
Summary
Synopsis
Selegiline (deprenyl) is a selective inhibitor of cerebral monoamine oxidase type B at the dosage (10 mg/day) used in patients with Parkinson’s disease. Through this activity, the drug increases nigrostriatal dopamine levels, and may protect neurons against damage by free radicals and possibly exogenous neurotoxins. Selegiline also inhibits dopamine reuptake from the synaptic cleft. Because of its selectivity, selegiline 10mg daily does not prevent the breakdown and exacerbate the indirect pressor effects of dietary amines such as tyramine; it is devoid of the ‘cheese’ effect.
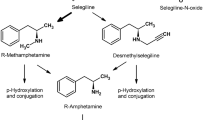
Following oral administration, selegiline is rapidly metabolised to L-methamphetamine and L-amphetamine, which may account for the euphoria and insomnia seen in many patients, although potentiation of dopaminergic activity with concurrent levodopa appears more likely. The drug is a useful adjunct to levodopa in Parkinsonism, improving ‘end-of dose’ fluctuations, producing modest improvements in motor function, and allowing a reduction in levodopa dosage. Indeed, if levodopa dosages are not decreased when selegiline is added to the therapeutic regimen, peak concentration dyskinesias due to levodopa are often exacerbated. However, symptomatic benefits are rarely maintained for more than a year and selegiline is relatively ineffective in allaying the abrupt swings in response to levodopa (‘on/off’ effects). When used alone in patients with mild disease, selegiline appears to slow the rate of symptom progression and may extend survival, through either neuroprotection or symptom relief Whichever mechanism(s) is responsible, there is strong evidence to suggest that selegiline should be considered both in patients newly diagnosed with Parkinson’s disease in an attempt to delay symptom progression, and in those experiencing dose-dependent fluctuations in response to levodopa.
Pharmacological and Pharmacokinetic Properties
At the dosage recommended for use in patients with Parkinson’s disease (10 mg/day), selegiline is an irreversible selective inhibitor of monoamine oxidase type B (MAO-B), an enzyme responsible for dopamine metabolism in the brain. Post mortem studies in recipients of selegiline and levodopa indicate about 90% inhibition of nigrostriatal MAO-B activity resulting in a 70% increase in dopamine levels compared with untreated patients with Parkinson’s disease.
Deamination of dopamine by MAO-B produces oxygen free radicals, which may be implicated in the progressive nigrostriatal degeneration in idiopathic Parkinson’s disease. Selegiline should therefore limit this oxidative stress by blocking MAO-B, and indeed this hypothesis has been supported by animal studies. MAO-B also catalyses the formation of the neurotoxic 1-methyl-4-phenylpyridinium ion (MPP+) from l-methyl-4-phenyl-l,2,3,6-tetrahydropyridine (MPTP), a compound which causes symptoms and pathology very similar to those of idiopathic Parkinsonism. Pretreatment with selegiline prevented the signs and symptoms of MPTP-induced neuronal damage in animals.
Dopaminergic function is also enhanced by the ability of selegiline to block synaptic dopamine reuptake.
Because selegiline is extensively and rapidly metabolised, mainly to L-methamphetamine, L-amphetamine and demethyl-selegiline, pharmacokinetic analysis to date is limited. The parent drug is undetectable following oral administration, but peak serum concentrations of the metabolites occurred within 0.5 to 2 hours with an absorption half-life of 24 minutes. Mean serum concentrations of L-methamphetamine, L-amphetamine and demethyl-selegiline were 9, 1.3 and 5.8 µg/L, respectively, after selegiline 10 mg/day orally for 22 to 24 months in 4 patients with Parkinson’s disease. Selegiline is extensively distributed, despite being 94% bound to plasma proteins, and binds to striatum, cortex and brain stem. Renal elimination is the predominant route of selegiline excretion, with 86% of an oral dose recovered in the urine, principally as L-methamphetamine (59%) and L-amphetamine (26%).
Therapeutic Use
Selegiline 10mg daily has been investigated as a supplement to standard levodopa plus decarboxylase inhibitor regimens in an attempt to smooth out response fluctuations, and as monotherapy in patients with early mild disease to try to slow symptom progression of Parkinson’s disease.
The many noncomparative and placebo-controlled studies demonstrated that the addition of selegiline to levodopa improved the disability rating scores by 18 to 32%, compared with 8 to 27% in placebo recipients. Tremor was more frequently relieved than rigidity. The dosage of levodopa was reduced by approximately 10 to 30% without adversely affecting the degree of symptom control. ‘End-of-dose’ fluctuations in response to levodopa significantly improved in 50 to 63% of selegiline recipients, and early morning akinesias in 56%, but the drug had no significant effect in improving ‘on/off’ oscillations. Moreover, the benefits of adding selegiline declined with time, with a reduction in both the proportion of adequately controlled patients and the extent of improvement; the mean duration of benefit was 7 to 8 months in 1 long term study. A retrospective study suggested that addition of selegiline to a levodopa regimen extended life expectancy by 15 months.
Encouraging results have been obtained with selegiline monotherapy in patients with early and mildly symptomatic Parkinson’s disease. Prospective trials revealed that selegiline monotherapy delayed, but did not prevent, the progression of symptoms and prolonged mobility without additional levodopa by 6 to 11 months. After 12 months, 26 to 44% of selegiline recipients compared with 47 to 56% of placebo-treated patients had symptoms sufficiently severe to justify starting levodopa therapy. It is unclear if these results are a consequence of protection against further neuronal destruction or are symptomatic effects. The latter seems less likely since selegiline alone provides little symptom relief.
Tolerability
Selegiline does not significantly inhibit MAO type A at therapeutic doses used to treat Parkinson’s disease. It is therefore not associated with the ‘cheese’ effect, which occurs when the indirect pressor effects of dietary amines (e.g. tyramine) are exacerbated because of accumulation resulting from nonselective MAO inhibition. Headache has, however, been reported by 4 to 26% of patients and a single hypertensive episode has been documented. Orthostatic hypotension, occasionally causing syncope, has occurred in several patients.
Because it potentiates striatal dopaminergic activity, selegiline exacerbates peak concentration dyskinesias due to levodopa in approximately 28% of patients. Symptoms usually resolve when the levodopa dosage is reduced.
Mood elevation (in 6 of 11 patients), insomnia (in 10 to 32%; similar to levodopa alone), hallucinations (in 2 to 9%) and confusion (in 5 to 10%) have occurred during coadministration of selegiline and levodopa, indicating caution when introducing selegiline in some elderly demented patients. The most likely cause of these effects appears to be increased dopaminergic activity, but there is possibly some contribution from the selegiline metabolites L-methamphetamine and L-amphetamine since insomnia and euphoria have been noted during selegiline monotherapy. Gastrointestinal symptoms, primarily nausea, occur in 12% of selegiline recipients, and pre-existing peptic ulcer may be exacerbated.
Drug Interactions
The concurrent use of selegiline with pethidine (meperidine) is contraindicated, and fluoxetine should be avoided. Coadministration of medications containing sympathomimetic amines (e.g. cold remedies) appears to be safe if the daily dosage of selegiline does not exceed 10mg.
Dosage and Administration
In the treatment of patients with Parkinson’s disease, selegiline 5mg orally twice daily, with breakfast and at midday, is recommended. Higher dosages are no more effective than 10 mg/day, and restriction of both tyramine-containing food and indirect sympathomimetic medications may be necessary above this dosage.
Similar content being viewed by others


References
Ballard PA, Tetrud JW, Langston JW. Permanent human parkinsonism due to l-methyl-4-phenyl-l,2,3,6-tetrahydropyridine (MPTP): seven cases. Neurology 35: 949–456, 1985
Beckett AH, Rowland M. Urinary excretion kinetics of amphetamine in man. Journal of Pharmacy and Pharmacology 17: 628–639, 1965a
Beckett AH, Rowland M. Urinary excretion kinetics of methylamphetamine in man. Journal of Pharmacy and Pharmacology 17: 1095–1145, 1965b
Birkmayer W, Knoll J, Riederer P, Youdim MBH, Hars V, et al. Increased life expectancy resulting from addition of L-Deprenyl to Madopar treatment in Parkinson’s disease: a long-term study. Journal of Neural Transmission 64: 113–127, 1985
Birkmayer W, Riederer P, Ambrozi L. Implications of combined treatment with’ Madopar’ and L-Deprenil in Parkinson’s disease: a long term study. Lancet 1: 439–443, 1977
Birkmayer W, Riederer P, Youdim MBH, Linauer W. The potentiation of the anti akinetic effect after L-dopa treatment by an inhibitor of Mao-B, Deprenil. Journal of Neural Transmission 36: 303–326, 1975
Bradbury AJ, Costall B, Jenner PG, Kelly ME, Marsden CD, et al. The neurotoxic actions of l-methyl-4-phenylpyridine (MPP+) are not prevented by Deprenyl treatment. Neuroscience Letters 58: 177–181, 1985
Brodersen P, Philbert A, Gulliksen G, Stigård A. The effect of L-Deprenyl on on-off phenomena in Parkinson’s disease. Acta Neurologica Scandinavica 71: 494–497, 1985
Burns RS, Chiueh CC, Markey SP, Ebert MH, Jacobowitz DM, et al. A primate model of parkinsonism: selective destruction of dopaminergic neurons in the pars compacta of the substantia nigra by N-methyl-4-phenyl-l,2,3,6-tetrahydropyridine. Proceedings of the National Academy of the Sciences of the United States of America 80: 4546–4550, 1983
Carrillo M-C, Kanai S, Nokubo M. (-) Deprenyl induces activities of both Superoxide dismutase and catalase but not of glutathione peroxidase in the striatum of young male rats. Life Sciences 48: 517–521, 1991
Cedarbaum JM, Silvestri M, Clark M, Harts A, Kutt H. L-Deprenyl, levodopa pharmacokinetics, and response fluctuations in Parkinson’s disease. Clinical Neuropharmacology 13: 29–35, 1990
Chiba K, Trevor A, Castagnoli Jr JN. Metabolism of the neurotoxic tertiary amine, MPTP, by brain monoamine oxidase. Biochemical and Biophysical Research Communications 120: 574–578, 1984
Cohen G, Pasik P, Cohen B, Leist A, Mytilineou C, et al. Pargyline and Deprenyl prevent the neurotoxicity of l-methyl-4-phenyl-l,2,3,6-tetrahydropyridine (MPTP) in monkeys. European Journal of Pharmacology 106: 209–210, 1984
Cohen G, Spina MB. Deprenyl suppresses the oxidant stress associated with increased dopamine turnover. Annals of Neurology 26: 689–690, 1989
Csanda E, Tarczy M. Selegiline in the early and late phases of Parkinson’s disease. Journal of Neural Transmission 25 (Suppl.): 105–113, 1987
Csanda E, Tarczy M, Takáts A, Mogyorós I, Köves A, et al. L-Deprenyl in the treatment of Parkinson’s disease. Journal of Neural Transmission 19 (Suppl.): 283–290, 1983
Davis GC, Williams AC, Markey SP, Ebert MH, Caine ED, et al. Chronic Parkinsonism secondary to intravenous injection of meperidine analogues. Psychiatry Research 1, 249–254, 1979
Donnelly CH, Murphy DL. Substrate- and inhibitor-related characteristics of human platelet monoamine oxidase. Biochemical Pharmacology 26, 853–858, 1977
Eisler T, Teräväinen H, Nelson R, Krebs H, Weise V, et al. Deprenyl in Parkinson disease. Neurology 31: 19–23, 1981
Elizan TS, Moros DA, Yahr MD. Early combination of selegiline and low-dose levodopa as initial symptomatic therapy in Parkinson’s disease. Archives of Neurology 48: 31–34, 1991
Elizan TS, Yahr MD, Moros DA, Mendoza MR, Pang S, et al. Selegiline as an adjunct to conventional levodopa therapy in Parkinson’s disease: experience with this type B monoamine oxidase inhibitor in 200 patients. Archives of Neurology 46: 1280–1283, 1989a
Elizan TS, Yahr MD, Moros DA, Mendoza MR, Pang S, et al. Selegiline use to prevent progression of Parkinson’s disease. Archives of Neurology 46: 1275–1279, 1989b
Elsworth JD, Glover V, Reynolds GP, Sandier M, Lees AJ, et al. Deprenyl administration in man: a selective monoamine oxidase B inhibitor without the ‘cheese effect’. Psychopharmacology 57: 33–38, 1978
Elsworth JD, Sandier M, Lees AJ, Ward C, Stern GM. The contribution of amphetamine metabolites of (−)-deprenyl to its antiparkinsonian properties. Journal of Neural Transmission 54: 105–110, 1982
Fahn S. High-dosage antioxidants in early Parkinson’s disease. Abstract Archives of Neurology 45: 810, 1988
Feighner JP, Boyer WF, Tyler DL, Neborsky RJ. Adverse consequences of fluoxetine-MAOI combination therapy. Journal of Clinical Psychiatry 51: 222–225, 1990
Fowler CJ, Oreland L, Marcusson J, Windblad B. Titration of human brain monoamine oxidase-A and -B by clorgyline and L-Deprenil. Naunyn-Schmiedeberg’s Archives of Pharmacology 311: 263–272, 1980
Fowler JS, MacGregor RR, Wolf AP, Arnett CD, Dewey SL, et al. Mapping human brain monoamine oxidase A and B with 11C-labeled suicide inactivators and PET. Science 235: 481–485, 1987
Friedhoff AJ. Deprenyl and the progression of Parkinson’s disease. Correspondence. Science 249: 303, 1990
Fuller RW, Hemrick-Luecke SK. A high dose of MPTP overcomes the protective effect of selegiline against dopaminergic neurotoxicity. Journal of Pharmacy and Pharmacology 41: 492–493, 1989
Fuller RW, Hemrick-Luecke SK, Perry KW. Deprenyl antagonizes acute lethality of l-methyl-4-phenyl-l,2,3,6-tetrahydropyridine in mice. Journal of Pharmacology and Experimental Therapeutics 247: 531–535, 1988
Giovannini P, Grassi MP, Scigliano G, Piccolo I, Soliveri P, et al. Deprenyl in Parkinson disease: personal experience. Italian Journal of Neurological Sciences 6: 207–212, 1985
Giovannini P, Martignoni E, Piccolo I, Pacchetti C, Grassi MP, et al. (-)Deprenyl in Parkinson’s disease: a two-year study in the different evolutive stages. Journal of Neural Transmission 22 (Suppl.): 235–246, 1986
Glover V, Elsworth JD, Sandler M. Dopamine oxidation and its inhibition by (−)-Deprenyl in man. Journal of Neural Transmission 16 (Suppl.): 163–172, 1980
Glover V, Sandier M, Owen F, Riley GJ. Dopamine is a monoamine oxidase B substrate in man. Nature 265: 80–81, 1977
Golbe LI. Long-term efficacy and safety of deprenyl (selegiline) in advanced Parkinson’s disease. Neurology 39: 1109–1111, 1989
Golbe LI, Langston JW, Shoulson I. Selegiline and Parkinson’s disease: protective and symptomatic considerations. Drugs 39: 646–651, 1990
Golbe LI, Lieberman AN, Muenter MD, Ahlskog JE, Gopinathan G, et al. Deprenyl in the treatment of symptom fluctuations in advanced Parkinson’s disease. Clinical Neuropharmacology 11: 45–55, 1988a
Golbe LI, Farrell TM, Davis PH. Case-control study of early life dietary factors in Parkinson’s disease. Archives of Neurology 45: 1350–1353, 1988b
Goldstein M, Lew JY, Deutch AY. Deprenyl for the treatment of early Parkinson’s disease. New England Journal of Medicine 322(21): 1526–1527, 1990
Halliwell B. Oxidants and the central nervous system: some fundamental questions. Acta Neurologica Scandinavica 80 (Suppl. 126): 23–33, 1989
Heikkila RE, Manzino L, Cabbat FS, Duvoisin RC. Protection against the dopaminergic neurotoxicity of l-methyl-4-phenyl-1,2,5,6-tetrahydropyridine by monoamine oxidase inhibitors. Nature 311, 467–469, 1984
Heinonen EH, Rinne UK, Tuominen J. Selegiline in the treatment of daily fluctuations in disability of parkinsonian patients with long-term levodopa treatment. Acta Neurologica Scandinavica 80 (Suppl. 126): 113–118, 1989a
Heinonen EH, Myllylä V, Sotaniemi K, Lammintausta R, Salonen JS, et al. Pharmacokinetics and metabolism of selegiline. Acta Neurologica Scandinavica 80 (Suppl. 126): 93–99, 1989b
Javitch JA, Snyder SH, Uptake of MPP(+) by dopamine neurons explains selectivity of parkinsonism-inducing neurotoxin, MPTP. European Journal of Pharmacology 106: 455–456, 1984
Jenner P, Rupniak NM, Rose S, Kelly E, Kilpatrick G, et al. l-Methyl-4-phenyl-1,2,3,6-tetrahydropyridine-induced parkinsonism in the common marmoset. Neuroscience Letters 50: 85–90, 1984
Kalir A, Sabbagh A, Youdim MBH. Selective acetylenic ‘suicide’ and reversible inhibitors of monoamine oxidase types A and B. British Journal of Pharmacology 73: 55–64, 1981
Karoum F, Chuang LW, Eisler T, Calne DB, Liebowitz MR, et al. Metabolism of (−)deprenyl to amphetamine and metamphetamine may be responsible for deprenyl’s therapeutic benefit: a biochemical assessment. Neurology 32: 503–509, 1982
Kish SJ, Morito C, Hornykiewicz O. Glutathione peroxidase activity in Parkinson’s disease brain. Neuroscience Letters 58: 343–346, 1985
Knoll J. The pharmacology of (−)deprenyl. Journal of Neural Transmission 22 (Suppl.): 75–89, 1986
Knoll J. R-(−)-deprenyl (selegiline, Movergan®) facilitates the activity of the nigrostriatal dopaminergic neuron. Journal of Neural Transmission 25(4): 45–66, 1987
Knoll J. Extension of life span of rats by long-term (-)deprenyl treatment. Mount Sinai Journal of Medicine 55: 67–74, 1988
Knoll J. The pharmacology of selegiline ((−)deprenyl). New aspects. Acta Neurologica Scandinavica 80 (Suppl. 126): 83–91, 1989
Knoll J, Ecsery Z, Kelemen K, Nievel J, Knoll B. Phenylisopro-pylmethylpropinylamine (E-250), a new psychic energizer. Archives of Internal Pharmacodynamics 155: 154–164, 1965
Langston JW. Selegiline as neuroprotective therapy in Parkinson’s disease: concepts and controversies. Neurology 40 (Suppl. 3): 61–66, 1990
Langston JW, Ballard P, Tetrud JW, Irwin I. Chronic Parkinsonism in humans due to a product of meperidine-analog synthesis. Science 219: 979–980, 1983
Langston JW, Langston EB, Irwin I. MPTP-induced parkinsonism in human and non-human primates — clinical and experimental aspects. Acta Neurologica Scandinavica 100 (Suppl.): 49–54, 1984
Langtry HD, Clissold SP. Pergolide: a review of its pharmacological properties and therapeutic potential in Parkinson’s disease. Drugs 39: 491–506, 1990
Lee DH, Mendoza M, Dvorozniak MT, Chung E, van Woert MH, et al. Platelet monoamine oxidase in Parkinson patients: effect of L-deprenyl therapy. Journal of Neural Transmission 1: 189–194, 1989
Lees AJ. The on-off phenomenon. Journal of Neurology, Neurosurgery and Psychiatry 52 (Suppl.): 29–37, 1989
Lees AJ, Shaw KM, Kohout LJ, Stern GM, Elsworth JD. Deprenyl in Parkinson’s disease. Lancet 2: 791–795, 1977
Lewin R. Parkinson’s disease: an environmental cause? Science 229: 257–258, 1985a
Lewin R. Clinical trial for Parkinson’s disease. Science 230: 527–528, 1985b
Lieberman AN, Gopinathan G, Neophytides A, Foo SH. Deprenyl versus placebo in Parkinson disease: a double-blind study. New York State Journal of Medicine 87: 646–649, 1987
Magyar K, Tothfalusi L. Pharmacokinetic aspects of deprenyl effects. Polish Journal of Pharmacology and Pharmacy 36: 373–384, 1984
Marley E, Blackwell B. Interactions of monoamine oxidase inhibitors, amines and foodstuffs. Advances in Pharmacology and Chemotherapy 8: 186–239, 1970
Marsden CD. Parkinson’s disease. Lancet 335: 948–952, 1990
Marttila RJ, Lorentz H, Rinne UK. Oxygen toxicity protecting enzymes in Parkinson’s disease. Increase of Superoxide dismutase-like activity in the substantia nigra and basal nucleus. Journal of the Neurological Sciences 86: 321–331, 1988
Meeker JE, Reynolds PC. Postmortem tissue methamphetamine concentrations following selegiline administration. Journal of Analytical Toxicology 14: 330–331, 1990
Myllylä VV, Sotaniemi KA, Tuominen J, Heinonen EH. Selegiline as primary treatment in early phase Parkinson’s disease — an interim report. Acta Neurologica Scandinavica 80 (Suppl.): 177–182, 1989
Myllylä VV, Sotaniemi KA, Vuorinen J, Heinonen EH. Selegiline (deprenyl) as primary treatment in Parkinsons disease. In Rinne UK & Heinonen E (Eds) Selegiline therapy in early Parkinson’s disease, pp. 19–24, European Conference on Parkinson’s Disease and Extrapyrimidal Disorders, Rome, July 10–14, 1990, Munksgaard, Copenhagen, 1990
Nutt JG. Abnormalities of posture and movement. In Cassel et al. (Eds) Geriatric Medicine, 2nd ed., pp. 463–472, Springer-Verlag, New York, 1990
Parkes JD, Tarsy D, Marsden CD, Bovill KT, Phipps JA, et al. Amphetamines in the treatment of Parkinson’s disease. Journal of Neurology, Neurosurgery, and Psychiatry 38: 232–237, 1975
Parkinson Study Group. Effect of deprenyl on the progression of disability in early Parkinson’s disease. New England Journal of Medicine 321: 1364–1371, 1989a
Parkinson Study Group. DATATOP: a multicenter controlled clinical trial in early Parkinson’s disease. Archives of Neurology 46: 1052–1060, 1989b
Pearce JMS. Progression of Parkinson’s disease. British Medical Journal 301: 396, 1990
Perry TL, Godin DV, Hansen S. Parkinson’s disease: a disorder due to nigral glutathione deficiency? Neuroscience Letters 33: 305–310, 1982
Perry TL, Yong VW. Idiopathic Parkinson’s disease, progressive supranuclear palsy and glutathione metabolism in the substantia nigra of patients. Neuroscience Letters 67: 269–274, 1986
Pickar D, Cohen RM, Jimerson DC, Murphy DL. Tyramine infusions and selective monoamine oxidase inhibitor treatment. Psychopharmacology 74: 4–7, 1981
Poewe W, Gerstenbrand F, Ransmayr G. Experience with selegiline in the treatment of Parkinson’s disease. Journal of Neural Transmission 25 (Suppl.): 131–135, 1987
Prasad A, Glover V, Goodwin BL, Sandier M, Signy M, et al. Enhanced pressor sensitivity to oral tyramine challenge following high dose selegiline treatment. Psychopharmacology 95: 540–543, 1988
Presthus J, Berstad J, Lien K. Selegiline (l-deprenyl) and low-dose levodopa treatment of Parkinson’s disease: a double-blind crossover trial. Acta Neurologica Scandinavica 76: 200–203, 1987
Presthus J, Hajba A. Deprenyl (selegiline) combined with levodopa and a decarboxylase inhibitor in the treatment of Parkinson’s disease. Acta Neurologica Scandinavica 95 (Suppl.): 127–133, 1983
Przuntek H, Kuhn W. The effect of R-(-)-deprenyl in de novo Parkinson patients on combination therapy with levodopa and decarboxylase inhibitor. Journal of Neural Transmission 25 (Suppl.): 97–104, 1987
Quinn NP. Anti-Parkinsonian drugs today. Drugs 28: 236–262, 1984
Rascol O, Montastruc JL, Senard JM, Demonet JF, Simonetta M, et al. Two weeks of treatment with deprenyl (selegiline) does not prolong L-dopa effect in parkinsonian patients: a double-blind cross-over placebo-controlled trial. Neurology 38: 1387–1391, 1988
Reynolds GP, Elsworth JD, Blau K, Sandier M, Lees AJ, et al. Deprenyl is metabolised to methamphetamine and amphetamine in man. British Journal of Clinical Pharmacology 6: 542–544, 1978a
Reynolds GP, Riederer P, Sandier M, Jellinger K, Seemann D. Amphetamine and 2-phenylethylamine in post-mortem parkinsonian brain after (-)deprenyl administration. Journal of Neural Transmission 43: 271–277, 1978b
Riederer P, Sofic E, Rausch WD, Schmidt B, Reynolds GP, et al. Transition metals, ferritin, glutathione, and ascorbic acid in parkinsonian brains. Journal of Neurochemistry 52: 515–520, 1989
Riederer P, Youdim MBH. Monoamine oxidase activity and monamine metabolism in brains of parkinsonian patients treated with 1-deprenyl. Journal of Neurochemistry 46: 1359–1365, 1986
Riederer P, Youdim MBU, Rausch WD, Birkmayer W, Jellinger K, et al. On the mode of action of L-Deprenyl in the human central nervous system. Journal of Neural Transmission 43: 217–226, 1978
Rinne JO, Roytta M, Rummukainen J, Paljarvi L, Rinne UK. Nigral degeneration in Parkinson’s disease. In Rinne UK & Heinonen E (Eds) Selegiline therapy in early Parkinson’s disease, pp. 9–12, European Conference on Parkinson’s Disease and Extrapyramidal Disorders, Rome, July 10–14, 1990. Munksgaard, Copenhagen, 1990.
Rinne UK. Deprenyl (selegiline) in the treatment of Parkinson’s disease. Acta Neurologica Scandinavica 95 (Suppl.): 107–111, 1983
Rossetti ZL, Sotgin A, Sharp DE, Hadjiconstantinou M, Neff NH. 1-Methyl-4-phenyl-l,2,3,6-tetrahydropyridine (MPTP) and free radicals in vitro. Biochemical Pharmacology 37: 4573–4574, 1988
Ruggieri S, Denaro A, Meco G, Carta A, Stocchi F, et al. Multicenter trial of L-Deprenyl in Parkinson disease. Italian Journal of Neurological Sciences 7: 133–137, 1986
Saggu H, Cooksey J, Dexter D, Wells FR, Lees A, et al. A selective increase in paniculate Superoxide dismutase activity in parkinsonian substantia nigra. Journal of Neurochemistry 53: 692–697, 1989
Saint-Hilaire M, Feldman RG, Durso R. Deprenyl for the treatment of early Parkinson’s disease. Correspondence. New England Journal of Medicine 322: 1527, 1990
Sandier M. (-)Deprenyl in perspective: prophylaxis for Parkinson’s disease? Journal of Neural Transmission 22 (Suppl.): 107–115, 1986
Schachter M, Marsden CD, Parkes JD, Jenner P, Testa B. Deprenyl in the management of response fluctuations in patients with Parkinson’s disease on levodopa. Journal of Neurology, Neurosurgery, and Psychiatry 43: 1016–1021, 1980
Schulz R, Antonin K-H, Hoffmann E, Jedrychowski M, Nilsson E, et al. Tyramine kinetics and pressor sensitivity during monoamine oxidase inhibition by selegiline. Clinical Pharmacology and Therapeutics 46: 528–536, 1989
Shoulson I, Fahn S, Oakes D, Lang A, Langston JW, et al. Deprenyl for the treatment of early Parkinson’s disease. New England Journal of Medicine 322: 1527–1528, 1990
Sivertsen B, Dupont E, Mikkelsen B, Mogensen P, Rasmussen C, et al. Selegiline and levodopa in early or moderately advanced Parkinson’s disease: a double-blind controlled short- and long-term study. Acta Neurologica Scandinavica 126: 147–152, 1989
Sonsalla PK, Golbe LI. Deprenyl as prophylaxis against Parkinson’s disease? Clinical Neuropharmacology 11: 500–511, 1988
Sterling TD. Deprenyl for the treatment of early Parkinson’s disease. Correspondence. New England Journal of Medicine 322: 1526, 1990
Sternbach H. Danger of MAOI therapy after fluoxetine withdrawal. Lancet 2: 850–851, 1988
Suchowersky O, deVries JD. Interaction of fluoxetine and selegiline. Correspondence. Canadian Journal of Psychiatry 35: 571–572, 1990
Sudarsky L. Deprenyl and the progression of Parkinson’s disease. Correspondence. Science 249: 303, 1990
Sunderland T, Mueller EA, Cohen RM, Jimerson DC, Pickar D, et al. Tyramine pressor sensitivity changes during deprenyl treatment. Psychopharmacology 86: 432–437, 1985
Teräväinen H. Selegiline in Parkinson’s disease. Acta Neurologica Scandanavica 81: 333–336, 1990
Tetrud JW, Langston JW. R-(-)-Deprenyl as a possible protective agent in Parkinson’s disease. Journal of Neural Transmission 25 (Suppl.): 69–79, 1987
Tetrud JW, Langston JW. The effect of deprenyl (selegiline) on the natural history of Parkinson’s disease. Science 245: 519–522, 1989
Tetrud JW, Langston JW. Deprenyl and the progression of Parkinson’s disease. Science 249: 303–304, 1990
Teychenne PF, Parker S. Double-blind;, crossover placebo controlled trial of selegiline in Parkinson’s disease — an interim analysis. Acta Neurologica Scandinavica 126: 119–125, 1989
Waters CH. Side effects of selegiline (eldepryl). Abstract 938P. Neurology 40 (Suppl.): 370, 1990
Wiener HL, Hashim A, Lajtha A, Sershen H. Chronic L-Deprenyl does not alter the restoration of striatal dopamine in MPTP-lesioned mice. Journal of Neuroscience Research 23: 326–329, 1989
Yahr MD, Elizan TS, Moros D. Selegiline in the treatment of Parkinson’s disease — long term experience. Acta Neurologica Scandinavica 126: 157–161, 1989
Yoshida T, Yamada Y, Yamamoto T, Kuroiwa Y. Metabolism of deprenyl, a selective monoamine oxidase (MAO)B inhibitor in rat: relationship of metabolism to MAO-B inhibitory potency. Xenobiotica 16: 129–136, 1986
Youdim MBH. The active centers of monoamine oxidase types ‘A’ and ‘B’: binding with (14C)-chorgyline and (14C)-deprenyl. Journal of Neural Transmission 43: 199–208, 1978
Zornberg GL. Severe adverse interaction between pethidine and selegiline. Correspondence. Lancet 337(1): 246, 1991
Zweig RM, Carmichael JM, Morrill GB. Deprenyl for the treatment of early Parkinson’s disease. Correspondence. New England Journal of Medicine 322: 1526, 1990
Author information
Authors and Affiliations
Additional information
Various sections of the manuscript reviewed by: S.T. Gancher, Department of Neurology, Oregon Health Sciences University School of Medicine, Portland, Oregon, USA; P. Giovannini, Department of Neurology, Istituto Nazionale Neurologico ‘C.Besta’, Milan, Italy; L.I. Golbe, Department of Neurology, University of Medicine and Dentistry — Robert Wood Johnson Medical School, New Brunswick, New Jersey, USA; J.W. Langston, Clinical Center for Parkinson’s Disease and Movement Disorders, California Parkinson’s Foundation, San Jose, California, USA; C.D. Marsden, Institute of Neurology, University of London Department of Clinical Neurology, The National Hospital, London, England; J.S. Meyer, Cerebrovascular Research Laboratories, Baylor College of Medicine, Houston, Texas, USA; J.G. Nutt, Department of Neurology, Oregon Health Sciences University School of Medicine, Portland, Oregon, USA; B.J. Sahakian, Section of Old Age Psychiatry, Institute of Psychiatry, The Bethlehem Royal Hospital and the Maudsley Hospital, London, England; M. Sandler, Department of Chemical Pathology, University of London Postgraduate Medical School, Queen Charlotte’s and Chelsea Hospital, London, England; I. Shoulson, Department of Neurology, University of Rochester Medical Center, Rochester, New York, USA.
Rights and permissions
About this article
Cite this article
Chrisp, P., Mammen, G.J. & Sorkin, E.M. Selegiline. Drugs & Aging 1, 228–248 (1991). https://doi.org/10.2165/00002512-199101030-00006
Published:
Issue Date:
DOI: https://doi.org/10.2165/00002512-199101030-00006