
Abstract
Background: Osteoporosis is a condition marked by low bone mineral density and the deterioration of bone tissue. One of the main clinical and economic consequences of osteoporosis is skeletal fractures.
Objective: To assess the healthcare and work loss costs of US patients with non-vertebral (NV) osteoporotic fractures.
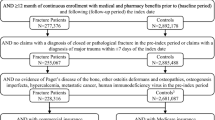
Methods: Privately insured (aged 18–64 years) and Medicare (aged ≥65 years) patients with osteoporosis (ICD-9-CM code: 733.0x) were identified during 1999–2006 using two claims databases. Patients with an NV fracture (femur, pelvis, lower leg, upper arm, forearm, rib or hip) were matched randomly on age, sex, employment status and geographic region to controls with osteoporosis and no fractures. Patient characteristics and annual healthcare costs were assessed over the year following the index fracture for privately insured (n = 4764) and Medicare (n = 48 742) beneficiaries (Medicare drug costs were estimated using multivariable models). Indirect (i.e. work loss) costs were calculated for a subset of privately insured, employed patients with available disability data (n = 1148). All costs were reported in $US, year 2006 values.
Results: In Medicare, mean incremental healthcare costs per NV fracture patient were $US13 387 ($US22 466 vs $US9079; p < 0.05). The most expensive patients had index fractures of the hip, multiple sites and femur (incremental costs of $US25 519, $US20 137 and $US19 403, respectively). Patients with NV non-hip (NVNH) fractures had incremental healthcare costs of $US7868 per patient ($US16 704 vs $US8836; p < 0.05). Aggregate annual incremental healthcare costs of NVNH patients in the Medicare research sample (n = 35 933) were $US282.7 million compared with $US204.1 million for hip fracture patients (n = 7997).
Among the privately insured, mean incremental healthcare costs per NV fracture patient were $US5961 ($US11 636 vs $US5675; p < 0.05). The most expensive patients had index fractures of the hip, multiple sites and pelvis (incremental costs of $US13 801, $US9642 and $US8164, respectively). Annual incremental healthcare costs per NVNH patient were $US5381 ($US11 090 vs $US5709; p < 0.05). Aggregate annual incremental healthcare costs of NVNH patients in the privately insured sample (n = 4478) were $US24.1 million compared with $US3.5 million for hip fracture patients (n = 255). Mean incremental work loss costs per NV fracture employee were $US1956 ($US4349 vs $US2393; p < 0.05). Among patients with available disability data, work loss accounted for 29.5% of total costs per NV fracture employee.
Conclusion: The cost burden of NV fracture patients to payers is substantial. Although hip fracture patients were more costly per patient in both Medicare and privately insured samples, NVNH fracture patients still had substantial incremental costs. Because NVNH patients accounted for a larger proportion of the fracture population, they were associated with greater aggregate incremental healthcare costs than hip fracture patients.








Similar content being viewed by others


References
The World Health Organization Scientific Group. Prevention and management of osteoporosis [technical report series no. 921]. Geneva, Switzerland: WHO, 2003
National Osteoporosis Foundation. Osteoporosis fast facts [online]. Available from URL: http://www.nof.org/osteoporosis/diseasefacts.htm [Accessed 2009 Mar 6]
National Institute of Arthritis and Musculoskeletal and Skin Diseases. Fact sheets: osteoporosis overview [online]. Available from URL: http://www.niams.nih.gov/Health_Info/Bone/Osteoporosis/default.asp [Accessed 2009 Mar 6]
Pasco JA, Sanders KM, Hoekstra FM, et al. The human cost of fracture. Osteoporos Int 2005 Dec; 16 (12): 2046–52
Srivastava M, Deal C. Osteoporosis in elderly: prevention and treatment. Clin Geriatr Med 2002; 18: 529–55
Burge R, Dawson-Hughes B, Solomon DH, et al. Incidence and economic burden of osteoporosis-related fractures in the United States, 20052025. J Bone Miner Res 2007; 22: 465–75
Tosteson AN, Gabriel SE, Grove MR, et al. Impact of hip and vertebral fractures on quality-adjusted life years. Osteoporos Int 2001; 12: 1042–9
Boonen S, Singer AJ. Osteoporosis management: impact of fracture type on cost and quality of life in patients at risk for fracture I. Curr Med Res Opin 2008; 24 (6): 1781–8
Melton LJ, Gabriel SE, Crowson CS, et al. Cost-equivalence of different osteoporotic fractures. Osteoporos Int 2003; 14: 383–8
Orsini LS, Rousculp MD, Long SR, et al. Health care utilization and expenditures in the United States: a study of osteoporosis- related fractures. Osteoporos Int 2005; 16: 359–71
Ray NF, Chan JK, Thamer M, et al. Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995: report from the National Osteoporosis Foundation. J Bone Miner Res 1997; 10 (1): 24–35
Melton LJ. Adverse outcomes of osteoporotic fractures in the general population. J Bone Miner Res 2003 Jun; 18 (6): 1139–41
Ohlsfeldt RL, Borisov NN, Steer RL. Fragility fracturerelated direct medical costs in the first year following a nonvertebral fracture in a managed care setting. Osteoporosis Int 2006; 17: 252–8
Centers for Medicare and Medicaid Services. Medicare enrollment — aged beneficiaries: as of July 2006 [online]. Available from URL: http://www.cms.hhs.gov/MedicareEnRpts/Downloads/06Aged.pdf [Accessed 2009 Mar 9]
National Economic Council/Domestic Policy Council. America’s seniors and Medicare: challenges for today and tomorrow [online]. Available from URL: http://clinton5.nara.gov/media/pdf/med_exec_summ_2000.pdf [Accessed 2009 Mar 9]
Purcell P. Older workers: employment and retirement trends. CRS report for Congress, updated September 7, 2007 [online]. Available from URL: http://opencrs.cdt.org/rpts/RL30629_20070907.pdf [Accessed 2009 Mar 9]
Owen RA, Melton 3rd LJ, Gallagher JC, et al. The national cost of acute care of hip fractures associated with osteoporosis. Clin Orthop Relat Res 1980 Jul-Aug; 150: 172–6
Martin BC, Chisholm MA, Kotzan JA. Isolating the cost of osteoporosis-related fracture for postmenopausal women: a population-based study. Gerontology 2001 Jan-Feb; 47 (1): 21–9
Lindsay R, Burge RT, Strauss M. One year outcomes and costs following a vertebral fracture. Osteoporos Int 2005; 16: 78–85
Chrischilles E, Shireman T, Wallace R. Costs and health effects of osteoporotic fractures. Bone 1994 Jul-Aug; 15 (4): 377–86
King AB, Saag KG, Burge RT, et al. Fracture Reduction Affects Medicare Economics (FRAME): impact of increased osteoporosis diagnosis and treatment. Osteoporos Int 2005; 16: 1545–57
Zethraeus N, Borgstrom F, Johnell O, et al. Costs and quality of life associated with osteoporosis related fractures: results from a Swedish survey [Working Paper Series in Economics and Finance 2002, no. 512; online]. Available from URL: http://swopec.hhs.se/hastef/abs/hastef0512.htm [Accessed 2009 Sep 10]
Levy P, Levy E, Audran M, et al. The cost of osteoporosis in men: the French situation. Bone 2002 Apr; 30 (4): 631–6
Bouee S, Lafuma A, Fagnani F, et al. Estimation of direct unit costs associated with non-vertebral osteoporotic fractures in five European countries. Rheumatol Int 2006 Oct; 26 (12): 1063–72
Chen Z, Maricic M, Aragaki AK, et al. Fracture risk increases after diagnosis of breast or other cancers in postmenopausal women: results from the Women’s Health Initiative. Osteoporos Int 2009 Apr; 20 (4): 527–36
Abelson A. A review of Paget’s disease of bone with a focus on the efficacy and safety of zoledronic acid 5mg. Curr Med Res Opin 2008 Mar; 24 (3): 695–705
Blouin S, Libouban H, Moreau MF, et al. Orchidectomy models of osteoporosis. Methods Mol Bio 2008; 455: 125–34
Hasselman CT, Vogt MT, Stone KL, et al. Foot and ankle fractures in elderly white women: incidence and risk factors. J Bone Joint Surg Am 2003 May; 85-A (5): 820–4
Kaye RA. Insufficiency stress fractures of the foot and ankle in postmenopausal women. Foot Ankle Int 1998 Apr; 19 (4): 221–4
Siris ES, Miller PD, Barrett-Connor E, et al. Identification and fracture outcomes of undiagnosed low bone mineral density in postmenopausalwomen: results from theNational Osteoporosis Risk Assessment. JAMA 2001; 286: 2815–22
Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40 (5): 373–83
Romano PS, Roos LL, Jollis J. Adapting a clinical comorbidity index for use with ICD-9-CM administrative data. J Clin Epidemiol 1993; 46 (10): 1075–9
Akobundu E, Ju J, Blatt L, et al. Cost-of-illness studies: a review of current methods. Pharmacoeconomics 2006; 24 (9): 869–90
Rousculp MD, Long SR, Wang S, et al. Economic burden of osteoporosis-related fractures in Medicaid. Value Health 2007; 10 (2): 144–52
Gunter MJ, Beaton SJ, Brenneman SK, et al. Management of osteoporosis in women aged 50 and older with osteoporosis- related fractures in a managed care population. Dis Manag 2003 Summer; 6 (2): 83–91
Sasser AC, Rousculp MD, Birnbaum HG, et al. Economic burden of osteoporosis, breast cancer, and cardiovascular disease among postmenopausal women in an employed population. Womens Health Issues 2005 May-Jun; 15 (3): 97–108
Acknowledgements
This research project was funded by Eli Lilly and Company. Drs Russel Burge and Eric Edgell are employees of Eli Lilly and Company in the Global Health Outcomes department. Eli Lilly and Company markets pharmacological therapies for the prevention and treatment of osteoporosis.
The authors thank Susan Dennett of Eli Lilly and Company for her contributions to the study design. The authors also thank Anna Gu for providing computer programming input on various aspects of the analysis.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Rights and permissions
About this article
Cite this article
Pike, C., Birnbaum, H.G., Schiller, M. et al. Direct and Indirect Costs of Non-Vertebral Fracture Patients with Osteoporosis in the US. Pharmacoeconomics 28, 395–409 (2010). https://doi.org/10.2165/11531040-000000000-00000
Published:
Issue Date:
DOI: https://doi.org/10.2165/11531040-000000000-00000