

Talha M Siddiqui                                         BDS, MCPS
Aisha Wali2Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â BDS, MPH
Mortaza Azimi3Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â BDS
Tawoos Salehi4Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â BDS
Sohaib Mahmood Siddiqui5Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â BDSÂ Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â
OBJECTIVE: The objective of the present study was to assess the relationship between socioeconomic status and Dental caries in patients attending Out Patient Department of Baqai Dental College.
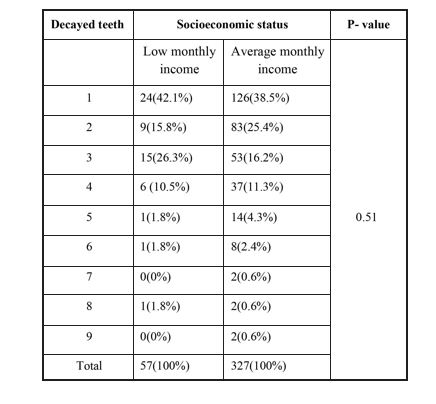
METHODOLOGY: A cross sectional study was conducted in the Department of Oral Diagnosis, Baqai Dental College from 26th April 2017 to17th December. A structured questionnaire was developed and demographic profile, socioeconomic status, residence and decayed teeth were recorded. Data was analyzed for frequency and percentages of different variables and chi- square test was used to check for association between the variables by using IBM SPSS version 22. RESULTS: The present study reported that out of 327 patients, 189(57.8%) belonged to rural area with an average monthly income. One hundred and twenty six (38.5%) of patients with an average monthly income, and 24(42.1%) from low monthly income, each reported only one decayed teeth.
CONCLUSION: The present study reported an inverse relationship between socioeconomic status and dental caries. The number of patients from low socioeconomic status showed less number of decayed teeth.
KEY WORDS: Dental caries, income, socioeconomic status, teaching hospital.
HOW TO CITE: Siddiqui TM, Wali A, Azimi M, Salehi T, Siddiqui SM. Socioeconomic status and dental caries: exploring the relation in patients visiting dental teaching hospital, karachi. J Pak Dent Assoc 2019;28(1):27-32. DOI: https://doi.org/10.25301/JPDA.281.27
Received: 17 August 2018, Accepted: 27 November 2018
INTRODUCTION
Social inequalities in health and oral health outcomes are measured by level of education, profession, monthly earnings and type of housing or combination of various indicators.1,2 Current evidences suggested that lower the standard of living, the worsen the health status that could be irrespective of the measure.1-4 When compared to adult populations, social differences in general health and oral health amongst children and adolescents have received relatively little attention.5 Socioeconomic status is classified into three categories, high socioeconomic status, moderate socioeconomic status and low socioeconomic status.
Oral health is an important part of general health and numerous studies reported an association between socioeconomic factors and oral health.7-12 Dental caries is one of the most common infectious diseases despite of its widespread preventive measures, this disease exerts a social, physical, mental and financial burden globally especially in developing countries.13 Although frequency of dental caries has declined in the past decades amongst adolescents and adults14,15 but still the burden remains high in underprivileged and adult populations. Waseem F16 in a study reported an association between the frequency of dental visits and the socioeconomic status. Amin M et al17 in a study reported an association between Dental caries and socioeconomic status. Schwendicke et al18 reported that adults with lower educational level or lower monthly earnings were more likely to fall in the category of higher risk of dental caries. There is an intricate association between socioeconomic status and oral health18-20 Hobdell et al21 in a study also reported a marked relationship between oral diseases and socioeconomic status. The results from the previous studies reported that people from low socioeconomic status have poor oral health than those with a higher socioeconomic status and that oral health deteriorate gradually from higher socioeconomic status to lower socioeconomic status.22,23 Low socioeconomic status, low monthly household earnings and low educational level are associated with least access to dental health facilities and oral hygiene products, poorer knowledge regarding oral and dental health and subsequently a greater frequency and severity of dental caries.24
The aim of the present study was to assess the relation between socioeconomic status and Dental caries in patients attending Out Patient Department of Baqai Dental College.
METHODOLOGYÂ
A cross sectional study was conducted in the Department of Oral Diagnosis, Baqai Dental College from 26th April 2017 to17th December 2017. The study was approved by Ethical Committee, Baqai Medical University. The sample size was calculated by taking 50% prevalence rate and computed using Open Epi version 3.03a at 95% confidence interval and a =5%. The sample size calculated was 384. The subjects were conveniently selected for the purpose of this study. Patients aged 18-45 years from all socioeconomic status were included in the study.6
Oral examination was conducted by two calibrated, trained examiners according to WHO criteria.24 Dental caries was recorded by using plain mouth mirror, Community Periodontal Index (CPI) probe with the patient seated on a dental chair. All teeth were examined in a systematic manner using international FDI nomenclature to identify each tooth. The patients were asked to rinse mouth thoroughly before intraoral examination starts and the teeth were then dried with cotton swab and dental caries was recorded using the DMFT index corresponding to the average number of decayed, missing and filled permanent teeth. A structured questionnaire was developed which included questions regarding decayed teeth, self-earners, house ownership, periodic loan dental visits, brushing habits.
Data was analyzed for frequency and percentages of different variables and chi square test was used to check for association between residence and socioeconomic status, decayed teeth and socioeconomic status by using IBM SPSS version 22. P- value was set at 0.05
RESULTS
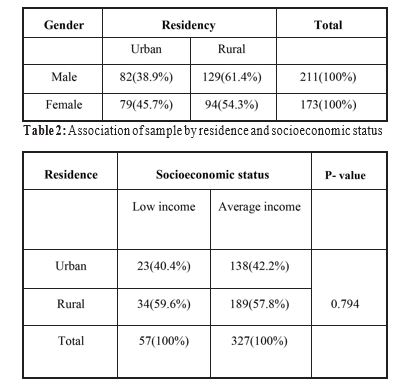
A total of 384 patients (211 males and 173 females) were examined with the response rate of 100%. (Table 1)
Socioeconomic status was divided into low monthly income, average monthly income and high monthly income. Table 2 showed association of residence with socioeconomic status and out of 327 patients, 189(57.8%) belonged to rural area with an average monthly income. Distribution of decayed teeth and its association with socioeconomic status was reported in table 3 and 126(38.5%) of patients from an average monthly income, and 24(42.1%) from low monthly income, each reported only one decayed teeth. Association of socioeconomic status with different variables was shown in Table 4, 273 (83.5%) of patients were self -earners, 269(82.2%) from average monthly income had their own house, 206(63%) of the patients from average SES were too much concerned about their dental health, 214(65.4%) of the patients from average SES reported that there is a dental facility near their house.
Table 1: Distribution of gender and residence
DISCUSSION
The present study reported an inverse relationship between socioeconomic status and dental caries. Socioeconomic factors are key determinants of oral health inequalities.25 Numerous studies have shown inverse relationship between socioeconomic status and prevalence of dental diseases and as socioeconomic status increases, the incidence and prevalence of  dental diseases and their consequences decreases, while on the other hand, the individuals with low socio-economic status have poor oral conditions.26 Amin et al17 in a study reported that monthly income level has no statistically significant association with decayed teeth. The present study reported that dental caries was more seen in individuals with average monthly income. Carmichael et al27 were unable to report statistically significant effect of monthly income and prevalence of dental caries. Wang et al28 in a study reported that participants with higher monthly earnings had lower prevalence of dental caries. Low monthly earnings has been closely associated with lower level of education29 and thus poor people display lack of knowledge of caries prevention with higher frequency of dental caries.30 It was reported in the present study that about 15% of the families were from low monthly income (< 10,000) and 85% of the families were from average monthly income (> 10,000). 126(38.5%) of the patients from average monthly income and 24(42.1%) of patients from low monthly income reported only one decayed tooth. Kattula D et al31 in a study reported 60% of the families in the area earned an income of less than Rs 5000 per month and only 2% of the households had a family income more than Rs.20000 per month. Sixty three percent of the families resided in permanent houses and 10.8% had crude or raw houses. The present study reported that 269(82.2%) of the patients from average monthly income owned houses and 35(62.5%) of the patients from low monthly income owned houses. Chandra Shekar B et al32 in a study reported that prevalence of dental caries was 29(43.3%) from upper socioeconomic status and 8(78.6%) from low socioeconomic status.
Factors that are associated with dental caries includes demographic profile, food intake , fluoride usage and access to oral and dental health care services.14,33 Results of some studies showed the effects of socioeconomic factors on oral health-related behaviours in adolescents and adults.34,35 Ashok B et al36 in a study reported that 91.8% of the patients in the lower socioeconomic status have a caries exposure, while only 82% and 73.4% of the moderate and higher socioeconomic status respectively. Waseem F et al16 in a study reported that tooth brushing was more frequent amongst high socioeconomic status whereas low socioeconomic subjects did not regularly brushed their teeth. Rasidi M et al37 in a study reported that dental caries from the low socioeconomic status was higher when compared to the patients belonging to average socioeconomic status. Wang et al28 in a study reported that only 32.8% of the patients brushed their teeth at least twice a day and only 1.2% flossed their teeth. The present study reported that 192(59.1%) of the patients from average monthly income brushed their teeth once a day and 35(61.4%) from low monthly income. Alvarez L et al38 reported that prevalence of dental caries was 55.9% and 28.9% in adults and elderly people, respectively. Severity of dental caries was related to older age individuals, low socioeconomic status, use of dental public health services, lack of frequent brushing, gingival bleeding, and self-perceived need for dental health care services.39
Attitudes towards oral health depends on their socioeconomic status. In the presence of high-socio economic status, better oral health is experienced, and lower dental caries rates are observed.40 The dental visits are important as oral diseases can be diagnosed, managed, and even avoided on time, and personal oral hygiene guidelines can be constantly reminded to dental practice visitors.41-47 Some studies have highlighted that low-socioeconomic status families visit a dentist more frequently due to pain or discomfort.48-50 Waseem F et al16 in a study reported statistically significant results observed between frequencies of dental visits with socioeconomic status. It has been reported that people from low socioeconomic status were less likely to have dental visits to a dental care specialist.51-53Â The present study reported that 69(21.1%) of the patients from average monthly income often visits dental clinics once in 3 months and 258(78.9%) visited once in 6 months.
LIMITATIONS
The present study was limited around certain aspects which included inequality in the sample size. The sample should be collected on a larger scale. The measurement of socioeconomic status and monthly income was missing.
CONCLUSION
The present study reported an inverse relationship between socioeconomic status and dental caries. The number of patients from low socioeconomic status showed less number of decayed teeth.
CONFLICT OF INTEREST
None to declare
REFERENCES
- Locker Deprivation and oral health: a review. Community Dent Oral Epidemiol 2000;28:161-69.https://doi.org/10.1034/j.1600-0528.2000.280301.x
- Watt From victim blamimg to upstream action: tackling the social determinants of oral health inequalities. Community Dent Oral Epidemiol 2007;35:1-11.https://doi.org/10.1111/j.1600-0528.2007.00348.xÂ
- Sabbah W, Tsakos G, Chandola T, Sheiham A, Watt RG: Social gradients in oral and general health. J Dent Res 2007;86:992-96. https://doi.org/10.1177/154405910708601014Â
- Torsheim T, Leversen I, Samdal O: Adolescent health inequality: are behavioral factors important? Nor J Epidemiol 2007;17:79-8.
- Polk DE, Weyant RJ, Manz MC: Socio-economic factors in adolescents’oral health: are they mediated by oral hygiene behaviors or preventive interventions? Community Dent Oral Epidemiol 2010; 38:1-9.https://doi.org/10.1111/j.1600-0528.2009.00499.x Afshan S. Defining income groups. dawn.com.
- Petridou E, Athanassouli T, Panagopoulos H, Revinthi K. Socio- demographic and dietary factors in relation to dental health among Greek Community Dent Oral Epidemiol 1996;24:307-11. https://doi.org/10.1111/j.1600-0528.1996.tb00867.xÂ
- Friere MD, Melo DR, Silva Dental caries prevalence in relation to socio-economic status of nursery school children in Goiania-GO, Brazil. Community Dent Oral Epidemiol 1996;24:357-61. https://doi.org/10.1111/j.1600-0528.1996.tb00876.x
- Whittle JG, Whittle House hold income in relation to dental health and dental health behaviors: The use of super profiles. Community Dent Health 1998;15:150-54.
- Hosani EA, Rugg-Gunn Combination of low parental educational attainment and high parental income related to high caries experience in pre-school children in Abu-Dhabi. Community Dent Oral Epidemiol 1998;26:31-6.https://doi.org/10.1111/j.1600-0528.1998.tb02080.x
- Text book of clinical pedodontics. 4th ed. USA: WB Saunders Company; 1991. p. 470.
- Cameron A, Widmer R. Handbook of pediatric dentistry. 3rd ed. Mosby Elsevier;
- Pitts N, Amaechi B, Niederman R, et Global oral health inequalities: dental caries task group-research agenda. Adv Dent Res 2011;23:211-20.https://doi.org/10.1177/0022034511402016Â
- Do LG, Lg Distribution of caries in children: variations between and within populations. J Dent Res 2012;91:536-43. https://doi.org/10.1177/0022034511434355Â
- Waseem F, Hussain A, Maqsood A, Sultan M. Socioeconomic status and oral health care attitudes: A snapshot of Karachi based teaching hospital. Pak Oral & Dent J. 2015;35:49-52.
- Amin M, Amanullah M, Tarar AM. Dental Caries, Periodontal Disease and their Associated Factors Among Patients Visiting Dental Teaching Hospital in Multan, Pakistan. J Pak Dent Assoc 2016;25: 98-102.
- Schwendicke F, Dörfer CE, Schlattmann P, et al. Socioeconomic inequality and caries: a systematic review and meta-analysis. J Dent Res 2015;94:10-18.https://doi.org/10.1177/0022034514557546Â
- Listl Income-related inequalities in dental service utilization by Europeans aged 50+. J Dent Res 2011;90:717-23. https://doi.org/10.1177/0022034511399907
- Han DH, Khang YH, Choi HJ. Association of parental education with tooth loss among Korean Elders. Community Dent Oral Epidemiol 2015;43:489-99.https://doi.org/10.1111/cdoe.12172Â
- Hobdell MH, Oliveira ER, Bautista R, et al. Oral diseases and socio-economic status (SES). Br Dent J 2003;194:91-6. https://doi.org/10.1038/sj.bdj.4809882Â
- Steele J, Shen J, Tsakos G, et The Interplay between socioeconomic inequalities and clinical oral health. J Dent Res 2015; 94:9-26.https://doi.org/10.1177/0022034514553978Â
- Kim DW, Park JC, Rim TT, et al. Socioeconomic disparities of periodontitis in Koreans based on the KNHANES Oral Dis 2014; 20:551-9.https://doi.org/10.1111/odi.12168
- Holst , Schuller A.A., Aleksejuniené J., Eriksen H.M. Caries in population-A theoretical, causal approach. Eur. J. Oral Sci. 2001;109: 143-8.https://doi.org/10.1034/j.1600-0722.2001.00022.xÂ
- World Health Organization. Oral Health Assessment form. Oral Health Surveys, Basic 4th ed. Geneva: W H O press; 1997. p. 26-9.
- British Dental Association. Oral health inequalities London: British Dental Association, 2009. http://www.bda.org/inequalities (accessed March 2013).
- Carmichael , French A., Rugg-Gunn A., Furness JA.: The relationship between social class and caries experience in five years old children in Newcastle and Northumberland after twelve years’ fluoridation. Community Dent. Health;1984;1:47 -54.
- Wang, L., Cheng, L., Yuan, , Hong, X., & Hu, T. Association between socio-economic status and dental caries in elderly people in Sichuan Province, China: a cross-sectional study. Brit Med J Open, 2017. 7, e016557.https://doi.org/10.1136/bmjopen-2017-016557Â
- Kattula D, Venugopal S, Velusamy V, et al. Measuring Poverty in Southern India: A Comparison of Socio-Economic Scales Evaluated against Childhood Stunting. Zeeb H, PLoS ONE. 2016;11(8):e0160706. https://doi.org/10.1371/journal.pone.0160706Â
- Chandra Shekar B R, Reddy C. Oral health status in relation to socioeconomic factors among the municipal employees of Mysore Indian J Dent Res 2011;22:410-18. https://doi.org/10.4103/0970-9290.87063Â
- Cornejo-Ovalle M, Paraje G, Vásquez-LavÃn F, et al. Changes in socioeconomic inequalities in the use of dental care following major healthcare reform in Chile, 2004-2009. Int J Environ Res Public Health 2015;12:2823-36.
- https://doi.org/10.3390/ijerph120302823