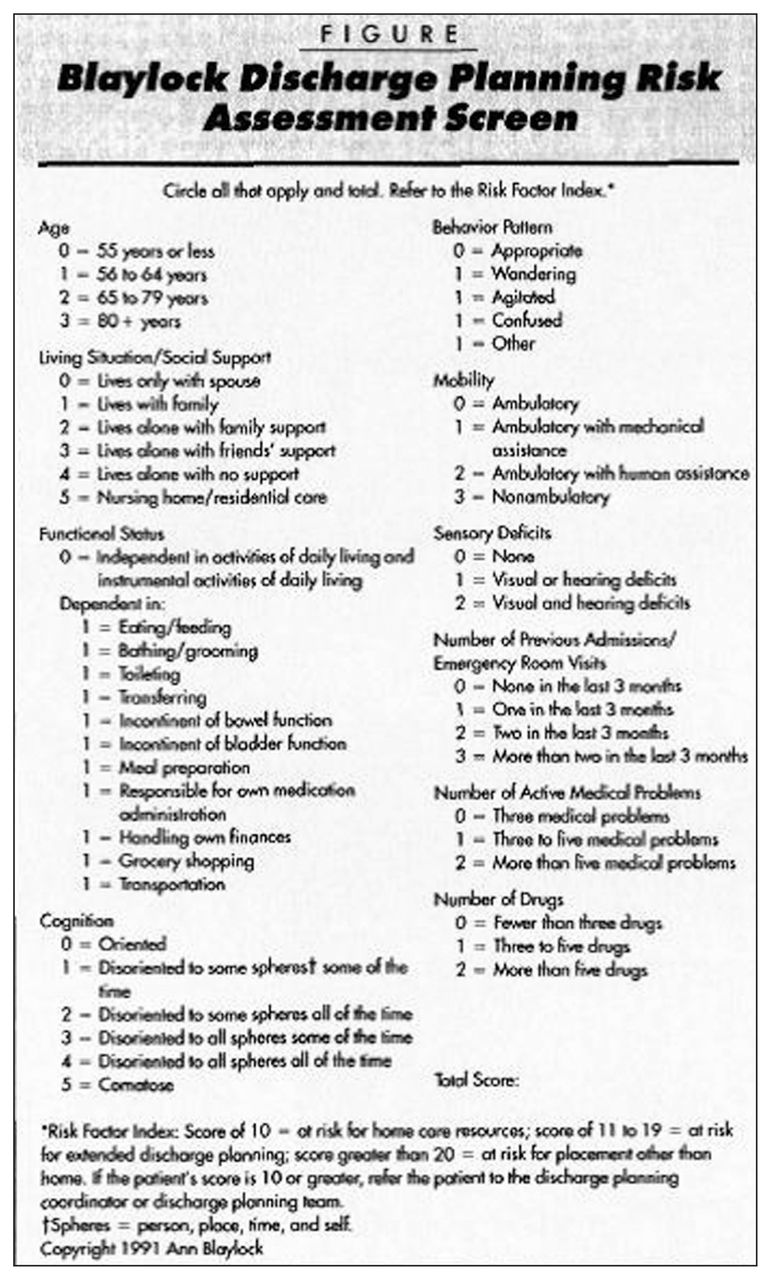
Blaylock Risk Assessment Screening Score (reproduced with permission from Ann Blaylock and the University of Texas Arlington).
Typically, a score of 0–10 identifies patients at low risk for complications, 11–20 identifies those requiring discharge planning, and scores above 20 indicate patients who require extensive discharge planning and who are likely to be discharged to a location other than home.4 The current clinical utility of the BRASS is debated. This screening tool has been used previously with varied success for patients admitted to the intensive care unit (ICU) and in medical patients postdischarge.5,6 However, the patient population for these 2 studies was not specific to knee or hip arthroplasty patients or elective admissions.
The aim of our study was to assess the BRASS in terms of its ability to correctly predict patients at risk of increased hospital stay, specifically, after elective hip or knee arthroplasty at our institution. Other risk factors for delayed discharge (e.g., American Society of Anesthesiologists [ASA] score, body mass index [BMI], type of surgical replacement) were also analyzed and corroborated with this tool in hopes of identifying which patient factors, when used in addition to BRASS scores, could facilitate more accurate identification of patients at risk of longer than expected postoperative LOS.
Methods
Data collection consisted of a retrospective chart review of orthopedic patients treated at Kingston General Hospital (KGH) between August 2007 and June 2010. Individuals undergoing primary elective arthroplasty for knee or hip OA were eligible for inclusion. Exclusion criteria were nonelective hip or knee arthroplasties and revision procedures.
A sample size calculation to determine a statistically significant difference in mean LOS between hip and knee replacement participants with an α of 0.5, power of 0.8, a mean difference of 1 day and standard deviation (SD) of 3 required analysis of 284 cases. We therefore reviewed a sample of 300 cases stemming back from 2010 that would reflect our modern practice for inpatient stay discharge record. Patients who did not consent to have their data used for research purposes and patient charts with absent Blaylock Scores were excluded from analysis.
At KGH, the average LOS for our elective total joint replacement patients is 4.6 (range 1.2–21.2) days.7 This is comparable to the Canadian national average. In the Canadian Joint Replacement Registry 2013 annual report, the median LOS in 2010–2011 for both sexes combined was 5 days for hip replacements and 4 days for knee replacements.8 For the purpose of our study, we defined prolonged LOS as 5 or more days. Other variables that could influence LOS were collected: patient age, ASA score, BMI and type of replacement (knee v. hip).
Statistical analysis
Data were organized and collected with Microsoft Excel and analyzed with SPSS software version 17.0. Statistical significance was established a priori at α = 0.05. We performed multiple linear regression analysis to explore variables predictive of LOS. A multivariate analysis of variance (MANOVA) was performed to identify differences in dependent variables for BRASS quartiles. Post hoc comparisons were Bonferroni corrected. We used contingency tables to calculate sensitivity and specificity as well as positive and negative predictive values according to a BRASS of 8 or more and 10 or more for LOS of 5 days or longer. These results were depicted in a receiver operating characteristic (ROC) curve. Length of stay was analyzed for outliers, and individuals exceeding 2.5 SDs were excluded (n = 2).
Results
A total of 2718 procedures were performed at KGH during our study period. We excluded the charts of 442 patients who underwent nonelective hip or knee arthroplasties and 342 who underwent revision procedures, leaving 1934 charts that met our inclusion criteria. As per our sample size calculation, we reviewed a sample of 300 charts. Of these, 243 case files met our inclusion criteria. A further 2 charts were excluded as outliers, leaving a final sample of 241 patients.
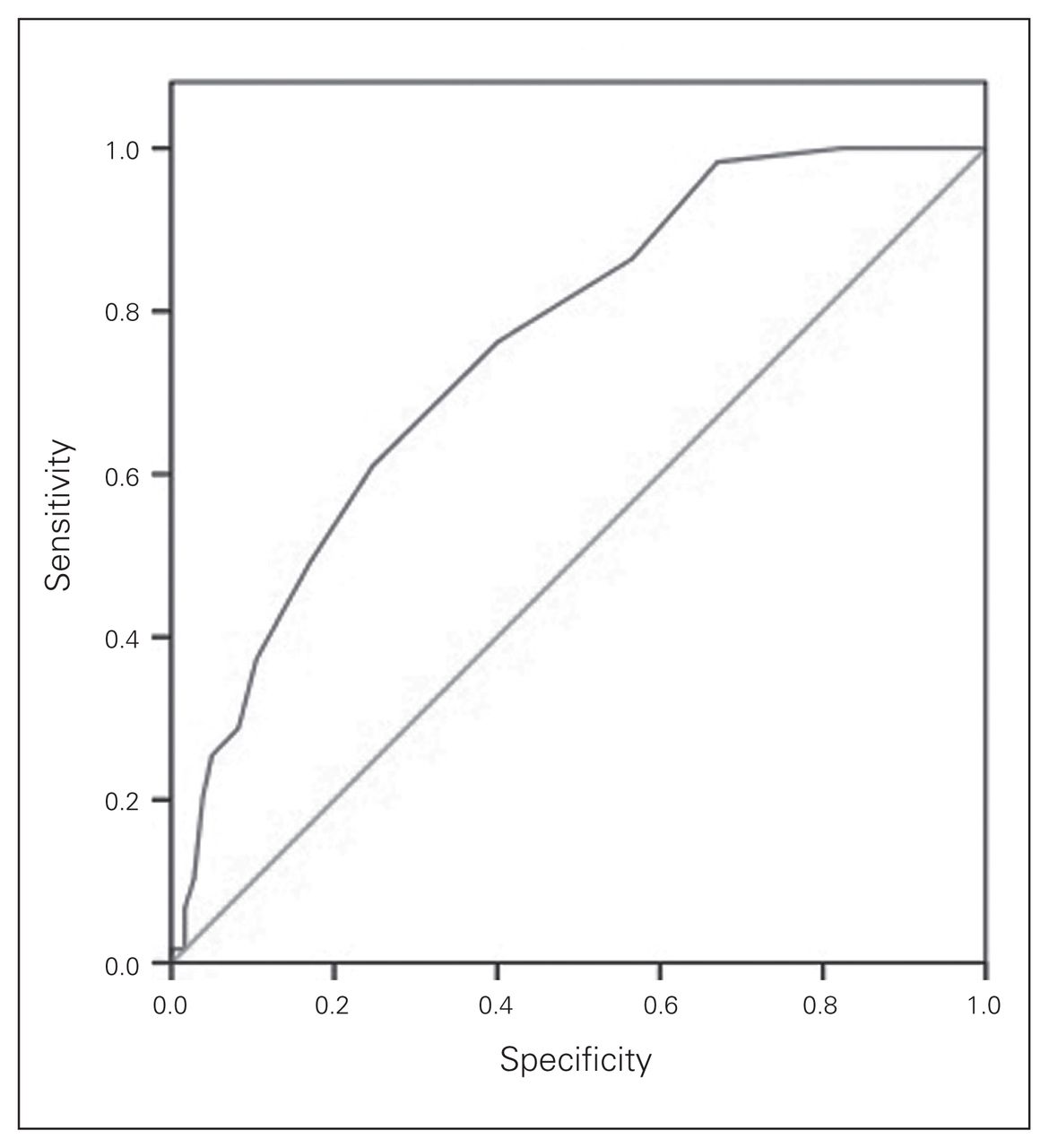
Descriptive statistics are reported in Table 1. Individuals with knee OA accounted for 67% of the cohort, and most patients returned home upon discharge (86%). Age, ASA, LOS and sex were similar between groups, while the average BMI of individuals with knee OA was significantly greater than that of individuals with hip OA (Table 2). Also, patients discharged to hospital had a significantly longer LOS than those discharged home (Table 3). The BRASS for patients discharged home were significantly lower than for those discharged to hospital (Table 3). Multiple linear regression results are summarized in Table 4. Of the variables included in the regression model, higher BRASS and hip replacement were predictive of longer postoperative LOS. The BRASS quartiles (3, 5 and 7.5 representing the 25th, median and 75th percentile, respectively) explored associations with age, sex, type of replacement, ASA score, BMI and LOS (Table 5). We observed a significant main effect of BRASS on age, ASA and LOS. We also found a significant difference in knee and hip OA distribution among the quartiles. Greater BRASS were associated with older age, greater ASA category and longer LOS. Post hoc analysis revealed significant differences in age between all of the quartiles except between the second and third quartiles. Individuals in the first quartile had significantly lower ASA scores than those in the second (p = 0.002), third (p < 0.001) and fourth (p < 0.001) quartiles. The fourth BRASS quartile was associated with significantly longer LOS than all other quartiles (first quartile p < 0.001, second quartile p < 0.001, third quartile p < 0.001). No significant differences in LOS existed among the first 3 quartiles. We used BRASS of 8 or more and 10 or more when assessing the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of the BRASS (Table 6). Sensitivity was low for the cut-offs of both 8 and 10, decreasing for the latter. Specificity, however, was higher, with a value of 83% for a BRASS cut-off of 8 or greater and increasing to 92% with a BRASS cut-off of 10 or greater. An ROC curve is depicted in Figure 2. The area under the curve was 0.76 ± 0.03 (p < 0.001), indicating the accuracy of the measured diagnostic test to be of fair quality.
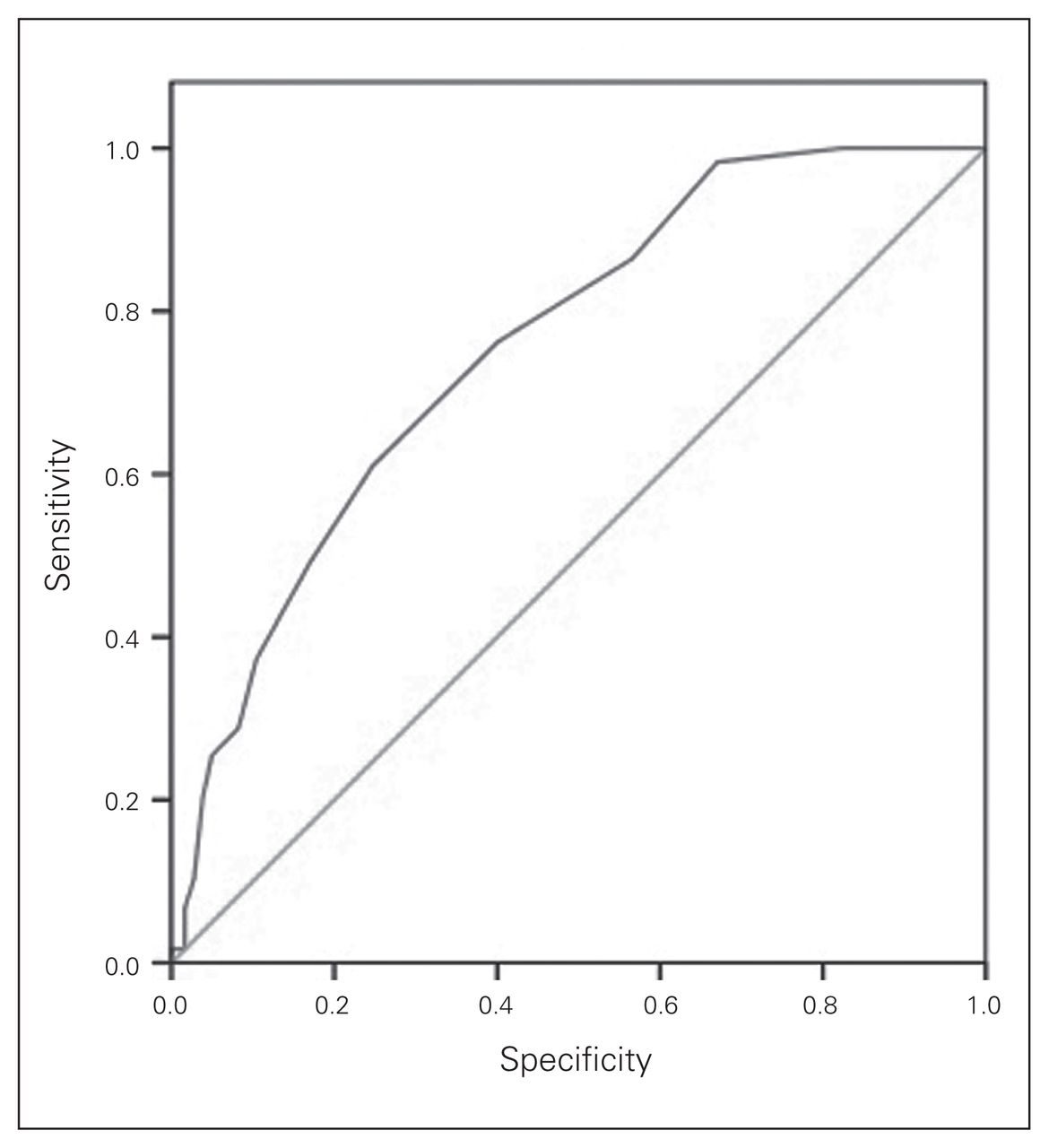
The area under the receiver operating characteristic (ROC) curve was 0.76 ± 0.03 (p < 0.001). This indicates that the accuracy of the measured diagnostic test to be of a fair quality.
Descriptive statistics
Descriptive statistics by surgery type (knee v. hip)
Descriptive statistics by discharge location demographics
Summary of multiple regression analysis for length of stay (n = 239)*
BRASS MANOVA results*
BRASS 2 × 2 table results for a length of stay of ≥ 5 days
Discussion
We performed a retrospective chart review of 241 patients who underwent elective primary hip or knee arthroplasty at KGH, and found the following significant results.
First, higher tabulated BRASS and hip replacement were significant predictors of increased postoperative LOS. Other collected patient demographic factors, such as age, sex, BMI and ASA score did not show a significant correlation with increasing LOS in our multiple regression analysis. Consistent with the results of Mistiaen and colleagues,5 our data show that patients with increased BRASS had longer postoperative LOS. Although not statistically significant (p = 0.10), patients undergoing hip arthroplasty tended to stay longer than those undergoing knee arthroplasty (Table 2). This finding could be explained by our specific patient cohort, as our sample comprised 80 hip arthroplasty patients and 161 knee arthroplasty patients. It is possible, given the smaller number of hip arthroplasty patients, that this may have skewed our results in the smaller hip arthroplasty population pool. It does contradict other publications showing that knee arthroplasty patients tend to stay longer in hospital postsurgery than hip arthroplasty patients.9,10 Pain and function improve less and more slowly in early and intermediate postoperative periods for patients who undergo knee arthroplasty than those who undergo hip arthroplasty.11 In addition, Waddell and colleagues12 found that knee arthroplasty patients are typically older, have a higher BMI and have a poorer health status than hip arthroplasty patients. The knee arthroplasty participants in our study were similar in age to the hip arthroplasty patients, but they did have poorer health status, as measured by the ASA score, and had higher BMIs.
Second, quartile analysis showed that patients with higher BRASS not only had significantly longer postoperative LOS, but were also significantly older and had higher ASA scores. Patients’ BMIs were similar across all 4 quartiles. These findings are supported in the literature. Foote and colleagues13 showed that increased age and ASA scores were associated with prolonged postoperative LOS. Forrest and colleagues,14 when looking for correlation of patient age, sex, marital status, BMI and comorbid illness, found that the only factor that correlated with LOS was age. Moreover, Jonas and colleagues15 reported that the female sex, patients living in more deprived areas, high ASA scores, elevated BMI and age, were all associated with increased LOS following knee arthroplasty. Interestingly, Abbas and colleagues16 also reported that female sex predicted prolonged LOS following total hip replacement. Our quartile analysis also showed a higher percentage of women in the fourth quartile group. Joshi and colleagues17 showed a significant positive correlation between ASA, but not BMI, and LOS for hip and knee arthroplasty patients. Differences among previous studies may be partly explained by different patient cohorts.
Third, analysis of discharge destination showed that both postoperative LOS and BRASS were greater in patients discharged to a nursing home/hospital than in patients discharged home. Theoretically, the unanticipated procurement following arthroplasty surgery of a rehabilitation, retirement or nursing home bed for a patient previously residing at home is a time-consuming process, which increases postoperative LOS. Oldmeadow and colleagues3 showed targeted postoperative care resulted in more patients being discharged directly home after hip or knee arthroplasty, thus decreasing hospital LOS.
Finally, BRASS Scores of 8 or more, and especially 10 or more, had a high specificity when accessing an LOS of 5 days or longer. Both cut-off values were associated with high NPVs. This indicates that there is a high propensity to consider an individual likely to stay in hospital 5 or more days after their surgery if their BRASS is 8 or higher, and even more so if their BRASS is 10 or higher. Sensitivity and PPVs, however, were low. Our low sensitivity is consistent with the results of Mistiaen and colleagues,5 who also found BRASS to poorly identify patients with problems or unmet needs after discharge. They provided possible explanations for this finding that could also be applied to our data. Following surgery, elderly patients may show a decline in their preadmission functional status, and thus, any preoperative screening tools attempting to identify patients at risk of longer than expected postoperative LOS could have missed these patients and not have identified them as high risk based on their preoperative admission status. To better identify patients at risk of longer than expected postoperative LOS following arthroplasty surgery, other patient factors, such as increased age, ASA score and type of surgery, should be included in conjunction with the BRASS to improve the sensitivity or PPV. The high specificity is helpful preoperatively in that scores greater than 10 will most likely lead to increased LOS; anyone scoring higher than 10 will need alternative arrangements, and surgery can be delayed until arrangements are in place. This will maximize bed use efficiency and keep average LOS down. Also, it will allow for the concentrated efforts by allied health care professionals pre-operatively on specific targeted patients to prepare for possible discharge issues and organize rehabilitation in hospital or temporary nursing home care if full home care services are not sufficient.
Longer than expected LOS, as predicted by various BRASS cutoff scores, is consistent with a recent review of our institution’s average LOS for elective hip and knee arthroplasty patients: the average LOS was 4.1 days for patients with a BRASS of 0–10 and 7.3 days for patients with a BRASS of 11–21.3 Furthermore, patients with an LOS longer than 4 days had an average BRASS of 8.3 Like Mistiaen and colleagues,5 we argued that the BRASS index is a promising instrument for discharge planning, but needs further development. As shown by our ROC curve, when used alone as a diagnostic tool BRASS is fairly accurate. However, our results showed that there are other patient-specific factors that also correlate with prolonged LOS that, when used, can increase the sensitivity or PPV of such an assessment.
Our results showed that patient-specific factors, such as age, type of surgery and elevated ASA score, were all correlated with a prolonged postoperative LOS. Thus, when used in conjunction with the BRASS screening tool, they could potentially more effectively and accurately identify patients at risk of prolonged LOS. Results from Husted and colleagues,18 who looked at predictors of LOC in fast-track hip and knee arthroplasty procedures, found that patient variables, such as age, sex, marital status, comorbidity, preoperative use of walking aids, pre- and postoperative hemoglobin levels, need for blood transfusions, ASA scores, and the time between surgery and mobilization, all influenced LOS. However, the greater the number of variables accessed, the harder it is to control and interpret any resulting findings. We advocate the use of the BRASS score, ASA and type of surgery to target the at-risk population and simplify the screening progress without too much effort. Keeping screening simple and effective improves efficiencies all around and is valuable in minimizing complications and LOS in our arthroplasty group.
Conclusion
The BRASS represents a novel and significant predictor of LOS following elective orthopedic surgery. We demonstrated that patients with a BRASS of 8 or more — especially a BRASS of 10 or more — following elective hip and knee arthroplasty surgery, are likely to stay in hospital 5 or more days and should receive pre-emptive social work consultations to facilitate discharge planning. Patient-specific factors, such age, type of surgery and ASA score, are correlated with prolonged postoperative LOS and can be used in combination with the BRASS to more effectively and accurately identify patients at risk of prolonged LOS. This would facilitate necessary arrangements for safe hospital discharge before admission and in turn facilitate timely and efficient posthospital continuity of care. This would allow for more hospital beds and resources to be available for future surgical procedures, reducing cancellations for lack of surgical beds and reducing costs per case for hospital budgets.
Footnotes
Competing interests: G. Wood declares being a paid consultant and receiving speaker fees from Stryker. No other competing interests declared.
Contributors: D. Cunic and G. Wood designed the study. D. Cunic, S. Lacombe and K. Kohajer acquired and analyzed the data, which H. Grant also analyzed. All authors wrote and reviewed the article and approved the final version for publication.
- Accepted April 29, 2014.

{kind=link}
{kind=link}
Article tools





