
Summary
Abstract
Escitalopram (Cipralex®, Lexapro™), the active S-enantiomer of the racemic selective serotonin reuptake inhibitor (SSRI) citalopram (RS-citalopram), is a highly selective inhibitor of the serotonin transporter protein. It possesses a rapid onset of antidepressant activity, and is an effective and generally well tolerated treatment for moderate-to-severe major depressive disorder (MDD). Pooled analyses from an extensive clinical trial database suggest that escitalopram is consistently more effective than citalopram in moderate-to-severe MDD. Preliminary studies suggest that escitalopram is as effective as other SSRIs and the extended-release (XR) formulation of the serotonin/noradrenaline (norepinephrine) reuptake inhibitor venlafaxine, and may have cost-effectiveness and cost-utility advantages. However, additional longer-term, comparative studies evaluating specific efficacy, tolerability, health-related quality of life and economic indices would be helpful in definitively positioning escitalopram relative to these other agents in the treatment of MDD. Nevertheless, available clinical and pharmacoeconomic data indicate that escitalopram is an effective first-line option in the management of patients with MDD.
Pharmacological Properties
Unlike other SSRIs, escitalopram appears to not only bind to a primary high-affinity site on the serotonin transporter protein, but also to a secondary, lower-affinity allosteric site that is considered to stabilise and prolong drug binding. In vitro, escitalopram was approximately twice as potent as citalopram in inhibiting serotonin reuptake and, in radioligand binding assays, it was more selective than other SSRIs, including citalopram, for the human serotonin transporter protein. Escitalopram has shown no or very low affinity for various other receptors in vitro. In vivo, escitalopram was four times more potent than citalopram at reducing firing activity of presumed serotonergic neurons in the dorsal raphe nucleus in rat brain.
The multiple-dose pharmacokinetic profile of escitalopram is linear across a 10–30 mg/day dosage (20 mg/day is the maximum approved dosage). Steady-state plasma concentrations are achieved after about 7–10 days’ administration of escitalopram 10 mg/day. The absolute oral bioavailability of escitalopram is about 80%, and protein binding, which is independent of escitalopram plasma concentrations, is ≈55%. Concurrent food ingestion has no influence on escitalopram pharmacokinetics. Escitalopram is extensively metabolised in the liver. In vitro, the cytochrome P450 isoenzymes 2C19, 3A4 and 2D6 contribute equally to its metabolism. The main metabolite is S-demethylcitalopram, which is further metabolised to S-didemethylcitalopram. Both metabolites have virtually no serotonin reuptake activity in vivo. Escitalopram and metabolites are primarily renally excreted, with only a small percentage eliminated as unchanged drug. The plasma elimination half-life is ≈27–33 hours.
Escitalopram dosage adjustments are advocated in elderly patients and those with hepatic impairment, and caution should be exercised with escitalopram use in patients with severe renal impairment.
Therapeutic Efficacy
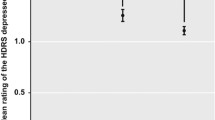
In well designed, comparative studies with placebo and/or citalopram in patients with moderate-to-severe MDD, escitalopram was more effective than placebo and at least as effective as citalopram in reducing the mean Montgomery-Åsberg Depression Rating Scale (MADRS) total score from baseline (primary efficacy parameter). In large, pooled analyses in patients with moderate-to-severe MDD, escitalopram was consistently more effective than placebo or citalopram in terms of a faster onset of antidepressant activity, greater decreases in mean MADRS total score and mean Clinical Global Impression-Severity score, and superior rates of response (percentage of patients with a ≥50% decrease in MADRS score) and remission (percentage of patients attaining a MADRS score ≤12).
Several randomised, double-blind studies in patients with moderate-to-severe MDD showed that escitalopram was as effective as paroxetine, sertraline or venlafaxine XR in reducing MADRS scores.
Escitalopram demonstrated continued efficacy in a 52-week open-label extension of two 8-week double-blind studies in primary-care patients with moderate-to-severe MDD, and significantly prevented relapse in 36- and 52-week double-blind, placebo-controlled studies.
Modelled pharmacoeconomic evaluations and a prospective pharmacoeconomic analysis suggested cost-effectiveness advantages for escitalopram relative to several other SSRIs and venlafaxine (including the XR formulation). Cost utility analyses showed that escitalopram dominated all the other treatments. A potential for cost savings (up to 4.5%) was shown in total healthcare budgets for depression when escitalopram is introduced.
Tolerability
In placebo-controlled studies, the most common treatment-emergent adverse events with escitalopram were nausea (15%), ejaculation disorder (9%), insomnia (9%), diarrhoea (8%), somnolence (7%), dry mouth (6%) and dizziness (6%). Nausea led to withdrawal of 2% of patients and 2% of men withdrew because of ejaculation disorder.
Large-scale comparisons of escitalopram with citalopram revealed that the overall type and incidence of adverse events were generally similar between treatments. Escitalopram demonstrated a lower incidence of nausea, increased sweating and constipation than venlafaxine XR. Discontinuation syndrome (Discontinuation Emergent Signs and Symptoms score increase of ≥4) was seen in fewer escitalopram than venlafaxine XR recipients after treatment withdrawal Likewise, in comparisons with paroxetine, fewer escitalopram recipients had discontinuation syndrome after treatment cessation. The tolerability profile of escitalopram was generally similar to that of fluoxetine in elderly patients and to that of sertraline in patients aged 18–80 years.
A large meta-analysis of data from placebo-controlled studies specific to the use of escitalopram revealed that no suicides with the drug occurred within the first 2 weeks or throughout up to 24 weeks of therapy. In addition, MADRS item-10 (‘suicidal thoughts’) scores were reduced compared with placebo from the first week in 8-week studies. Pharmacovigilance data reveal a very low suicide rate of 1.8 per 1 million patients treated with escitalopram.












Similar content being viewed by others

Notes
The use of trade names is for product identification purposes only and does not imply endorsement.
References
Waugh J, Goa KL. Escitalopram: a review of its use in the management of major depressive and anxiety disorders. CNS Drugs 2003; 17(5): 343–62
Croom K, Plosker GL. Escitalopram: a pharmacoeconomic review of its use in depression. Pharmacoeconomics 2003; 21(16): 1185–209
Eccles M, Freemantle N, Mason J. North of England evidenced-based guide development project: summary version of guidelines for the choice of antidepressants for depression in primary care. The North of England Anti-depressant Guideline Development Group. Fam Pract 1999; 16(2): 103–11
Canadian Psychiatric Association and the Canadian Network for Mood and Anxiety Treatment (CANMAT). Clinical guidelines for the treatment of depressive disorders. Can J Psychiatry 2001; 46 Suppl. 1: 1S–92S
Keller MB. The long-term treatment of depression. J Clin Psychiatry 1999; 60 Suppl. 17: 41–5
Kasper S. From symptoms to social functioning: differential effects of antidepressant therapy. Int Clin Psychopharmacol 1999; 14 Suppl. 1: S27–31
Sullivan PW, Valuck R, Saseen J, et al. A comparison of the direct costs and cost effectiveness of serotonin reuptake inhibitors and associated adverse drug reactions. CNS Drugs 2004; 18(13): 911–32
Fernandez JL, Montgomery S, François C. Evaluation of the cost effectiveness of escitalopram versus venlafaxine XR in major depressive disorder. Pharmacoeconomics 2005; 23(2): 155–67
Institute for Clinical Systems Improvement. Health care guideline: major depression in adults in primary care [online]. Available from URL: http://www.isci.org [Accessed 2005 Jul 17]
National Institute for Clinical Excellence. Depression: management of depression in primary and secondary care. Clinical guideline 23. London: National Institute for Clinical Excellence, 2004 Dec
Norman TR, Olver JS. New formulations of existing antidepressants: advantages in the management of depression. CNS Drugs 2004; 18(8): 505–20
Sánchez C, Bergqvist PB, Brennum LT, et al. Escitalopram, the S-(+)-enantiomer of citalopram, is a selective serotonin reuptake inhibitor with potent effects in animal models predictive of antidepressant and anxiolytic activities. Psychopharmacology (Berl) 2003 Jun; 167(4): 353–62
Forest Laboratories Inc. Lexapro™ (escitalopram oxalate) US prescribing information [online]. Available from URL: http://www.fda.gov [Accessed 2005 Jul 17]
H. Lundbeck AS. Cipralex: European summary of product characteristics [online]. Available from URL: http://www.cipralex.com/images/Cipralex/smpc.pdf [Accessed 2005 Jul 17]
Lundbeck Canada Inc. Annotated prescribing information: escitalopram. Canada: Lundbeck Canada Inc., 2005
Rausch JL, Corley KM, Hobby HM. Improved potency of escitalopram on the human serotonin transporter: demonstration of an ex vivo assay technique. J Clin Psychopharmacol 2004 Apr; 24(2): 209–13
Owens MJ, Knight DL, Nemeroff CB. Second-generation SS-RIs: human monoamine transporter binding profile of escitalopram and R-fluoxetine. Biol Psychiatry 2001; 50: 345–50
Chen F, Larsen MB, Sánchez C, et al. The S-enantiomer of R,S-citalopram, increases inhibitor binding to the human serotonin transporter by an allosteric mechanism. Comparison with other serotonin transporter inhibitors. Eur Neuropsychopharmacol 2005 Mar; 15(2): 193–8
Mørk A, Kreilgaard M, Sánchez C. The R-enantiomer of citalopram counteracts escitalopram-induced increase in extracellular 5-HT in the frontal cortex of freely moving rats. Neuropharmacology 2003 Aug; 45(2): 167–73
Storustovu S, Sánchez C, Porzgen P, et al. R-citalopram functionally antagonises escitalopram in vivo and in vitro: evidence for kinetic interaction at the serotonin transporter. Br J Pharmacol 2004 May; 142(1): 172–80
Sánchez C, Kreilgaard M. R-citalopram inhibits functional and 5-HTP-evoked behavioural responses to the SSRI, escitalopram. Pharmacol Biochem Behav 2004 Feb; 77(2): 391–8
Mitchell PJ, Hogg S. Behavioral effects of escitalopram predict potent antidepressant activity [abstract no. 401]. Biol Psychiatry 2001; 49 Suppl.: 115S
Nadeem HS, Attenburrow MJ, Cowen PJ. Comparison of the effects of citalopram and escitalopram on 5-HT-mediated neuroendocrine responses. Neuropsychopharmacology 2004 Sep; 29(9): 1699–703
Wingen M, Bothmer J, Langer S, et al. Actual driving performance and psychomotor function in healthy subjects after acute and subchronic treatment with escitalopram, mirtazapine, and placebo: a crossover trial. J Clin Psychiatry 2005 Apr; 66(4): 436–43
Sánchez C, Bogeso KP, Ebert B, et al. Escitalopram versus citalopram: the surprising role of the R-enantiomer. Psychopharmacology (Berl) 2004 Jul; 174(2): 163–76
Chen F, Larsen MB, Neubauer HA, et al. Characterization of an allosteric citalopram-binding site at the serotonin transporter. J Neurochem 2005 Jan; 92(1): 21–8
Sánchez C, Gruca P, Papp M. R-citalopram counteracts the antidepressant-like effect of escitalopram in a rat chronic mild stress model. Behav Pharmacol 2003 Sep; 14(5–6): 465–70
El Mansari M, Sánchez C, Chouvet G, et al. Effects of acute and long-term administration of escitalopram and citalopram on serotonin neurotransmission: an in vivo electrophysiological study in rat brain. Neuropsychopharmacology 2005; 30: 1269–77
Ceglia I, Acconcia S, Fracasso C, et al. Effects of chronic treatment with escitalopram or citalopram on extracellular 5-HT in the prefrontal cortex of rats: role of 5-HT1a receptors. Br J Pharmacol 2004 Jun; 142(3): 469–78
Søgaard B, Mengel H, Rao N, et al. The pharmacokinetics of escitalopram after oral and intravenous administration of single and multiple doses to healthy subjects. J Clin Pharmacol. In Press
von Moltke LL, Greenblatt DJ, Giancarlo GM, et al. Escitalopram (S-citalopram) and its metabolites in vitro: cytochromes mediating biotransformation, inhibitory effects, and comparison to R-citalopram. Drug Metab Dispos 2001 Aug; 29(8): 1102–9
Areberg J, Christophersen JS, Poulsen MN, et al. Pharmacokinetics of escitalopram in subjects with hepatic impairment [poster]. 8th World Congress of Biological Psychiatry; 2005 Jun 28–Jul 3; Vienna
Malling D, Poulsen MN, Søgaard B. The effect of cimetidine or omeprazole on the pharmacokinetics of escitalopram in healthy subjects. Br J Clin Pharmacol 2005; 60(3): 287–90
Gutierrez MM, Rosenberg J, Abramowitz W. An evaluation of the potential for pharmacokinetic interaction between escitalopram and the cytochrome P450 3A4 inhibitor ritonavir. Clin Ther 2003 Apr; 25(4): 1200–10
Preskorn SH, Klick-Davis A, Coyner L, et al. The effect of escitalopram versus sertraline versus duloxetine on CYP 2D6 function [abstract no. NR877 plus poster]. New Research Abstracts. American Psychiatric Association 2005 Annual Meeting; 2005 May 21–26; Atlanta (GA), 326
Moore N, Verdoux H, Fantino B. Prospective, multicentre, randomized, double-blind study of the efficacy of escitalopram versus citalopram in outpatient treatment of major depressive disorder. Int Clin Psychopharmacol 2005 May; 20(3): 131–7
Lepola UM, Loft H, Reines EH. Escitalopram (10–20 mg/day) is effective and well tolerated in a placebo-controlled study in depression in primary care. Int Clin Psychopharmacol 2003 Jul; 18: 211–7
Ninan PT, Ventura D, Wang J. Escitalopram is effective and well-tolerated in the treatment of severe depression [abstract no. NR 486 plus poster]. New Research Abstracts: American Psychiatric Association 2003 Annual Meeting; 2003 May 17–22; San Francisco (CA), 182
Forest Laboratories Inc. SCT-MD-26 [online]. Available from URL: http://forestclinicaltrials.com [Accessed 2005 Sep 6]
Burke WJ, Gergel I, Bose A. Fixed-dose trial of the single isomer SSRI escitalopram in depressed outpatients. J Clin Psychiatry 2002 Apr; 63(4): 331–6
Wade A, Lemming OM, Hedegaard KB. Escitalopram 10 mg/ day is effective and well tolerated in a placebo-controlled study in depression in primary care. Int Clin Psychopharmacol 2002 May; 17(3): 95–102
Colonna L, Andersen HF, Reines EH. A randomized, double-blind, 24-week study of escitalopram (10 mg/day) versus citalopram (20 mg/day) in primary care patients with major depressive disorder. Curr Res Med Opin 2005; 21(10): 1659–68
Vaya L, Appaya PM, Hegde RP, et al. Escitalopram versus citalopram and sertraline: a double-blind controlled, multi-centric trial in Indian patients with unipolar depression. Ind J Psychiatry 2004; 46: 333–41
Alexopoulos GS, Gordon J, Zhang D. A placebo-controlled trial of escitalopram and sertraline in the treatment of major depressive disorder [abstract no. 54]. Neuropsychopharmacology 2004; 29 Suppl. 1: 87. Plus poster presented at the 43rd Annual Meeting of the American College of Neuropsychopharmacology; 2004 Dec 12–16; San Juan, Puerto Rico
Baldwin D, Hindmarch I, Huusom AKT. Escitalopram and paroxetine in the short and long-term treatment of major depressive disorder (MDD) [abstract no. P01.135]. Int J Neuropsychopharmacol 2004 Jun 22; 7 Suppl. 1: S 168. Plus poster presented at the 24th Congress of the Collegium Internationale Neuropsychopharmacologicum; 2004 Jun 20–24; Paris
Alexopoulos GS, Privitera W, Ventura D, et al. Fixed dose of escitalopram (10 mg/day) and a flexible dosing regimen of sertraline (50–200 mg/day) in a randomised, double-blind comparison in depressed patients [abstract no. 6257]. World J Biol Psychiatry 2004; 5 Suppl. 1: 97.Plus poster presented at the International Congress of Biological Psychiatry; 2004 Feb 9–13; Sydney
Forest Laboratories Inc. SCT-MD-27 [online]. Available from URL: http://forestclinicaltrials.com [Accessed 2005 Sep 12]
Clayton A, Wightman D, Modell JG, et al. Effects in MDD on sexual functioning of bupropion XL, escitalopram, and placebo in depressed patients [abstract no. NR-818 plus poster]. New Research Abstracts. American Psychiatric Association 2005 Annual Meeting; 2005 May 21–26; Atlanta (GA), 303
Wightman D, Horrigan JP, Modell JG, et al. The tolerability and safety of bupropion XL versus escitalopram in the treatment of major depressive disorder [poster]. 13th Congress of the Association of European Psychiatrists (AEP); 2005 Apr 2–6; Munich
Bielski RJ, Ventura D, Chang CC. A double-blind comparison of escitalopram and venlafaxine extended release in the treatment of major depressive disorder. J Clin Psychiatry 2004 Sep; 65(9): 1190–6
Montgomery SA, Huusom AKT, Bothmer J. A randomised study comparing escitalopram with venlafaxine XR in primary care patients with major depressive disorder. Neuropsychobiology 2004; 50(1): 57–64
Rush AJ, Bose A. Escitalopram in clinical practice: results of an open-label trial in a naturalistic setting. Depress Anxiety 2005; 21(1): 26–32
Möller HJ, Lotze K, Langer S. postmarketing surveillance of escitalopram in depressed outpatients [abstract no. PO-021.10]. World J Biol Psychiatry 2005; 6 Suppl. 1: 282–283. Plus poster presented at the 8th World Congress of Biological Psychiatry; 2005 Jun 28–Jul 3; Vienna
Zimbroff DL, Bose A, Li D. Escitalopram treatment of SSRI nonresponders can lead to remission in patients who fail initial SSRI therapy [abstract no. NR758 plus poster]. 157th Annual Meeting of the American Psychiatric Association: New Research Abstracts; 2004 May 1–6; New York
Wade A, Despiegel N, Reines EH. Escitalopram in the long-term treatment of major depressive disorder. Ann Clin Psychiatry. In Press
Kornstein SG, Bose A, Li D. Maintenance treatment with escitalopram prevents recurrence of depressive episodes [abstract no. NR744 plus poster]. 157th Annual Meeting of the American Psychiatric Association: New Research Abstracts; 2004 May 1–6; New York, 279–80
Rapaport MH, Bose A, Zheng H. Escitalopram continuation treatment prevents relapse of depressive episodes. J Clin Psychiatry 2004 Jan; 65(1): 44–9
Llorca PM, Azorin JM, Despiegel N, et al. Efficacy of escitalopram in patients with severe depression: a pooled analysis. Int J Clin Pract 2005 Mar; 59(3): 268–75
Lepola U, Wade A, Andersen HF. Do equivalent doses of escitalopram and citalopram have similar efficacy? A pooled analysis of two positive placebo-controlled studies in major depressive disorder. Int Clin Psychopharmacol 2004 May; 19(3): 149–55
Auquier P, Robitail S, Llorca PM, et al. Comparison of escitalopram and citalopram efficacy: a meta-analysis. Int J Psychiatry Clin Pract 2003; 7(4): 259–68
Gorman JM, Korotzer A, Su G. Efficacy comparison of escitalopram and citalopram in the treatment of major depressive disorder: pooled analysis of placebo-controlled trials. CNS Spectr 2002 Apr; 7 (4 Suppl. 1): 40–4
Wade A, Andersen HF. Onset of effect of escitalopram; a pooled analysis [poster]. 8th World Congress of Biological Psychiatry; 2005 Jun 28–Jul 3; Vienna
Bandelow B, Anderson HF. Escitalopram in the treatment of anxiety associated with depression [poster]. 8th World Congress of Biological Psychiatry; 2005 Jun 28–Jul 3; Vienna
Einarson TR. Evidence based review of escitalopram in treating major depressive disorder in primary care. Int Clin Psychopharmacol 2004 Sep; 19(5): 305–10
Lader M, Andersen HF, Baekdal T. The effect of escitalopram on sleep problems in depressed patients. Hum Psychopharmacol 2005; 20: 349–54
Kennedy SH, Anderson EA. Short-term efficacy of escitalopram treatment of MDD: a pooled analysis versus SSRIs and venlafaxine [abstract no. NR873 plus poster]. New Research Abstracts. American Psychiatric Association 2005 Annual Meeting; 2005 May 21–26; Atlanta (GA), 325
Bech P, Tanghoj P, Cialdella P, et al. Escitalopram dose-response revisited: an alternative psychometric approach to evaluate clinical effects of escitalopram compared to citalopram and placebo in patients with major depression. Int J Neuropsychopharmacol 2004 Sep; 7(3): 283–90
Wade AG, Toumi I, Hemels MEH. A probabilistic cost-effectiveness analysis of escitalopram, generic citalopram and venlafaxine as a first-line treatment of major depressive disorder in the UK. Curr Med Res Opin 2005 Apr; 21(4): 631–41
Hemels MEH, Kasper S, Walter E, et al. Cost-effectiveness of escitalopram versus citalopram in the treatment of severe depression. Ann Pharmacother 2004 Jun; 38(6): 954–60
Wade AG, Toumi I, Hemels ME. A pharmacoeconomic evaluation of escitalopram versus citalopram in the treatment of severe depression in the United Kingdom. Clin Ther 2005 Apr; 27(4): 486–96
François C, Toumi M, Aakhus AM, et al. A pharmacoeconomic evaluation of escitalopram, a new selective serotonin reuptake inhibitor. Comparison of cost-effectiveness between escitalopram, citalopram, fluoxetine, and venlafaxine for the treatment of depression in Norway. Eur J Health Econ 2003; 4(1): 12–9
Demyttenaere K, Hemels ME, Hudry J, et al. A cost-effectiveness model of escitalopram, citalopram, and venlafaxine as first-line treatment for major depressive disorder in Belgium. Clin Ther 2005 Jan; 27(1): 111–24
Hemels ME, Kasper S, Walter E, et al. Cost-effectiveness analysis of escitalopram: a new SSRI in the first-line treatment of major depressive disorder in Austria. Curr Med Res Opin 2004 Jun; 20(6): 869–78
Löthgren M, Hemels M, François C, et al. A cost-effectiveness analysis of escitalopram as first-line treatment of depression in Sweden. Prim Care Psych 2004; 9(4): 153–61
Hemels M. Probabilistic cost-effectiveness analysis of escitalopram: a new SSRI in the first-line treatment of major depressive disorder in the Netherlands. 5th World Congress of the International Health Economics Association; 2005 Jul 10–13; Barcelona, 140–1
Armstrong EP, Skrepnek GH, Malone DC, et al. A cost-effectiveness analysis of escitalopram and sertraline in the treatment of major depressive disorder [abstract no. PMH28]. Value Health 2005; 8(3): 393
François C, Sintonen H, Toumi M. Introduction of escitalopram, a new SSRI in Finland: comparison of cost-effectiveness between the other SSRIs and SNRI for the treatment of depression and estimation of the budgetary impact. J Med Econ 2002; 5: 91–107
Kulp W, Greiner W, Schulenburg JM. Cost-effectiveness of escitalopram vs. venlafaxine XR in the treatment of major depressive disorder in Germany [abstract no. PMH27]. Value Health 2005; 8(3): 392–3. Plus poster presented at ISPOR 10th Annual Meeting; 2005 May 15–18; Washington, DC
Rosenbaum JF, Fava M, Hoog SL, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial. Biol Psychiatry 1998; 44: 77–87
Baldwin DA, Montgomery SA, Nil R, et al. Discontinuation symptoms in affective disorders [poster]. 8th World Congress of Biological Psychiatry; 2005 Jun 28–Jul 3; Vienna
Kasper S, de Swart H, Anderson HF, et al. Escitalopram in the treatment of depressed elderly patients. Am J Ger Psychiatr. In Press
Gersing K, Taylor L, Mereadith C. Outcomes and adverse events for escitalopram and sertraline in a real-world setting [abstract no. NR815 plus poster]. New Research Abstracts. American Psychiatric Association 2005 Annual Meeting; 2005 May 21–26; Atlanta (GA)
Ashton AK, Mahmood A, Iqbal F. Improvements in SSRI/ SNRI-induced sexual dysfunction by switching to escitalopram. J Sex Marital Ther 2005; 31: 257–62
Gunnell D, Saperia J, Ashby D. Selective serotonin reuptake inhibitors (SSRIs) and suicide in adults: meta-analysis of drug company data from placebo controlled, randomised controlled trials submitted to the MHRA’s safety review. BMJ 2005; 330: 385–8
Pedersen AG. Escitalopram and suicidality in adult depression and anxiety. Int Clin Psychopharmacol 2005 May; 20(3): 139–43
Magnuson TM, Burke WJ. Clinical experience with escitalopram, a stereoisomer antidepressant. Todays Ther Trends 2003; 21(2): 117–26
Ellis P. Australian and New Zealand clinical practice guidelines for the treatment of depression. Aust N Z J Psychiatry 2004 Jun; 38(6): 389–407
Ashton AK. Reversal of fluoxetine-induced sexual dysfunction by switching to escitalopram [letter]. J Sex Marital Ther 2004; 30: 1–2
US Food and Drug Administration. FDA talk paper: FDA reviews data for antidepressant use in adults [online]. Available from URL: http://www.fda.gov/bbs/topics/ANSWERS/2005/ANS01362.html [Accessed 2005 Sep 9]
Acknowledgements
At the request of the journal, H. Lundbeck A/S provided a non-binding review of this article.
Author information
Authors and Affiliations
Corresponding author
Additional information
Various sections of the manuscript reviewed by: T.R. Einarson, Lesley Dan Faculty of Pharmacy, University of Toronto, Toronto, Ontario, Canada; G. Guzzo, Lesley Dan Faculty of Pharmacy, University of Toronto, Toronto, Ontario, Canada; N. Haddjeri, Faculty of Pharmacy, Claude Bernard University, Lyon, France; H. Koponen, Department of Psychiatry, University of Oulu, Oulu, Finland; U. Lepola, Psychiatric Research Clinic of Kuopio, Helsinki and Oulu University, Helsinki, Finland; M. Machado, Lesley Dan Faculty of Pharmacy, University of Toronto, Toronto, Ontario, Canada; P. Marr, Lesley Dan Faculty of Pharmacy, University of Toronto, Toronto, Ontario, Canada; T.R. Norman, Department of Psychiatry, University of Melbourne, Austin Hospital, Heidelberg, Victoria, Australia.
Data Selection
Sources: Medical literature published in any language since 1980 on escitalopram, identified using MEDLINE and EMBASE, supplemented by AdisBase (a proprietary database of Adis International). Additional references were identified from the reference lists of published articles. Bibliographical information, including contributory unpublished data, was also requested from the company developing the drug.
Search Strategy: MEDLINE search terms were ‘escitalopram’ and ‘depression’. EMBASE search terms were ‘escitalopram’ and ‘depression’. AdisBase search terms were ‘escitalopram’ or ‘S-citalopram’ and ‘depression’. Searches were last updated 12 October 2005.
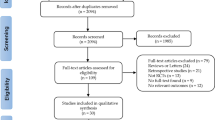
Selection: Studies in patients who received escitalopram. Inclusion of studies was based mainly on the methods sections of trials. When available, large, well controlled trials with appropriate statistical methodology were preferred. Relevant pharmacodynamic, pharmacokinetic, and pharmacoeconomic data are also included.
Index Terms: Escitalopram, depression, major depressive disorder, pharmacodynamics, pharmacokinetics, therapeutic efficacy, pharmacoeconomics, tolerability.
Rights and permissions
About this article
Cite this article
Murdoch, D., Keam, S.J. Escitalopram. Drugs 65, 2379–2404 (2005). https://doi.org/10.2165/00003495-200565160-00013
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003495-200565160-00013