
Beyond the Guidelines: The Grey Zones of the Management of Gastric Cancer. Consensus Statements from the Gastric Cancer Italian Network (GAIN)

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
3. Results
3.1. Role of Multidisciplinary Team
3.1.1. Statements
3.1.2. Sources of Evidence
3.2. Risk Factors
3.2.1. Precancerous Conditions: Chronic Gastritis with Intestinal-Type Metaplasia, Chronic Atrophic Gastritis
Statements
- (1)
- An esophagogastroduodenoscopy (EGDS) should be performed on all patients presenting with new onset dyspeptic symptoms, regardless of the presence of gastroesophageal reflux or other risk factors such as active smoking or H. pylori positivity. Population screening is recommended in Asian countries but there is no evidence to support it in Western populations.
- (2)
- Early identification of patients with chronic atrophic gastritis and intestinal metaplasia (including Barrett) is fundamental to endoscopic staging by the updated Sydney system, with an accurate assessment of the degree of atrophy/metaplasia with OLGA (Operative Link on Gastritis Assessment) and OLGIM (Operative Link on Gastritis/Intestinal-Metaplasia Assessment) classification systems.
- (3)
- Endoscopic surveillance of precancerous lesions must be guided by both severity of the histologic finding and the extent and association of other risk factors such as familial gastric neoplasia, autoimmune gastritis, Barrett, and non-eradication of H. pylori infection. Endoscopic surveillance is recommended every 3 years in patients with intestinal metaplasia limited to the antrum or gastric body, mainly for patients with familial gastric neoplasia, autoimmune gastritis, or non-eradication of H. pylori infection. In patients with chronic atrophic gastritis and/or diffuse intestinal metaplasia, endoscopic follow-up every 1–2 years is recommended.
Sources of Evidence
3.2.2. Family History of Gastric Cancer and Hereditary Gastric Cancer (HDGC and Other Syndromes)
Statements
- (1)
- Genetic testing is recommended if: there is family history of ≥2 cases of gastric cancer at any age, in first- or second-degree relatives, with ≥1 diffuse histology; a diagnosis of diffuse gastric cancer before age 40 years; or in families with both diffuse gastric cancer and lobular breast cancer with a case identified before age 50 years.
- (2)
- Genetic testing should also be considered for all patients with a diagnosis of gastric neoplasia and a family history compatible with Lynch syndrome, FAP, Peutz–Jeghers, Li–Fraumeni, juvenile polyposis, hereditary breast and ovarian cancer syndrome (germline mutations in BRCA1 or BRCA2).
Sources of Evidence
3.3. Diagnostic and Staging Work-Up
3.3.1. Pathologic Evaluation: Minimum Requirements for Diagnosis and Staging of Gastric Cancer
Statements
- A histopathologic diagnosis on primary tumor requires at least 6 biopsy samples (optimal 6–8 because of intratumoral heterogeneity).
- The biopsy specimen report should contain histotype according to WHO classification, expressing the presence and possible percentage of SRC component, Lauren classification, and grading. The surgical anatomopathologic report should contain: macroscopic description of the lesions and sites (primitive/lymph nodes/any other samples), microscopic description including WHO classification, Lauren classification, grading, staging according to the most up-to-date TNM (Tumor-Nodes-Metastasis) version, margin status, lymphovascular and perineural invasion, tumor regression grading (TRG) according to Becker or Mandard after neoadjuvant treatments. Metastatic LNFs (lymph nodes)/total LNFs for every lymph node station should be identified by the surgeon, or at least perigastric lymph nodes (stations 1–7) should be distinguished from extraperigastric lymph nodes (stations 8–12 and 12–16).
- Microsatellite instability (MSI) should be reported for both operable and metastatic disease, HER2-status assessment is mandatory in metastatic disease and could be reported for localized disease. HER2 status should be determined by immunohistochemistry (IHC) and/or FISH (fluorescence in-situ hybridization) in all patients with metastatic cancer before first-line chemotherapy. HER2 status should preferably be determined on metastatic localization (if a result is not already available) or surgical sample, because of intratumoral heterogeneity, but can also be performed on gastric biopsy, in which case at least five samples must be evaluated for a correct determination.
- Determining PD-L1 expression is not yet mandatory but could be in the future if immunotherapy approval processes require combined positive score (CPS) for prescriptive purposes.
- The panel recognizes that NTRK (neurotrophic receptor tyrosine kinase) 1, 2, or 3 genes fusion may be targeted by EMA-approved agnostic drugs such as larotrectinib or entrectinib. These alterations may be identified by immunohistochemistry or nucleic acid-based techniques. However, incidence of gene fusion is low (<1%) in gastroesophageal cancer [33,34,35,36], particularly among Caucasian patients [37], and diagnostic techniques may be not routinely available at all institutions. Therefore, screening of NTRK gene fusion cannot be universally recommended, but is encouraged for pretreated patients without validated therapeutic alternatives [38,39,40,41,42].
Sources of Evidence
3.4. Preoperative Staging
3.4.1. The Role of Endoscopic Ultrasound
Statements
- (1)
- Endoscopic ultrasound (EUS) is the most accurate staging method for defining T parameters; its use is therefore recommended when this impacts the treatment approach (endoscopic resection, upfront surgery, perioperative treatment) (Table 2).
- (2)
- The usefulness of EUS in evaluating response after neoadjuvant chemotherapy or chemoradiotherapy appears limited, so it should not be used for restaging outside clinical trials (Table 2).
Sources of Evidence
3.4.2. The Role of FDG PET/CT
Statements
- (1)
- (2)
- FDG PET/CT during treatment or after the end of treatment is useful for identifying patients without any benefit from neoadjuvant treatment; however, this role is marginal outside clinical trials.
Sources of Evidence
3.4.3. Role of Laparoscopic Surgery
Statements
- (1)
- Staging laparoscopy with peritoneal cytology analysis at diagnosis should be considered in all patients at risk for undiagnosed peritoneal disease (cT3/4 and/or cN+), after collegial discussion, especially in those with suspected peritoneal carcinosis and neoadjuvant therapy candidates, to define the correct therapeutic procedure.
- (2)
- Exploratory/staging laparotomy is not recommended.
Sources of Evidence
3.4.4. Role of Nutritional Support during Early Phases of Disease
Statements
- (1)
- Validated screening tests for malnutrition should be used in all patients with gastric cancer before any anti-cancer treatment. For pathologic screening tests, the nutritional team must be involved in setting up an intervention.
- (2)
- Nutritional counseling should be the first intervention in pathologic nutritional screening. This aims to maintain adequate weight and quality of life (QoL) during chemotherapy.
- (3)
- Enteral nutrition support in patients treated with radical-intent gastrectomy should be considered in (neo-)adjuvant settings. After surgery, enteral nutrition can be performed through jejunostomy and continued at home.
Sources of Evidence
3.5. Management of Early Gastric Cancer and Multimodal Approach to Localized Gastric Cancer
3.5.1. Endoscopic Treatment
Statements
- (1)
- Endoscopic treatment is only reliable in early gastric cancers with Lauren intestinal histotype, <2 cm, well-differentiated, non-ulcerated, involving only the mucosa (T1a), and without clinical suspected lymph node involvement. Endoscopic resection can only be considered curative when histologic examination of the sample after endoscopic resection confirms all the above criteria with negative margin status (en bloc resection) in absence of vascular-lymphatic infiltration.
- (2)
- Surgical treatment is the therapeutic option for all early gastric cancers that do not meet the criteria described above, or when evaluation of the specimen does not confirm the radicality of the endoscopic resection.
- (3)
- After endoscopic resection of early gastric cancers, endoscopic follow-up after 3 months, 6 months, 1 year, then annually for 5 years is indicated to exclude the presence of locoregional recurrence.
Sources of Evidence
3.5.2. Principles of Adequate Surgery
Statements
- The extent of gastric resection depends on tumor location and the possibility of achieving an adequate free proximal margin.
- D2 dissection is standard treatment in gastric cancer patients, with the exception of early gastric tumors without nodal involvement.
Sources of Evidence
3.5.3. Sequencing Surgery and Chemotherapy
Statements
- (1)
- In patients with stage II or III gastric carcinoma, perioperative chemotherapy is the standard of care. FLOT (5-fluorouracil [5-FU], oxaliplatin, and docetaxel) is first choice in fit patients.
- (2)
- Patient compliance to preoperative treatment is higher than postoperative treatment.
- (3)
- Preoperative chemotherapy does not increase morbidity and early post-surgery mortality: FLOT is not associated with greater risk for post-surgical complications or mortality than ECF (epirubicin, cisplatin, and 5-FU) or ECX (epirubicin, cisplatin, and capecitabine).
- (4)
- After surgery without any preoperative treatment, an adjuvant therapy with fluoropyrimidine and/or oxaliplatin is recommended.
- (5)
- In the adjuvant setting after upfront surgery for pathologic stage II–III disease, the combination of fluoropyrimidine and oxaliplatin should be considered the preferred option in all patients with adequate recovery after resection.
- (6)
- All patients undergoing surgery for stomach cancer should receive postoperative treatment, regardless of prognostic factors and pathologic response.
Sources of Evidence
- (1)
- There is no difference in OS, but less toxicity, with two preoperative cycles of fluoropyrimidine and cisplatin compared with four preoperative cycles with ECX in patients with esophageal and Siewert I-II GEJ cancers [99].
- (2)
- There is no benefit from adding bevacizumab to perioperative ECX chemotherapy: 3-year overall survival 50.3% with chemotherapy versus 48.1% with addition of bevacizumab [100].
- (3)
- Pathologic regression grade/response (<pT1: 15% vs. 25%) and overall survival (50 months vs. 35 months; HR = 0.77; 95% CI, 0.63-0.94; p = 0.012) benefit from perioperative FLOT compared with the ECF/ECX combinations. OS at 2–3 and 5 years was 59%, 48%, and 36% with ECF/ECX compared with 68%, 57%, and 45% with FLOT [101]. Similar rates of post-surgical complications with FLOT and ECF/ECX were reported (51% vs. 50%). Median duration of hospitalization was also similar in the two arms (15 vs. 16 days), as were reoperation rates (10% vs. 11%), and deaths within 30 days (2% vs. 3%) and within 90 days (5% vs. 8%).
Statement
Sources of Evidence
Statement
Sources of Evidence
Statement
- (1)
- Perioperative chemotherapy can be considered first choice for patients with stage IB gastric cancer after multidisciplinary discussion about the site of the primary tumor, the characteristics of the patient (age, performance status [PS], comorbidities), and the biology of the tumor (histotype, MSI).
Sources of Evidence
Statement
Sources of Evidence
Statements
- (1)
- In patients with stage II/III gastric cancer undergoing suboptimal surgical (<D2) or with R1, adjuvant chemoradiotherapy should be considered as the first therapeutic option.
- (2)
- In patients with stage II/III gastric cancer undergoing radical surgery, adjuvant chemoradiotherapy can be considered after adjuvant chemotherapy in pN+ patients, after multidisciplinary discussion.
Sources of Evidence
3.5.4. Treatment of Siewert II Adenocarcinoma
Statement
- (1)
- In patients with Siewert II adenocarcinoma, while acknowledging the fundamental role of a multidisciplinary discussion for every single situation, perioperative chemotherapy with FLOT is preferable, reserving preoperative chemoradiotherapy for patients at high risk for R1 resection and local recurrence.
Sources of Evidence
3.6. Treatment of Elderly Patients with Locally Advanced Resectable Disease
3.6.1. (Neo-)Adjuvant Therapy
Statements
- MGA allows the identification of frail patients who are at higher risk for complications after gastrectomy.
- The role of MGA in determining medical treatment is less established in resectable disease compared with the palliative setting. However, MGA might also help the MDT in personalizing treatment approaches when the aim of treatment is curative.
- Age does not impact perioperative chemotherapy benefit over surgery alone or the benefit of FLOT over ECF/ECX.
- High-grade toxicities with FLOT are more common in the elderly. Accurate patient selection is therefore needed with taxane-based triplet regimens.
Sources of Evidence
3.6.2. Treatment of Locally Advanced Unresectable and Metastatic Disease
First-Line Therapy
Statements
- (1)
- Patient PS, comorbidities, and disease burden are all factors that should be considered in the choice of first-line therapy.
- (2)
- Among molecular parameters investigated, only HER2 status has been validated as a predictive biomarker for choice of first-line therapy.
- (3)
- Platinum plus fluoropyrimidine doublet chemotherapy regimens represent standard of care in this setting.
- (4)
- Triplet chemotherapy, mainly FLOT, is preferable for selected fit patients (i.e., with Eastern Cooperative Oncology Group [ECOG] PS 0–1, adequate organ function) with either locally advanced unresectable disease or high tumor burden.
- (5)
- While deciding optimal first-line chemotherapy in individual patients, a cautious assessment of residual toxicity from (neo-)adjuvant therapies as well as time interval between treatment interruption and evidence of recurrence is recommended.
- (6)
- For fit patients experiencing progression soon after (i.e., ≤6 months of completion) or during adjuvant treatment with platinum plus fluoropyrimidine, the combination of paclitaxel plus ramucirumab is the preferred choice.
- (7)
- For fit patients experiencing progression soon after (i.e., ≤6 months of completion) or during adjuvant treatment with docetaxel, FOLFIRI or ramucirumab should be considered. If recurrence occurs >6 months after completion of adjuvant therapy, paclitaxel plus ramucirumab should be considered.
Sources of Evidence
Second-Line Therapy
Statements
- (1)
- Considering the aggressiveness of the disease, often associated with rapid deterioration, many patients do not receive second-line therapy (in Western countries, ~30–40% of patients receive salvage therapies).
- (2)
- To increase the number of patients who are candidates for second-line therapies, accurate patient monitoring during first-line therapy is mandatory, to capture early signs of clinical progression which may anticipate radiographic progression.
- (3)
- Imaging for disease assessment should ideally be performed every 2 months in patients with metastatic disease and should be accompanied by detailed and close monitoring of clinical conditions.
- (4)
- All patients with ECOG PS 0 or 1 should be offered second-line treatment after progression to first-line therapy.
- (5)
- ECOG PS ≥ 2 patients are candidates for BSC alone.
- (6)
- For patients with gastric or GEJ cancer that has progressed after first-line therapy not including a taxane, the combination of paclitaxel and ramucirumab is the preferred choice.
- (7)
- For patients with gastric or GEJ cancer that has progressed after first-line therapy with a taxane, the combination of paclitaxel and ramucirumab should be considered in patients with previous response to first-line therapy. In all other patients, including those with contraindications to this combination, alternative options can be considered, such as single-agent ramucirumab or irinotecan.
Sources of Evidence
3.6.3. Role of Maintenance Therapy After First- and Second-Line Treatment
Statements
- Optimal treatment duration in first or second line cannot be informed by literature evidence and should be tailored to individual patient preference and tolerance.
- The choice of shifting to maintenance treatment should be individualized after discussion with the patient about the risk-to-benefit ratio of this approach.
- After 6 months of first-line combination treatment without evidence of progression, patients with HER2-positive disease can be offered maintenance with trastuzumab, either as single-agent or combined with fluoropyrimidine.
- Maintenance with ramucirumab monotherapy can be considered in patients treated with second-line paclitaxel plus ramucirumab with unacceptable toxicities related to paclitaxel.
Sources of Evidence
3.6.4. Role of Third-Line Therapy
Statements
- Fewer than 20% of Western gastric cancer patients are offered third-line therapies in clinical practice.
- Patients with adequate general health (ECOG PS 0–1) who experience progression on second-line therapy may be considered for third-line therapies. Among cytotoxic agents, TAS102 (if available) is a preferred option; irinotecan (if not used in previous lines) may be considered if TAS102 is not available.
Sources of Evidence
3.6.5. Role of Immunotherapy in Advanced Disease
Statements
- For patients with MSI-high disease, treatment with immune checkpoint inhibitors (ICIs) should be considered if not administered in earlier lines.
- Based on already published or presented Phase 3 studies investigating ICIs either alone or in combination with chemotherapy, ICIs should not be offered in routine practice to unselected metastatic gastric cancer patients outside clinical trials.
- Based on available efficacy data of ICIs in MSI-high gastric cancer patients, treatment with ICIs should always be considered in this subgroup within clinical trials or as off-label use.
- No pharmacoeconomic analyses have been published on the use of ICIs in advanced disease.
Sources of Evidence
3.6.6. Role of HIPEC and PIPAC in Advanced Disease
Statements
- (1)
- Results for CRS plus HIPEC in gastric cancer with peritoneal involvement are limited and controversial. While confirmation in randomized trials is ongoing, this approach should be offered only within a clinical trial.
- (2)
- There is currently insufficient evidence to recommend the use of PIPAC outside a clinical trial. The use of this technique may be of particular interest in treating uncontrolled malignant ascites.
Sources of Evidence
3.6.7. Nutritional Support During Treatment of Advanced Disease
Statement
- (1)
- HPN is a valid therapeutic option for malnourished patients with advanced gastric cancer. To reduce the risks related to HPN, this approach should be planned and managed by dedicated personnel according to validated protocols.
Sources of Evidence
Statements
- (1)
- Nutritional status assessment must be performed before treatment initiation in all patients who are candidates for systemic therapies.
- (2)
- Nutritional support need and programming of such support should be established by a dedicated nutrition expert.
Sources of Evidence
3.6.8. Definition of a Continuum of Care in Advanced Gastric Cancer
Statement
- (1)
- Multidisciplinary management, rather than treatment centralization in high-volume centers, represents the most effective strategy to optimize the continuum of care of medical therapies in all treatment phases.
Sources of Evidence
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Van Cutsem, E.; Sagaert, X.; Topal, B.; Haustermans, K.; Prenen, H. Gastric cancer. Lancet 2016, 388, 2654–2664. [Google Scholar] [CrossRef]
- Boniface, M.M.; Wani, S.B.; Schefter, T.E.; Koo, P.J.; Meguid, C.; Leong, S.; Kaplan, J.B.; Wingrove, L.J.; McCarter, M.D. Multidisciplinary management for esophageal and gastric cancer. Cancer Manag. Res. 2016, 8, 39–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misleh, J.G.; Santoro, P.; Strasser, J.F.; Bennett, J.J. Multidisciplinary management of gastric cancer. Surg. Oncol. Clin. N. Am. 2013, 22, 247–264. [Google Scholar] [CrossRef] [PubMed]
- Basta, Y.L.; Baur, O.L.; van Dieren, S.; Klinkenbijl, J.H.; Fockens, P.; Tytgat, K.M. Is there a Benefit of Multidisciplinary Cancer Team Meetings for Patients with Gastrointestinal Malignancies? Ann. Surg. Oncol. 2016, 23, 2430–2437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brauer, D.G.; Strand, M.S.; Sanford, D.E.; Kushnir, V.M.; Lim, K.H.; Mullady, D.K.; Tan, B.R., Jr.; Wang-Gillam, A.; Morton, A.E.; Ruzinova, M.B.; et al. Utility of a multidisciplinary tumor board in the management of pancreatic and upper gastrointestinal diseases: An observational study. HPB 2017, 19, 133–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Saghir, N.S.; Charara, R.N.; Kreidieh, F.Y.; Eaton, V.; Litvin, K.; Farhat, R.A.; Khoury, K.E.; Breidy, J.; Tamim, H.; Eid, T.A. Global Practice and Efficiency of Multidisciplinary Tumor Boards: Results of an American Society of Clinical Oncology International Survey. J. Glob. Oncol. 2015, 1, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Pillay, B.; Wootten, A.C.; Crowe, H.; Corcoran, N.; Tran, B.; Bowden, P.; Crowe, J.; Costello, A.J. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat. Rev. 2016, 42, 56–72. [Google Scholar] [CrossRef] [PubMed]
- Kamarajah, S.K.; Bundred, J.; Tan, B.H.L. Body composition assessment and sarcopenia in patients with gastric cancer: A systematic review and meta-analysis. Gastric. Cancer 2019, 22, 10–22. [Google Scholar] [CrossRef] [Green Version]
- Kuwada, K.; Kuroda, S.; Kikuchi, S.; Yoshida, R.; Nishizaki, M.; Kagawa, S.; Fujiwara, T. Clinical Impact of Sarcopenia on Gastric Cancer. Anticancer Res. 2019, 39, 2241–2249. [Google Scholar] [CrossRef] [Green Version]
- Antoun, S.; Borget, I.; Lanoy, E. Impact of sarcopenia on the prognosis and treatment toxicities in patients diagnosed with cancer. Curr. Opin. Support. Palliat. Care 2013, 7, 383–389. [Google Scholar] [CrossRef]
- Ongaro, E.; Buoro, V.; Cinausero, M.; Caccialanza, R.; Turri, A.; Fanotto, V.; Basile, D.; Vitale, M.G.; Ermacora, P.; Cardellino, G.G.; et al. Sarcopenia in gastric cancer: When the loss costs too much. Gastric. Cancer 2017, 20, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Adamu, M.A.; Weck, M.N.; Gao, L.; Brenner, H. Incidence of chronic atrophic gastritis: Systematic review and meta-analysis of follow-up studies. Eur. J. Epidemiol. 2010, 25, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Pimentel-Nunes, P.; Libanio, D.; Marcos-Pinto, R.; Areia, M.; Leja, M.; Esposito, G.; Garrido, M.; Kikuste, I.; Megraud, F.; Matysiak-Budnik, T.; et al. Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update 2019. Endoscopy 2019, 51, 365–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yue, H.; Shan, L.; Bin, L. The significance of OLGA and OLGIM staging systems in the risk assessment of gastric cancer: A systematic review and meta-analysis. Gastric. Cancer 2018, 21, 579–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moayyedi, P.; Lacy, B.E.; Andrews, C.N.; Enns, R.A.; Howden, C.W.; Vakil, N. ACG and CAG Clinical Guideline: Management of Dyspepsia. Am. J. Gastroenterol. 2017, 112, 988–1013. [Google Scholar] [CrossRef] [PubMed]
- Weck, M.N.; Brenner, H. Association of Helicobacter pylori infection with chronic atrophic gastritis: Meta-analyses according to type of disease definition. Int. J. Cancer 2008, 123, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Li, M.; Chen, S.; Hu, J.; Guo, Q.; Liu, R.; Zheng, H.; Jin, Z.; Yuan, Y.; Xi, Y.; et al. Endoscopic Screening in Asian Countries Is Associated With Reduced Gastric Cancer Mortality: A Meta-analysis and Systematic Review. Gastroenterology 2018, 155, 347–354.e9. [Google Scholar] [CrossRef] [Green Version]
- Zhao, B.; Zhao, J.; Cheng, W.F.; Shi, W.J.; Liu, W.; Pan, X.L.; Zhang, G.X. Efficacy of Helicobacter pylori eradication therapy on functional dyspepsia: A meta-analysis of randomized controlled studies with 12-month follow-up. J. Clin. Gastroenterol. 2014, 48, 241–247. [Google Scholar] [CrossRef]
- Hwang, Y.J.; Kim, N.; Lee, H.S.; Lee, J.B.; Choi, Y.J.; Yoon, H.; Shin, C.M.; Park, Y.S.; Lee, D.H. Reversibility of atrophic gastritis and intestinal metaplasia after Helicobacter pylori eradication—A prospective study for up to 10 years. Aliment. Pharmacol. Ther. 2018, 47, 380–390. [Google Scholar] [CrossRef] [Green Version]
- Choi, K.S.; Jun, J.K.; Suh, M.; Park, B.; Noh, D.K.; Song, S.H.; Jung, K.W.; Lee, H.Y.; Choi, I.J.; Park, E.C. Effect of endoscopy screening on stage at gastric cancer diagnosis: Results of the National Cancer Screening Programme in Korea. Br. J. Cancer 2015, 112, 608–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamashima, C.; Systematic Review, G.; Development Group for Gastric Cancer Screening Guidelines. Update version of the Japanese Guidelines for Gastric Cancer Screening. Jpn. J. Clin. Oncol. 2018, 48, 673–683. [Google Scholar] [CrossRef] [Green Version]
- Saumoy, M.; Schneider, Y.; Shen, N.; Kahaleh, M.; Sharaiha, R.Z.; Shah, S.C. Cost Effectiveness of Gastric Cancer Screening According to Race and Ethnicity. Gastroenterology 2018, 155, 648–660. [Google Scholar] [CrossRef] [Green Version]
- Rugge, M.; Capelle, L.G.; Fassan, M. Individual risk stratification of gastric cancer: Evolving concepts and their impact on clinical practice. Best Pract. Res. Clin. Gastroenterol. 2014, 28, 1043–1053. [Google Scholar] [CrossRef]
- Spence, A.D.; Cardwell, C.R.; McMenamin, U.C.; Hicks, B.M.; Johnston, B.T.; Murray, L.J.; Coleman, H.G. Adenocarcinoma risk in gastric atrophy and intestinal metaplasia: A systematic review. BMC Gastroenterol. 2017, 17, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pimenta-Melo, A.R.; Monteiro-Soares, M.; Libanio, D.; Dinis-Ribeiro, M. Missing rate for gastric cancer during upper gastrointestinal endoscopy: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2016, 28, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Vangala, D.B.; Cauchin, E.; Balmana, J.; Wyrwicz, L.; van Cutsem, E.; Guller, U.; Castells, A.; Carneiro, F.; Hammel, P.; Ducreux, M.; et al. Screening and surveillance in hereditary gastrointestinal cancers: Recommendations from the European Society of Digestive Oncology (ESDO) expert discussion at the 20th European Society for Medical Oncology (ESMO)/World Congress on Gastrointestinal Cancer, Barcelona, June 2018. Eur. J. Cancer 2018, 104, 91–103. [Google Scholar] [CrossRef]
- Fitzgerald, R.C.; Hardwick, R.; Huntsman, D.; Carneiro, F.; Guilford, P.; Blair, V.; Chung, D.C.; Norton, J.; Ragunath, K.; Van Krieken, J.H.; et al. Hereditary diffuse gastric cancer: Updated consensus guidelines for clinical management and directions for future research. J. Med. Genet. 2010, 47, 436–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansford, S.; Kaurah, P.; Li-Chang, H.; Woo, M.; Senz, J.; Pinheiro, H.; Schrader, K.A.; Schaeffer, D.F.; Shumansky, K.; Zogopoulos, G.; et al. Hereditary Diffuse Gastric Cancer Syndrome: CDH1 Mutations and Beyond. JAMA Oncol. 2015, 1, 23–32. [Google Scholar] [CrossRef] [Green Version]
- van der Post, R.S.; Vogelaar, I.P.; Carneiro, F.; Guilford, P.; Huntsman, D.; Hoogerbrugge, N.; Caldas, C.; Schreiber, K.E.; Hardwick, R.H.; Ausems, M.G.; et al. Hereditary diffuse gastric cancer: Updated clinical guidelines with an emphasis on germline CDH1 mutation carriers. J. Med. Genet. 2015, 52, 361–374. [Google Scholar] [CrossRef] [Green Version]
- Worthley, D.L.; Phillips, K.D.; Wayte, N.; Schrader, K.A.; Healey, S.; Kaurah, P.; Shulkes, A.; Grimpen, F.; Clouston, A.; Moore, D.; et al. Gastric adenocarcinoma and proximal polyposis of the stomach (GAPPS): A new autosomal dominant syndrome. Gut 2012, 61, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.; Pinheiro, H.; Figueiredo, J.; Seruca, R.; Carneiro, F. Familial gastric cancer: Genetic susceptibility, pathology, and implications for management. Lancet Oncol. 2015, 16, e60–e70. [Google Scholar] [CrossRef]
- He, C.; Bian, X.Y.; Ni, X.Z.; Shen, D.P.; Shen, Y.Y.; Liu, H.; Shen, Z.Y.; Liu, Q. Correlation of human epidermal growth factor receptor 2 expression with clinicopathological characteristics and prognosis in gastric cancer. World J. Gastroenterol. 2013, 19, 2171–2178. [Google Scholar] [CrossRef] [PubMed]
- Kwack, W.G.; Ho, W.J.; Kim, J.H.; Lee, J.H.; Kim, E.J.; Kang, H.W.; Lee, J.K. Understanding the diagnostic yield of current endoscopic biopsy for gastric neoplasm: A prospective single-center analysis based on tumor characteristics stratified by biopsy number and site. Medicine 2016, 95, e4196. [Google Scholar] [CrossRef]
- Petrelli, F.; Berenato, R.; Turati, L.; Mennitto, A.; Steccanella, F.; Caporale, M.; Dallera, P.; de Braud, F.; Pezzica, E.; Di Bartolomeo, M.; et al. Prognostic value of diffuse versus intestinal histotype in patients with gastric cancer: A systematic review and meta-analysis. J. Gastrointest. Oncol. 2017, 8, 148–163. [Google Scholar] [CrossRef] [Green Version]
- Smyth, E.C.; Fassan, M.; Cunningham, D.; Allum, W.H.; Okines, A.F.; Lampis, A.; Hahne, J.C.; Rugge, M.; Peckitt, C.; Nankivell, M.; et al. Effect of Pathologic Tumor Response and Nodal Status on Survival in the Medical Research Council Adjuvant Gastric Infusional Chemotherapy Trial. J. Clin. Oncol. 2016, 34, 2721–2727. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Werner, D.; Pauligk, C.; Steinmetz, K.; Kelsen, D.P.; Jager, E.; Altmannsberger, H.M.; Robinson, E.; Tafe, L.J.; Tang, L.H.; et al. Prognosis of metastatic gastric and gastroesophageal junction cancer by HER2 status: A European and USA International collaborative analysis. Ann. Oncol. 2012, 23, 2656–2662. [Google Scholar] [CrossRef]
- Arnold, A.; Daum, S.; von Winterfeld, M.; Berg, E.; Hummel, M.; Horst, D.; Rau, B.; Stein, U.; Treese, C. Analysis of NTRK expression in gastric and esophageal adenocarcinoma (AGE) with pan-TRK immunohistochemistry. Pathol. Res. Pract. 2019, 215, 152662. [Google Scholar] [CrossRef]
- Okamura, R.; Boichard, A.; Kato, S.; Sicklick, J.K.; Bazhenova, L.; Kurzrock, R. Analysis of NTRK Alterations in Pan-Cancer Adult and Pediatric Malignancies: Implications for NTRK-Targeted Therapeutics. JCO Precis Oncol. 2018, 2018. [Google Scholar] [CrossRef]
- Patel, M.R.S.; Demetri, G.; Doebele, R.C.; Chae, Y.K.; Conkling, P.; Garrido-Laguna, I.; Longo, F.; Rolfo, C.; Sigal, D. Efficacy and safety of entrectinib in NTRK fusion-positive gastrointestinal cancers: Updated integrated analysis of three clinical trials (STARTRK-2, STARTRK-1 and ALKA-372-001). In Proceedings of the ESMO World Congress on Gastrointestinal Cancer 2020 Virtual Meeting, 1–4 July 2020; Available online: https://www.esmo.org/meetings/past-meetings/esmo-world-gi-2020-virtual (accessed on 14 March 2021).
- Solomon, J.P.; Linkov, I.; Rosado, A.; Mullaney, K.; Rosen, E.Y.; Frosina, D.; Jungbluth, A.A.; Zehir, A.; Benayed, R.; Drilon, A.; et al. NTRK fusion detection across multiple assays and 33,997 cases: Diagnostic implications and pitfalls. Mod. Pathol. 2020, 33, 38–46. [Google Scholar] [CrossRef]
- Zehir, A.; Benayed, R.; Shah, R.H.; Syed, A.; Middha, S.; Kim, H.R.; Srinivasan, P.; Gao, J.; Chakravarty, D.; Devlin, S.M.; et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat. Med. 2017, 23, 703–713. [Google Scholar] [CrossRef]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Bartley, A.N.; Washington, M.K.; Colasacco, C.; Ventura, C.B.; Ismaila, N.; Benson, A.B., 3rd; Carrato, A.; Gulley, M.L.; Jain, D.; Kakar, S.; et al. HER2 Testing and Clinical Decision Making in Gastroesophageal Adenocarcinoma: Guideline From the College of American Pathologists, American Society for Clinical Pathology, and the American Society of Clinical Oncology. J. Clin. Oncol. 2017, 35, 446–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tominaga, N.; Gotoda, T.; Hara, M.; Hale, M.D.; Tsuchiya, T.; Matsubayashi, J.; Kono, S.; Kusano, C.; Itoi, T.; Fujimoto, K.; et al. Five biopsy specimens from the proximal part of the tumor reliably determine HER2 protein expression status in gastric cancer. Gastric. Cancer 2016, 19, 553–560. [Google Scholar] [CrossRef] [Green Version]
- Wong, N.; Amary, F.; Butler, R.; Byers, R.; Gonzalez, D.; Haynes, H.R.; Ilyas, M.; Salto-Tellez, M.; Taniere, P. HER2 testing of gastro-oesophageal adenocarcinoma: A commentary and guidance document from the Association of Clinical Pathologists Molecular Pathology and Diagnostics Committee. J. Clin. Pathol. 2018, 71, 388–394. [Google Scholar] [CrossRef] [Green Version]
- Lordick, F.; Janjigian, Y.Y. Clinical impact of tumour biology in the management of gastroesophageal cancer. Nat. Rev. Clin. Oncol. 2016, 13, 348–360. [Google Scholar] [CrossRef]
- Gambardella, V.; Gimeno-Valiente, F.; Tarazona, N.; Martinez-Ciarpaglini, C.; Roda, D.; Fleitas, T.; Tolosa, P.; Cejalvo, J.M.; Huerta, M.; Rosello, S.; et al. NRF2 through RPS6 Activation Is Related to Anti-HER2 Drug Resistance in HER2-Amplified Gastric Cancer. Clin. Cancer Res. 2019, 25, 1639–1649. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Fuca, G.; Morano, F.; Gloghini, A.; Corso, S.; Aprile, G.; Perrone, F.; De Vita, F.; Tamborini, E.; Tomasello, G.; et al. Biomarkers of Primary Resistance to Trastuzumab in HER2-Positive Metastatic Gastric Cancer Patients: The AMNESIA Case-Control Study. Clin. Cancer Res. 2018, 24, 1082–1089. [Google Scholar] [CrossRef] [Green Version]
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [Green Version]
- Ratti, M.; Lampis, A.; Hahne, J.C.; Passalacqua, R.; Valeri, N. Microsatellite instability in gastric cancer: Molecular bases, clinical perspectives, and new treatment approaches. Cell. Mol. Life Sci. 2018, 75, 4151–4162. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, C.S.; Doi, T.; Jang, R.W.; Muro, K.; Satoh, T.; Machado, M.; Sun, W.; Jalal, S.I.; Shah, M.A.; Metges, J.P.; et al. Safety and Efficacy of Pembrolizumab Monotherapy in Patients With Previously Treated Advanced Gastric and Gastroesophageal Junction Cancer: Phase 2 Clinical KEYNOTE-059 Trial. JAMA Oncol. 2018, 4, e180013. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, J.; Van Cutsem, E.; Bang, Y.; Fuchs, C.; Wyrwicz, L.; Lee, K.; Kudaba, I.; Garrido, M.; Chung, H.; Castro Salguero, H.; et al. Pembrolizumab with or without chemotherapy versus chemotherapy for first-line treatment of advanced gastric or gastroesophageal junction (G/GEJ) adenocarcinoma: The Phase 3 KEYNOTE-062 Study. Ann. Oncol. 2019, 30 (Suppl. 4), iv152–iv153. [Google Scholar] [CrossRef]
- Kulangara, K.; Zhang, N.; Corigliano, E.; Guerrero, L.; Waldroup, S.; Jaiswal, D.; Ms, M.J.; Shah, S.; Hanks, D.; Wang, J.; et al. Clinical Utility of the Combined Positive Score for Programmed Death Ligand-1 Expression and the Approval of Pembrolizumab for Treatment of Gastric Cancer. Arch. Pathol. Lab. Med. 2019, 143, 330–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mocellin, S.; Pasquali, S. Diagnostic accuracy of endoscopic ultrasonography (EUS) for the preoperative locoregional staging of primary gastric cancer. Cochrane Database Syst. Rev. 2015, CD009944. [Google Scholar] [CrossRef]
- Bohle, W.; Kasper, M.; Zoller, W.G. Different accuracy of endosonographic tumor staging after neoadjuvant chemotherapy and chemoradiotherapy in esophageal cancer. Surg. Endosc. 2016, 30, 2922–2928. [Google Scholar] [CrossRef]
- Misra, S.; Choi, M.; Livingstone, A.S.; Franceschi, D. The role of endoscopic ultrasound in assessing tumor response and staging after neoadjuvant chemotherapy for esophageal cancer. Surg. Endosc. 2012, 26, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Findlay, J.M.; Antonowicz, S.; Segaran, A.; El Kafsi, J.; Zhang, A.; Bradley, K.M.; Gillies, R.S.; Maynard, N.D.; Middleton, M.R. Routinely staging gastric cancer with (18)F-FDG PET-CT detects additional metastases and predicts early recurrence and death after surgery. Eur. Radiol. 2019, 29, 2490–2498. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, K.; Eshmuminov, D.; Bauerfeind, P.; Gubler, C.; Veit-Haibach, P.; Weber, A.; Abdul-Rahman, H.; Fischer, M.; Reiner, C.; Schneider, P.M. (18)FDG-PET-CT improves specificity of preoperative lymph-node staging in patients with intestinal but not diffuse-type esophagogastric adenocarcinoma. Eur. J. Surg. Oncol. 2017, 43, 196–202. [Google Scholar] [CrossRef] [Green Version]
- Chon, H.J.; Kim, C.; Cho, A.; Kim, Y.M.; Jang, S.J.; Kim, B.O.; Park, C.H.; Hyung, W.J.; Ahn, J.B.; Noh, S.H.; et al. The clinical implications of FDG-PET/CT differ according to histology in advanced gastric cancer. Gastric. Cancer 2019, 22, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Kawanaka, Y.; Kitajima, K.; Fukushima, K.; Mouri, M.; Doi, H.; Oshima, T.; Niwa, H.; Kaibe, N.; Sasako, M.; Tomita, T.; et al. Added value of pretreatment (18)F-FDG PET/CT for staging of advanced gastric cancer: Comparison with contrast-enhanced MDCT. Eur. J. Radiol. 2016, 85, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, J.M.; Beylergil, V.; Goldman, D.A.; van Beek, E.; Gonen, M.; Tang, L.; Downey, R.; Rizk, N.; Shah, M.; Strong, V.; et al. Post-Treatment/Pre-operative PET Response Is Not an Independent Predictor of Outcomes for Patients With Gastric and GEJ Adenocarcinoma. Ann. Surg. 2018, 267, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Schneider, P.M.; Eshmuminov, D.; Rordorf, T.; Vetter, D.; Veit-Haibach, P.; Weber, A.; Bauerfeind, P.; Samaras, P.; Lehmann, K. (18)FDG-PET-CT identifies histopathological non-responders after neoadjuvant chemotherapy in locally advanced gastric and cardia cancer: Cohort study. BMC Cancer 2018, 18, 548. [Google Scholar] [CrossRef] [PubMed]
- zum Buschenfelde, C.M.; Herrmann, K.; Schuster, T.; Geinitz, H.; Langer, R.; Becker, K.; Ott, K.; Ebert, M.; Zimmermann, F.; Friess, H.; et al. (18)F-FDG PET-guided salvage neoadjuvant radiochemotherapy of adenocarcinoma of the esophagogastric junction: The MUNICON II trial. J. Nucl. Med. 2011, 52, 1189–1196. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Chen, J.Q.; Liu, J.L.; Tian, L. Issues on peritoneal metastasis of gastric cancer: An update. World J. Surg. Oncol. 2019, 17, 215. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Li, Z.; Zhang, L.; Liu, Q.; Wang, Z.; Zhang, Z.; Xiao, G.; Fu, W.; Wang, X.; Ye, Y.; et al. Staging laparoscopy for locally advanced gastric cancer in Chinese patients: A multicenter prospective registry study. BMC Cancer 2018, 18, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coburn, N.; Cosby, R.; Klein, L.; Knight, G.; Malthaner, R.; Mamazza, J.; Mercer, C.D.; Ringash, J. Staging and surgical approaches in gastric cancer: A systematic review. Cancer Treat. Rev. 2018, 63, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Ramos, R.F.; Scalon, F.M.; Scalon, M.M.; Dias, D.I. Staging laparoscopy in gastric cancer to detect peritoneal metastases: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2016, 42, 1315–1321. [Google Scholar] [CrossRef]
- Jamel, S.; Markar, S.R.; Malietzis, G.; Acharya, A.; Athanasiou, T.; Hanna, G.B. Prognostic significance of peritoneal lavage cytology in staging gastric cancer: Systematic review and meta-analysis. Gastric. Cancer 2018, 21, 10–18. [Google Scholar] [CrossRef]
- Cardona, K.; Zhou, Q.; Gonen, M.; Shah, M.A.; Strong, V.E.; Brennan, M.F.; Coit, D.G. Role of repeat staging laparoscopy in locoregionally advanced gastric or gastroesophageal cancer after neoadjuvant therapy. Ann. Surg. Oncol. 2013, 20, 548–554. [Google Scholar] [CrossRef]
- Jensen, G.L.; Cederholm, T.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; de Baptista, G.A.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM Criteria for the Diagnosis of Malnutrition: A Consensus Report From the Global Clinical Nutrition Community. JPEN J. Parenter Enteral. Nutr. 2019, 43, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Guo, W.; Ou, G.; Li, X.; Huang, J.; Liu, J.; Wei, H. Screening of the nutritional risk of patients with gastric carcinoma before operation by NRS 2002 and its relationship with postoperative results. J. Gastroenterol. Hepatol. 2010, 25, 800–803. [Google Scholar] [CrossRef]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. ESPEN guidelines for nutrition screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Baldwin, C.; Spiro, A.; Ahern, R.; Emery, P.W. Oral nutritional interventions in malnourished patients with cancer: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2012, 104, 371–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravasco, P. Nutritional approaches in cancer: Relevance of individualized counseling and supplementation. Nutrition 2015, 31, 603–604. [Google Scholar] [CrossRef]
- Caccialanza, R.; Pedrazzoli, P.; Cereda, E.; Gavazzi, C.; Pinto, C.; Paccagnella, A.; Beretta, G.D.; Nardi, M.; Laviano, A.; Zagonel, V. Nutritional Support in Cancer Patients: A Position Paper from the Italian Society of Medical Oncology (AIOM) and the Italian Society of Artificial Nutrition and Metabolism (SINPE). J. Cancer 2016, 7, 131–135. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hubner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavazzi, C.; Colatruglio, S.; Valoriani, F.; Mazzaferro, V.; Sabbatini, A.; Biffi, R.; Mariani, L.; Miceli, R. Impact of home enteral nutrition in malnourished patients with upper gastrointestinal cancer: A multicentre randomised clinical trial. Eur. J. Cancer 2016, 64, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Abdelfatah, M.M.; Barakat, M.; Ahmad, D.; Ibrahim, M.; Ahmed, Y.; Kurdi, Y.; Grimm, I.S.; Othman, M.O. Long-term outcomes of endoscopic submucosal dissection versus surgery in early gastric cancer: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2019, 31, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Kondo, A.; de Moura, E.G.; Bernardo, W.M.; Yagi, O.K.; de Moura, D.T.; de Moura, E.T.; Bravo, J.G.; Yamazaki, K.; Sakai, P. Endoscopy vs surgery in the treatment of early gastric cancer: Systematic review. World J. Gastroenterol. 2015, 21, 13177–13187. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Ding, L.; Qiu, X.; Meng, F. Updated evaluation of endoscopic submucosal dissection versus surgery for early gastric cancer: A systematic review and meta-analysis. Int. J. Surg. 2020, 73, 28–41. [Google Scholar] [CrossRef]
- Bourke, M.J.; Neuhaus, H.; Bergman, J.J. Endoscopic Submucosal Dissection: Indications and Application in Western Endoscopy Practice. Gastroenterology 2018, 154, 1887–1900. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.G.; Park, C.M.; Lee, N.R.; Kim, J.; Lyu, D.H.; Park, S.H.; Choi, I.J.; Lee, W.S.; Park, S.J.; Kim, J.J.; et al. Long-Term Clinical Outcomes of Endoscopic Submucosal Dissection in Patients with Early Gastric Cancer: A Prospective Multicenter Cohort Study. Gut Liver 2018, 12, 402–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ning, F.L.; Zhang, C.D.; Wang, P.; Shao, S.; Dai, D.Q. Endoscopic resection versus radical gastrectomy for early gastric cancer in Asia: A meta-analysis. Int. J. Surg. 2017, 48, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, S.G.; Chung, H.; Lim, J.H.; Choi, J.M.; Park, J.Y.; Yang, H.J.; Han, S.J.; Oh, S.; Kim, M.S.; et al. Clinical efficacy of endoscopic ultrasonography for decision of treatment strategy of gastric cancer. Surg. Endosc. 2018, 32, 3789–3797. [Google Scholar] [CrossRef] [PubMed]
- Abdelfatah, M.M.; Barakat, M.; Othman, M.O.; Grimm, I.S.; Uedo, N. The incidence of lymph node metastasis in submucosal early gastric cancer according to the expanded criteria: A systematic review. Surg. Endosc. 2019, 33, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Cai, A.; Xi, H.; Chen, L.; Peng, Z.; Li, P.; Liu, N.; Cui, J.; Li, H. Predictive Factors for Lymph Node Metastasis in Undifferentiated Early Gastric Cancer: A Systematic Review and Meta-analysis. J. Gastrointest. Surg. 2017, 21, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Yin, Z.; Wang, S.; Wang, J.; Bai, B.; Qiu, Z.; Zhao, Q. Meta-analysis: The diagnostic efficacy of chromoendoscopy for early gastric cancer and premalignant gastric lesions. J. Gastroenterol. Hepatol. 2016, 31, 1539–1545. [Google Scholar] [CrossRef] [PubMed]
- Nam, H.S.; Choi, C.W.; Kim, S.J.; Kang, D.H.; Kim, H.W.; Park, S.B.; Ryu, D.G. Endoscopic predictive factors associated with local recurrence after gastric endoscopic submucosal dissection. Scand. J. Gastroenterol. 2018, 53, 1000–1007. [Google Scholar] [CrossRef] [PubMed]
- Japanese Gastric Cancer, A. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric. Cancer 2020. [Google Scholar] [CrossRef] [Green Version]
- Cho, B.C.; Jeung, H.C.; Choi, H.J.; Rha, S.Y.; Hyung, W.J.; Cheong, J.H.; Noh, S.H.; Chung, H.C. Prognostic impact of resection margin involvement after extended (D2/D3) gastrectomy for advanced gastric cancer: A 15-year experience at a single institute. J. Surg. Oncol. 2007, 95, 461–468. [Google Scholar] [CrossRef]
- Sano, T.; Sasako, M.; Mizusawa, J.; Yamamoto, S.; Katai, H.; Yoshikawa, T.; Nashimoto, A.; Ito, S.; Kaji, M.; Imamura, H.; et al. Randomized controlled trial to evaluate splenectomy in total gastrectomy for proximal gastric carcinoma. Ann. Surg. 2017, 265, 277–283. [Google Scholar] [CrossRef]
- Kim, H.H.; Han, S.U.; Kim, M.C.; Kim, W.; Lee, H.J.; Ryu, S.W.; Cho, G.S.; Kim, C.Y.; Yang, H.K.; Park, D.J.; et al. Effect of laparoscopic distal gastrectomy vs open distal gastrectomy on long-term survival among patients with stage I gastric cancer: The KLASS-01 randomized clinical trial. JAMA Oncol. 2019, 5, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Mocellin, S.; Nitti, D. Lymphadenectomy extent and survival of patients with gastric carcinoma: A systematic review and meta-analysis of time-to-event data from randomized trials. Cancer Treat. Rev. 2015, 41, 448–454. [Google Scholar] [CrossRef]
- Raziee, H.R.; Cardoso, R.; Seevaratnam, R.; Mahar, A.; Helyer, L.; Law, C.; Coburn, N. Systematic review of the predictors of positive margins in gastric cancer surgery and the effect on survival. Gastric. Cancer 2012, 15 (Suppl. 1), S116–S124. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Ychou, M.; Boige, V.; Pignon, J.P.; Conroy, T.; Bouche, O.; Lebreton, G.; Ducourtieux, M.; Bedenne, L.; Fabre, J.M.; Saint-Aubert, B.; et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: An FNCLCC and FFCD multicenter phase III trial. J. Clin. Oncol. 2011, 29, 1715–1721. [Google Scholar] [CrossRef] [PubMed]
- Ronellenfitsch, U.; Schwarzbach, M.; Hofheinz, R.; Kienle, P.; Kieser, M.; Slanger, T.E.; Burmeister, B.; Kelsen, D.; Niedzwiecki, D.; Schuhmacher, C.; et al. Preoperative chemo(radio)therapy versus primary surgery for gastroesophageal adenocarcinoma: Systematic review with meta-analysis combining individual patient and aggregate data. Eur. J. Cancer 2013, 49, 3149–3158. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D.; Stenning, S.P.; Smyth, E.C.; Okines, A.F.; Allum, W.H.; Rowley, S.; Stevenson, L.; Grabsch, H.I.; Alderson, D.; Crosby, T.; et al. Peri-operative chemotherapy with or without bevacizumab in operable oesophagogastric adenocarcinoma (UK Medical Research Council ST03): Primary analysis results of a multicentre, open-label, randomised phase 2-3 trial. Lancet Oncol. 2017, 18, 357–370. [Google Scholar] [CrossRef] [Green Version]
- Alderson, D.; Cunningham, D.; Nankivell, M.; Blazeby, J.M.; Griffin, S.M.; Crellin, A.; Grabsch, H.I.; Langer, R.; Pritchard, S.; Okines, A.; et al. Neoadjuvant cisplatin and fluorouracil versus epirubicin, cisplatin, and capecitabine followed by resection in patients with oesophageal adenocarcinoma (UK MRC OE05): An open-label, randomised phase 3 trial. Lancet Oncol. 2017, 18, 1249–1260. [Google Scholar] [CrossRef] [Green Version]
- Al-Batran, S.E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 2019, 393, 1948–1957. [Google Scholar] [CrossRef] [PubMed]
- Group, G.; Paoletti, X.; Oba, K.; Burzykowski, T.; Michiels, S.; Ohashi, Y.; Pignon, J.P.; Rougier, P.; Sakamoto, J.; Sargent, D.; et al. Benefit of adjuvant chemotherapy for resectable gastric cancer: A meta-analysis. JAMA 2010, 303, 1729–1737. [Google Scholar] [CrossRef]
- Noh, S.H.; Park, S.R.; Yang, H.K.; Chung, H.C.; Chung, I.J.; Kim, S.W.; Kim, H.H.; Choi, J.H.; Kim, H.K.; Yu, W.; et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1389–1396. [Google Scholar] [CrossRef]
- Yoshida, K.; Kodera, Y.; Kochi, M.; Ichikawa, W.; Kakeji, Y.; Sano, T.; Nagao, N.; Takahashi, M.; Takagane, A.; Watanabe, T.; et al. Addition of Docetaxel to Oral Fluoropyrimidine Improves Efficacy in Patients with Stage III Gastric Cancer: Interim Analysis of JACCRO GC-07, a Randomized Controlled Trial. J. Clin. Oncol. 2019, 37, 1296–1304. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Yin, Y.; Yin, Y.; Shen, C.; Wang, J.; Yin, X.; Chen, Z.; Zhou, Y.; Zhang, B. Comparative effectiveness of adjuvant treatments for resected gastric cancer: A network meta-analysis. Gastric. Cancer 2018, 21, 1031–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fornaro, L.; Vasile, E.; Aprile, G.; Goetze, T.O.; Vivaldi, C.; Falcone, A.; Al-Batran, S.E. Locally advanced gastro-oesophageal cancer: Recent therapeutic advances and research directions. Cancer Treat. Rev. 2018, 69, 90–100. [Google Scholar] [CrossRef]
- Fazio, N.; Biffi, R.; Maibach, R.; Hayoz, S.; Thierstein, S.; Brauchli, P.; Bernhard, J.; Stupp, R.; Andreoni, B.; Renne, G.; et al. Preoperative versus postoperative docetaxel-cisplatin-fluorouracil (TCF) chemotherapy in locally advanced resectable gastric carcinoma: 10-year follow-up of the SAKK 43/99 phase III trial. Ann. Oncol. 2016, 27, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.H.; Gao, P.; Song, Y.X.; Sun, J.X.; Chen, X.W.; Ma, B.; Yang, Y.C.; Wang, Z.N. Which is better for gastric cancer patients, perioperative or adjuvant chemotherapy: A meta-analysis. BMC Cancer 2016, 16, 631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Ende, T.; Ter Veer, E.; Machiels, M.; Mali, R.M.A.; Abe Nijenhuis, F.A.; de Waal, L.; Laarman, M.; Gisbertz, S.S.; Hulshof, M.; van Oijen, M.G.H.; et al. The efficacy and safety of (neo)adjuvant therapy for gastric cancer: A network meta-analysis. Cancers 2019, 11, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, J.; Cai, M.; Shuai, X.; Gao, J.; Wang, G.; Tao, K. Multimodal treatments for resectable gastric cancer: A systematic review and network meta-analysis. Eur. J. Surg. Oncol. 2019, 45, 1796–1805. [Google Scholar] [CrossRef]
- Lauren, P. The two histological main types of gastric carcinoma: Diffuse and so-called intestinal-type carcinoma. An attempt at a histo-clinical classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; Board, W.H.O.C.o.T.E. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Messager, M.; Lefevre, J.H.; Pichot-Delahaye, V.; Souadka, A.; Piessen, G.; Mariette, C.; Arnaud, J.P.; Balon, J.M.; Bonnetain, F.; Borie, F.; et al. The impact of perioperative chemotherapy on survival in patients with gastric signet ring cell adenocarcinoma: A multicenter comparative study. Ann. Surg. 2011, 254, 684–693; discussion 693. [Google Scholar] [CrossRef] [PubMed]
- Heger, U.; Blank, S.; Wiecha, C.; Langer, R.; Weichert, W.; Lordick, F.; Bruckner, T.; Dobritz, M.; Burian, M.; Springfeld, C.; et al. Is preoperative chemotherapy followed by surgery the appropriate treatment for signet ring cell containing adenocarcinomas of the esophagogastric junction and stomach? Ann. Surg. Oncol. 2014, 21, 1739–1748. [Google Scholar] [CrossRef] [PubMed]
- Pernot, S.; Dubreuil, O.; Aparicio, T.; Le Malicot, K.; Tougeron, D.; Lepere, C.; Lecaille, C.; Marthey, L.; Palle, J.; Bachet, J.B.; et al. Efficacy of a docetaxel-5FU-oxaliplatin regimen (TEFOX) in first-line treatment of advanced gastric signet ring cell carcinoma: An AGEO multicentre study. Br. J. Cancer 2018, 119, 424–428. [Google Scholar] [CrossRef]
- Eveno, C.; Adenis, A.; Bouche, O.; Le Malicot, K.; Hautefeuille, V.; Faroux, R.; Thirot Bidault, A.; Egreteau, J.; Meunier, B.; Mabro, M.; et al. Adjuvant chemotherapy versus perioperative chemotherapy (CTx) for resectable gastric signet ring cell (SRC) gastric cancer: A multicenter, randomized phase II study (PRODIGE 19). J. Clin. Oncol. 2019, 37 (Suppl. 15), 4019. [Google Scholar] [CrossRef]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.C.; Ng, K.F.; Yeh, T.S.; Cheng, C.T.; Lin, J.S.; Liu, Y.J.; Chuang, H.C.; Chen, T.C. Subtraction of Epstein-Barr virus and microsatellite instability genotypes from the Lauren histotypes: Combined molecular and histologic subtyping with clinicopathological and prognostic significance validated in a cohort of 1,248 cases. Int. J. Cancer 2019, 145, 3218–3230. [Google Scholar] [CrossRef] [PubMed]
- Sohn, B.H.; Hwang, J.E.; Jang, H.J.; Lee, H.S.; Oh, S.C.; Shim, J.J.; Lee, K.W.; Kim, E.H.; Yim, S.Y.; Lee, S.H.; et al. Clinical Significance of Four Molecular Subtypes of Gastric Cancer Identified by the Cancer Genome Atlas Project. Clin. Cancer Res. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Choi, Y.Y.; An, J.Y.; Shin, H.B.; Jo, A.; Choi, H.; Seo, S.H.; Bang, H.J.; Cheong, J.H.; Hyung, W.J.; et al. The benefit of microsatellite instability is attenuated by chemotherapy in stage II and stage III gastric cancer: Results from a large cohort with subgroup analyses. Int. J. Cancer 2015, 137, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Ciarpaglini, C.; Fleitas-Kanonnikoff, T.; Gambardella, V.; Llorca, M.; Mongort, C.; Mengual, R.; Nieto, G.; Navarro, L.; Huerta, M.; Rosello, S.; et al. Assessing molecular subtypes of gastric cancer: Microsatellite unstable and Epstein-Barr virus subtypes. Methods for detection and clinical and pathological implications. ESMO Open 2019, 4, e000470. [Google Scholar] [CrossRef] [Green Version]
- Polom, K.; Marano, L.; Marrelli, D.; De Luca, R.; Roviello, G.; Savelli, V.; Tan, P.; Roviello, F. Meta-analysis of microsatellite instability in relation to clinicopathological characteristics and overall survival in gastric cancer. Br. J. Surg. 2018, 105, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Pietrantonio, F.; Miceli, R.; Raimondi, A.; Kim, Y.W.; Kang, W.K.; Langley, R.E.; Choi, Y.Y.; Kim, K.M.; Nankivell, M.G.; Morano, F.; et al. Individual Patient Data Meta-Analysis of the Value of Microsatellite Instability As a Biomarker in Gastric Cancer. J. Clin. Oncol. 2019, 37, 3392–3400. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.T.; Cristescu, R.; Bass, A.J.; Kim, K.M.; Odegaard, J.I.; Kim, K.; Liu, X.Q.; Sher, X.; Jung, H.; Lee, M.; et al. Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat. Med. 2018, 24, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Ozguroglu, M.; Bang, Y.J.; Di Bartolomeo, M.; Mandala, M.; Ryu, M.H.; Fornaro, L.; Olesinski, T.; Caglevic, C.; Chung, H.C.; et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): A randomised, open-label, controlled, phase 3 trial. Lancet 2018, 392, 123–133. [Google Scholar] [CrossRef]
- Shapiro, J.; van Lanschot, J.J.B.; Hulshof, M.; van Hagen, P.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; Bonenkamp, J.J.; et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): Long-term results of a randomised controlled trial. Lancet Oncol. 2015, 16, 1090–1098. [Google Scholar] [CrossRef]
- Di Bartolomeo, M.; Pietrantonio, F.; Rulli, E.; Poli, D.; Berenato, R.; Caporale, M.; Bajetta, E.; Floriani, I. Impact on survival of timing and duration of adjuvant chemotherapy in radically resected gastric cancer. Tumori 2016, 102, e15–e19. [Google Scholar] [CrossRef]
- Greenleaf, E.K.; Kulaylat, A.N.; Hollenbeak, C.S.; Almhanna, K.; Wong, J. Timing of Adjuvant Chemotherapy and Impact on Survival for Resected Gastric Cancer. Ann. Surg. Oncol. 2016, 23, 4203–4213. [Google Scholar] [CrossRef]
- Jang, S.H.; Jung, Y.J.; Kim, M.G.; Kwon, S.J. The Prognostic Significance of Compliance with Postoperative Adjuvant Chemotherapy in Patients with Stage III Gastric Cancer: An Observational Study. J. Gastric. Cancer 2018, 18, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Park, H.S.; Jung, M.; Kim, H.S.; Kim, H.I.; An, J.Y.; Cheong, J.H.; Hyung, W.J.; Noh, S.H.; Kim, Y.I.; Chung, H.C.; et al. Proper timing of adjuvant chemotherapy affects survival in patients with stage 2 and 3 gastric cancer. Ann. Surg. Oncol. 2015, 22, 224–231. [Google Scholar] [CrossRef]
- Petrelli, F.; Zaniboni, A.; Ghidini, A.; Ghidini, M.; Turati, L.; Pizzo, C.; Ratti, M.; Libertini, M.; Tomasello, G. Timing of Adjuvant Chemotherapy and Survival in Colorectal, Gastric, and Pancreatic Cancer. A Systematic Review and Meta-Analysis. Cancers 2019, 11, 550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macdonald, J.S.; Smalley, S.R.; Benedetti, J.; Hundahl, S.A.; Estes, N.C.; Stemmermann, G.N.; Haller, D.G.; Ajani, J.A.; Gunderson, L.L.; Jessup, J.M.; et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N. Engl. J. Med. 2001, 345, 725–730. [Google Scholar] [CrossRef]
- Smalley, S.R.; Benedetti, J.K.; Haller, D.G.; Hundahl, S.A.; Estes, N.C.; Ajani, J.A.; Gunderson, L.L.; Goldman, B.; Martenson, J.A.; Jessup, J.M.; et al. Updated analysis of SWOG-directed intergroup study 0116: A phase III trial of adjuvant radiochemotherapy versus observation after curative gastric cancer resection. J. Clin. Oncol. 2012, 30, 2327–2333. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lim, D.H.; Lee, J.; Kang, W.K.; MacDonald, J.S.; Park, C.H.; Park, S.H.; Lee, S.H.; Kim, K.; Park, J.O.; et al. An observational study suggesting clinical benefit for adjuvant postoperative chemoradiation in a population of over 500 cases after gastric resection with D2 nodal dissection for adenocarcinoma of the stomach. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 1279–1285. [Google Scholar] [CrossRef]
- Lee, J.; Lim, D.H.; Kim, S.; Park, S.H.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Choi, M.G.; Sohn, T.S.; Noh, J.H.; et al. Phase III trial comparing capecitabine plus cisplatin versus capecitabine plus cisplatin with concurrent capecitabine radiotherapy in completely resected gastric cancer with D2 lymph node dissection: The ARTIST trial. J. Clin. Oncol. 2012, 30, 268–273. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, K.M.; Choi, M.G.; Lee, J.H.; Sohn, T.S.; Bae, J.M.; Kim, S.; Lee, S.J.; Kim, S.T.; Lee, J.; et al. Adjuvant Chemotherapy with or without Concurrent Radiotherapy for Patients with Stage IB Gastric Cancer: A Subgroup Analysis of the Adjuvant Chemoradiotherapy in Stomach Tumors (ARTIST) Phase III Trial. J. Gastric. Cancer 2018, 18, 348–355. [Google Scholar] [CrossRef]
- Kim, Y.; Park, S.H.; Kim, K.M.; Choi, M.G.; Lee, J.H.; Sohn, T.S.; Bae, J.M.; Kim, S.; Lee, S.J.; Kim, S.T.; et al. The Influence of Metastatic Lymph Node Ratio on the Treatment Outcomes in the Adjuvant Chemoradiotherapy in Stomach Tumors (ARTIST) Trial: A Phase III Trial. J. Gastric. Cancer 2016, 16, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Park, S.H.; Zang, D.Y.; Han, B.; Ji, J.H.; Kim, T.G.; Oh, S.Y.; Hwang, I.G.; Kim, J.H.; Shin, D.; Lim, D.H.; et al. ARTIST 2: Interim results of a phase III trial involving adjuvant chemotherapy and/or chemoradiotherapy after D2-gastrectomy in stage II/III gastric cancer (GC). J. Clin. Oncol. 2019, 37, 4001. [Google Scholar] [CrossRef]
- Stahl, M.; Walz, M.K.; Riera-Knorrenschild, J.; Stuschke, M.; Sandermann, A.; Bitzer, M.; Wilke, H.; Budach, W. Preoperative chemotherapy versus chemoradiotherapy in locally advanced adenocarcinomas of the oesophagogastric junction (POET): Long-term results of a controlled randomised trial. Eur. J. Cancer 2017, 81, 183–190. [Google Scholar] [CrossRef]
- von Dobeln, G.A.; Klevebro, F.; Jacobsen, A.B.; Johannessen, H.O.; Nielsen, N.H.; Johnsen, G.; Hatlevoll, I.; Glenjen, N.I.; Friesland, S.; Lundell, L.; et al. Neoadjuvant chemotherapy versus neoadjuvant chemoradiotherapy for cancer of the esophagus or gastroesophageal junction: Long-term results of a randomized clinical trial. Dis. Esophagus 2019, 32. [Google Scholar] [CrossRef]
- Petrelli, F.; Ghidini, M.; Barni, S.; Sgroi, G.; Passalacqua, R.; Tomasello, G. Neoadjuvant chemoradiotherapy or chemotherapy for gastroesophageal junction adenocarcinoma: A systematic review and meta-analysis. Gastric. Cancer 2019, 22, 245–254. [Google Scholar] [CrossRef] [Green Version]
- Pujara, D.; Mansfield, P.; Ajani, J.; Blum, M.; Elimova, E.; Chiang, Y.J.; Das, P.; Badgwell, B. Comprehensive geriatric assessment in patients with gastric and gastroesophageal adenocarcinoma undergoing gastrectomy. J. Surg. Oncol. 2015, 112, 883–887. [Google Scholar] [CrossRef] [Green Version]
- Tegels, J.J.; de Maat, M.F.; Hulsewe, K.W.; Hoofwijk, A.G.; Stoot, J.H. Value of geriatric frailty and nutritional status assessment in predicting postoperative mortality in gastric cancer surgery. J. Gastrointest. Surg. 2014, 18, 439–445; discussion 445–446. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.D.; Syn, N.L.; Moehler, M.; Grothe, W.; Yong, W.P.; Tai, B.C.; Ho, J.; Unverzagt, S. Chemotherapy for advanced gastric cancer. Cochrane Database Syst. Rev. 2017, 8, CD004064. [Google Scholar] [CrossRef] [PubMed]
- Ter Veer, E.; Haj Mohammad, N.; van Valkenhoef, G.; Ngai, L.L.; Mali, R.M.A.; Anderegg, M.C.; van Oijen, M.G.H.; van Laarhoven, H.W.M. The Efficacy and Safety of First-line Chemotherapy in Advanced Esophagogastric Cancer: A Network Meta-analysis. J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, N.H.; ter Veer, E.; Ngai, L.; Mali, R.; van Oijen, M.G.; van Laarhoven, H.W. Optimal first-line chemotherapeutic treatment in patients with locally advanced or metastatic esophagogastric carcinoma: Triplet versus doublet chemotherapy: A systematic literature review and meta-analysis. Cancer Metastasis Rev. 2015, 34, 429–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chau, I.; Norman, A.R.; Cunningham, D.; Waters, J.S.; Oates, J.; Ross, P.J. Multivariate prognostic factor analysis in locally advanced and metastatic esophago-gastric cancer--pooled analysis from three multicenter, randomized, controlled trials using individual patient data. J. Clin. Oncol. 2004, 22, 2395–2403. [Google Scholar] [CrossRef] [PubMed]
- Chau, I.; Ashley, S.; Cunningham, D. Validation of the Royal Marsden hospital prognostic index in advanced esophagogastric cancer using individual patient data from the REAL 2 study. J. Clin. Oncol. 2009, 27, e3–e4. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lim, T.; Uhm, J.E.; Park, K.W.; Park, S.H.; Lee, S.C.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Sohn, T.S.; et al. Prognostic model to predict survival following first-line chemotherapy in patients with metastatic gastric adenocarcinoma. Ann. Oncol. 2007, 18, 886–891. [Google Scholar] [CrossRef]
- Wang, J.; Qu, J.; Li, Z.; Che, X.; Zhang, J.; Liu, J.; Teng, Y.; Jin, B.; Zhao, M.; Liu, Y.; et al. A Prognostic Model in Metastatic or Recurrent Gastric Cancer Patients with Good Performance Status Who Received First-Line Chemotherapy. Transl. Oncol. 2016, 9, 256–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrams, T.; Hess, L.M.; Zhu, Y.E.; Schelman, W.; Liepa, A.M.; Fuchs, C. Predictors of heterogeneity in the first-line treatment of patients with advanced/metastatic gastric cancer in the U.S. Gastric. Cancer 2018, 21, 738–744. [Google Scholar] [CrossRef] [Green Version]
- Al-Batran, S.E.; Pauligk, C.; Homann, N.; Hartmann, J.T.; Moehler, M.; Probst, S.; Rethwisch, V.; Stoehlmacher-Williams, J.; Prasnikar, N.; Hollerbach, S.; et al. The feasibility of triple-drug chemotherapy combination in older adult patients with oesophagogastric cancer: A randomised trial of the Arbeitsgemeinschaft Internistische Onkologie (FLOT65+). Eur. J. Cancer 2013, 49, 835–842. [Google Scholar] [CrossRef]
- Smyth, E.C.; Nilsson, M.; Grabsch, H.I.; van Grieken, N.C.; Lordick, F. Gastric cancer. Lancet 2020, 396, 635–648. [Google Scholar] [CrossRef]
- AIOM. Linee Guida Neoplasie Dello Stomaco e Della Giunzione Gastro-Esofagea. Available online: https://www.aiom.it/wp-content/uploads/2019/10/2019_LG_AIOM_Stomaco_giun-gastr-esof.pdf (accessed on 14 March 2021).
- Muro, K.; Van Cutsem, E.; Narita, Y.; Pentheroudakis, G.; Baba, E.; Li, J.; Ryu, M.H.; Zamaniah, W.W.; Yong, W.P.; Yeh, K.H.; et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with metastatic oesophageal cancer: A JSMO-ESMO initiative endorsed by CSCO, KSMO, MOS, SSO and TOS. Ann Oncol. 2019, 30, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Smyth, E.C.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D.; Committee, E.G. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v38–v49. [Google Scholar] [CrossRef]
- Wilke, H.; Muro, K.; Van Cutsem, E.; Oh, S.C.; Bodoky, G.; Shimada, Y.; Hironaka, S.; Sugimoto, N.; Lipatov, O.; Kim, T.Y.; et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): A double-blind, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1224–1235. [Google Scholar] [CrossRef]
- Kim, H.S.; Kim, H.J.; Kim, S.Y.; Kim, T.Y.; Lee, K.W.; Baek, S.K.; Kim, T.Y.; Ryu, M.H.; Nam, B.H.; Zang, D.Y. Second-line chemotherapy versus supportive cancer treatment in advanced gastric cancer: A meta-analysis. Ann. Oncol. 2013, 24, 2850–2854. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, C.S.; Tomasek, J.; Yong, C.J.; Dumitru, F.; Passalacqua, R.; Goswami, C.; Safran, H.; Dos Santos, L.V.; Aprile, G.; Ferry, D.R.; et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): An international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet 2014, 383, 31–39. [Google Scholar] [CrossRef]
- Guimbaud, R.; Louvet, C.; Ries, P.; Ychou, M.; Maillard, E.; Andre, T.; Gornet, J.M.; Aparicio, T.; Nguyen, S.; Azzedine, A.; et al. Prospective, randomized, multicenter, phase III study of fluorouracil, leucovorin, and irinotecan versus epirubicin, cisplatin, and capecitabine in advanced gastric adenocarcinoma: A French intergroup (Federation Francophone de Cancerologie Digestive, Federation Nationale des Centres de Lutte Contre le Cancer, and Groupe Cooperateur Multidisciplinaire en Oncologie) study. J. Clin. Oncol. 2014, 32, 3520–3526. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, M.; Stoss, O.; Shi, D.; Buttner, R.; van de Vijver, M.; Kim, W.; Ochiai, A.; Ruschoff, J.; Henkel, T. Assessment of a HER2 scoring system for gastric cancer: Results from a validation study. Histopathology 2008, 52, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Yagi, S.; Wakatsuki, T.; Yamamoto, N.; Chin, K.; Takahari, D.; Ogura, M.; Ichimura, T.; Nakayama, I.; Osumi, H.; Shinozaki, E.; et al. Clinical significance of intratumoral HER2 heterogeneity on trastuzumab efficacy using endoscopic biopsy specimens in patients with advanced HER2 positive gastric cancer. Gastric. Cancer 2019, 22, 518–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.E.; Park, K.U.; Yoo, S.B.; Nam, S.K.; Park, D.J.; Kim, H.H.; Lee, H.S. Clinical significance of intratumoral HER2 heterogeneity in gastric cancer. Eur. J. Cancer 2013, 49, 1448–1457. [Google Scholar] [CrossRef]
- Warneke, V.S.; Behrens, H.M.; Boger, C.; Becker, T.; Lordick, F.; Ebert, M.P.; Rocken, C. Her2/neu testing in gastric cancer: Evaluating the risk of sampling errors. Ann. Oncol. 2013, 24, 725–733. [Google Scholar] [CrossRef]
- Park, S.R.; Park, Y.S.; Ryu, M.H.; Ryoo, B.Y.; Woo, C.G.; Jung, H.Y.; Lee, J.H.; Lee, G.H.; Kang, Y.K. Extra-gain of HER2-positive cases through HER2 reassessment in primary and metastatic sites in advanced gastric cancer with initially HER2-negative primary tumours: Results of GASTric cancer HER2 reassessment study 1 (GASTHER1). Eur. J. Cancer 2016, 53, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Bozzetti, C.; Negri, F.V.; Lagrasta, C.A.; Crafa, P.; Bassano, C.; Tamagnini, I.; Gardini, G.; Nizzoli, R.; Leonardi, F.; Gasparro, D.; et al. Comparison of HER2 status in primary and paired metastatic sites of gastric carcinoma. Br. J. Cancer 2011, 104, 1372–1376. [Google Scholar] [CrossRef] [Green Version]
- Uchoa Guimaraes, C.T.; Ferreira Martins, N.N.; Cristina da Silva Oliveira, K.; Almeida, C.M.; Pinheiro, T.M.; Gigek, C.O.; Roberto de Araujo Cavallero, S.; Assumpcao, P.P.; Cardoso Smith, M.A.; Burbano, R.R.; et al. Liquid biopsy provides new insights into gastric cancer. Oncotarget 2018, 9, 15144–15156. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, K.; Yamaguchi, K.; Okumura, N.; Tanahashi, T.; Kodera, Y. Is conversion therapy possible in stage IV gastric cancer: The proposal of new biological categories of classification. Gastric. Cancer 2016, 19, 329–338. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Huang, X.; Song, Y.; Gao, P.; Zhou, C.; Guo, Z.; Shi, J.; Wu, Z.; Wang, Z. Conversion Surgery for Stage IV Gastric Cancer. Front. Oncol. 2019, 9, 1158. [Google Scholar] [CrossRef] [Green Version]
- Cascinu, S.; Graziano, F.; Barni, S.; Labianca, R.; Comella, G.; Casaretti, R.; Frontini, L.; Catalano, V.; Baldelli, A.M.; Catalano, G. A phase II study of sequential chemotherapy with docetaxel after the weekly PELF regimen in advanced gastric cancer. A report from the Italian group for the study of digestive tract cancer. Br. J. Cancer 2001, 84, 470–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aurello, P.; Petrucciani, N.; Giulitti, D.; Campanella, L.; D’Angelo, F.; Ramacciato, G. Pulmonary metastases from gastric cancer: Is there any indication for lung metastasectomy? A systematic review. Med. Oncol. 2016, 33, 9. [Google Scholar] [CrossRef] [PubMed]
- Montagnani, F.; Crivelli, F.; Aprile, G.; Vivaldi, C.; Pecora, I.; De Vivo, R.; Clerico, M.A.; Fornaro, L. Long-term survival after liver metastasectomy in gastric cancer: Systematic review and meta-analysis of prognostic factors. Cancer Treat. Rev. 2018, 69, 11–20. [Google Scholar] [CrossRef]
- Dahdaleh, F.S.; Turaga, K.K. Evolving Treatment Strategies and Outcomes in Advanced Gastric Cancer with Peritoneal Metastasis. Surg. Oncol. Clin. N. Am. 2018, 27, 519–537. [Google Scholar] [CrossRef]
- Al-Batran, S.E.; Homann, N.; Pauligk, C.; Illerhaus, G.; Martens, U.M.; Stoehlmacher, J.; Schmalenberg, H.; Luley, K.B.; Prasnikar, N.; Egger, M.; et al. Effect of Neoadjuvant Chemotherapy Followed by Surgical Resection on Survival in Patients With Limited Metastatic Gastric or Gastroesophageal Junction Cancer: The AIO-FLOT3 Trial. JAMA Oncol. 2017, 3, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Iacovelli, R.; Pietrantonio, F.; Farcomeni, A.; Maggi, C.; Palazzo, A.; Ricchini, F.; de Braud, F.; Di Bartolomeo, M. Chemotherapy or targeted therapy as second-line treatment of advanced gastric cancer. A systematic review and meta-analysis of published studies. PLoS ONE 2014, 9, e108940. [Google Scholar] [CrossRef] [Green Version]
- Makiyama, A.; Sukawa, Y.; Kashiwada, T.; Kawada, J.; Hosokawa, A.; Horie, Y.; Tsuji, A.; Moriwaki, T.; Tanioka, H.; Shinozaki, K.; et al. Randomized, Phase II Study of Trastuzumab Beyond Progression in Patients With HER2-Positive Advanced Gastric or Gastroesophageal Junction Cancer: WJOG7112G (T-ACT Study). J. Clin. Oncol. 2020, JCO1903077. [Google Scholar] [CrossRef]
- Ford, H.E.; Marshall, A.; Bridgewater, J.A.; Janowitz, T.; Coxon, F.Y.; Wadsley, J.; Mansoor, W.; Fyfe, D.; Madhusudan, S.; Middleton, G.W.; et al. Docetaxel versus active symptom control for refractory oesophagogastric adenocarcinoma (COUGAR-02): An open-label, phase 3 randomised controlled trial. Lancet Oncol. 2014, 15, 78–86. [Google Scholar] [CrossRef]
- Thuss-Patience, P.C.; Kretzschmar, A.; Bichev, D.; Deist, T.; Hinke, A.; Breithaupt, K.; Dogan, Y.; Gebauer, B.; Schumacher, G.; Reichardt, P. Survival advantage for irinotecan versus best supportive care as second-line chemotherapy in gastric cancer—A randomised phase III study of the Arbeitsgemeinschaft Internistische Onkologie (AIO). Eur. J. Cancer 2011, 47, 2306–2314. [Google Scholar] [CrossRef] [PubMed]
- Hironaka, S.; Ueda, S.; Yasui, H.; Nishina, T.; Tsuda, M.; Tsumura, T.; Sugimoto, N.; Shimodaira, H.; Tokunaga, S.; Moriwaki, T.; et al. Randomized, open-label, phase III study comparing irinotecan with paclitaxel in patients with advanced gastric cancer without severe peritoneal metastasis after failure of prior combination chemotherapy using fluoropyrimidine plus platinum: WJOG 4007 trial. J. Clin. Oncol. 2013, 31, 4438–4444. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Maeng, C.H.; Kim, T.Y.; Zang, D.Y.; Kim, Y.H.; Hwang, I.G.; Oh, S.C.; Chung, J.S.; Song, H.S.; Kim, J.W.; et al. A Phase III Study to Compare the Efficacy and Safety of Paclitaxel Versus Irinotecan in Patients with Metastatic or Recurrent Gastric Cancer Who Failed in First-line Therapy (KCSG ST10-01). Oncologist 2019, 24, 18. [Google Scholar] [CrossRef] [Green Version]
- Di Bartolomeo, M.; Niger, M.; Tirino, G.; Petrillo, A.; Berenato, R.; Laterza, M.M.; Pietrantonio, F.; Morano, F.; Antista, M.; Lonardi, S.; et al. Ramucirumab as Second-Line Therapy in Metastatic Gastric Cancer: Real-World Data from the RAMoss Study. Target Oncol. 2018, 13, 227–234. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Muro, K.; Cunningham, D.; Bodoky, G.; Sobrero, A.; Cascinu, S.; Ajani, J.; Oh, S.C.; Al-Batran, S.E.; Wainberg, Z.A.; et al. Biomarker analyses of second-line ramucirumab in patients with advanced gastric cancer from RAINBOW, a global, randomized, double-blind, phase 3 study. Eur. J. Cancer 2020, 127, 150–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanotto, V.; Cordio, S.; Pasquini, G.; Fontanella, C.; Rimassa, L.; Leone, F.; Rosati, G.; Santini, D.; Giampieri, R.; Di Donato, S.; et al. Prognostic factors in 868 advanced gastric cancer patients treated with second-line chemotherapy in the real world. Gastric. Cancer 2017, 20, 825–833. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, C.S.; Muro, K.; Tomasek, J.; Van Cutsem, E.; Cho, J.Y.; Oh, S.C.; Safran, H.; Bodoky, G.; Chau, I.; Shimada, Y.; et al. Prognostic Factor Analysis of Overall Survival in Gastric Cancer from Two Phase III Studies of Second-line Ramucirumab (REGARD and RAINBOW) Using Pooled Patient Data. J. Gastric. Cancer 2017, 17, 132–144. [Google Scholar] [CrossRef] [Green Version]
- Iwasa, S.; Kudo, T.; Takahari, D.; Hara, H.; Kato, K.; Satoh, T. Practical guidance for the evaluation of disease progression and the decision to change treatment in patients with advanced gastric cancer receiving chemotherapy. Int. J. Clin. Oncol. 2020. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Barretta, F.; Fanotto, V.; Park, S.H.; Morano, F.; Fuca, G.; Niger, M.; Prisciandaro, M.; Silvestris, N.; Bergamo, F.; et al. Estimating Survival Probabilities of Advanced Gastric Cancer Patients in the Second-Line Setting: The Gastric Life Nomogram. Oncology 2018, 95, 344–352. [Google Scholar] [CrossRef]
- Muro, K.; Cho, J.Y.; Bodoky, G.; Goswami, C.; Chao, Y.; Dos Santos, L.V.; Shimada, Y.; Topuzov, E.; Van Cutsem, E.; Tabernero, J.; et al. Age does not influence efficacy of ramucirumab in advanced gastric cancer: Subgroup analyses of REGARD and RAINBOW. J. Gastroenterol. Hepatol. 2018, 33, 814–824. [Google Scholar] [CrossRef] [PubMed]
- Klempner, S.J.; Maron, S.B.; Chase, L.; Lomnicki, S.; Wainberg, Z.A.; Catenacci, D.V.T. Initial Report of Second-Line FOLFIRI in Combination with Ramucirumab in Advanced Gastroesophageal Adenocarcinomas: A Multi-Institutional Retrospective Analysis. Oncologist 2019, 24, 475–482. [Google Scholar] [CrossRef] [Green Version]
- Lorenzen, S.; Thuss-Patience, P.C.; Pauligk, C.; Goekkurt, E.; Ettrich, T.J.; Lordick, F.; Stahl, M.; Reichardt, P.; Soekler, M.; Pink, D.; et al. FOLFIRI plus ramucirumab versus paclitaxel plus ramucirumab as second-line therapy for patients with advanced or metastatic gastroesophageal adenocarcinoma with or without prior docetaxel: Results from the phase II RAMIRIS Study of the AIO. J. Clin. Oncol. 2020, 38, 4514. [Google Scholar] [CrossRef]
- Aprile, G.; Fanotto, V.; Garattini, S.K.; Bozza, C.; DE CAR-LO, E.; Fontanella, C.; Bonotto, M.; Basile, D.; Cattaneo, M.; Casagrande, M.; et al. The concept of maintenance: May we move it to gastric, pancreatic and liver cancers? WCRJ 2016, 3, e713. [Google Scholar]
- Qiu, M.Z.; Wei, X.L.; Zhang, D.S.; Jin, Y.; Zhou, Y.X.; Wang, D.S.; Ren, C.; Bai, L.; Luo, H.Y.; Wang, Z.Q.; et al. Efficacy and safety of capecitabine as maintenance treatment after first-line chemotherapy using oxaliplatin and capecitabine in advanced gastric adenocarcinoma patients: A prospective observation. Tumour Biol. 2014, 35, 4369–4375. [Google Scholar] [CrossRef] [PubMed]
- Eren, O.O.; Ozturk, M.A.; Sonmez, O.U.; Oyan, B. Safety, Feasibility, and Efficacy of Capecitabine Maintenance in Patients with Advanced Gastric Cancer: A Retrospective Study. Am. J. Ther. 2016, 23, e1493–e1497. [Google Scholar] [CrossRef] [Green Version]
- Petrioli, R.; Francini, E.; Roviello, F.; Marrelli, D.; Miano, S.T.; Fiaschi, A.I.; Laera, L.; Bellini, M.A.; Roviello, G. Treatment of advanced oesophagogastric cancer with FOLFOX-4 regimen followed by leucovorin/bolus and continuous infusion 5-FU as maintenance chemotherapy in patients aged >/= 75 years with impaired performance status. J. Geriatr. Oncol. 2015, 6, 380–386. [Google Scholar] [CrossRef]
- Di Bartolomeo, M.; Niger, M.; Morano, F.; Corallo, S.; Antista, M.; Tamberi, S.; Lonardi, S.; Di Donato, S.; Berardi, R.; Scartozzi, M.; et al. Assessment of ramucirumab plus paclitaxel as switch maintenance versus continuation of first-line chemotherapy in patients with advanced HER-2 negative gastric or gastroesophageal junction cancers: The ARMANI phase III trial. BMC Cancer 2019, 19, 283. [Google Scholar] [CrossRef] [PubMed]
- Haag, G.M.; Stocker, G.; Quidde, J.; Jaeger, D.; Lordick, F. Randomized controlled trial of S-1 maintenance therapy in metastatic esophagogastric cancer—The multinational MATEO study. BMC Cancer 2017, 17, 509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.W.; Ahn, M.S.; Jeong, G.S.; Lee, H.W.; Jeong, S.H.; Kang, S.Y.; Park, J.S.; Choi, J.H.; Sheen, S.S. The role of third-line chemotherapy in recurrent or metastatic gastric cancer: A cohort study with propensity score matching analysis. Medicine 2018, 97, e12588. [Google Scholar] [CrossRef]
- Fanotto, V.; Uccello, M.; Pecora, I.; Rimassa, L.; Leone, F.; Rosati, G.; Santini, D.; Giampieri, R.; Di Donato, S.; Tomasello, G.; et al. Outcomes of Advanced Gastric Cancer Patients Treated with at Least Three Lines of Systemic Chemotherapy. Oncologist 2018, 23, 272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shitara, K.; Doi, T.; Dvorkin, M.; Mansoor, W.; Arkenau, H.T.; Prokharau, A.; Alsina, M.; Ghidini, M.; Faustino, C.; Gorbunova, V.; et al. Trifluridine/tipiracil versus placebo in patients with heavily pretreated metastatic gastric cancer (TAGS): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2018, 19, 1437–1448. [Google Scholar] [CrossRef]
- Tabernero, J.; Alsina, M.; Shitara, K.; Doi, T.; Dvorkin, M.; Mansoor, W.; Arkenau, H.T.; Prokharau, A.; Ghidini, M.; Faustino, C.; et al. Health-related quality of life associated with trifluridine/tipiracil in heavily pretreated metastatic gastric cancer: Results from TAGS. Gastric. Cancer 2020, 23, 689–698. [Google Scholar] [CrossRef] [Green Version]
- Shitara, K.; Van Cutsem, E.; Bang, Y.J.; Fuchs, C.S.; Wyrwicz, L.; Lee, K.W.; Kudaba, I.; Garrido, M.; Chung, H.C.; Castro, H.R.; et al. Pembrolizumab With or Without Chemotherapy vs Chemotherapy in Patients with Advanced G/GEJ Cancer (GC) Including Outcomes According to Microsatellite Instability-High (MSI-H) Status in KEYNOTE-062. Ann. Oncol. 2019, 30, v878–v879. [Google Scholar] [CrossRef]
- Moehler, M.H.; Dvorkin, M.; Ozguroglu, M.; Ryu, M.; Muntean, A.S.; Lonardi, S.; Nechaeva, M.; Campos Bragagnoli, A.S.; Coskun, H.S.; Gracián, A.C.; et al. Results of the JAVELIN Gastric 100 phase 3 trial: Avelumab maintenance following first-line (1L) chemotherapy (CTx) vs continuation of CTx for HER2− advanced gastric or gastroesophageal junction cancer (GC/GEJC). J. Clin. Oncol. 2020, 38, 278. [Google Scholar] [CrossRef]
- Kang, Y.K.; Boku, N.; Satoh, T.; Ryu, M.H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.S.; Muro, K.; Kang, W.K.; et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 2461–2471. [Google Scholar] [CrossRef]
- Bang, Y.J.; Ruiz, E.Y.; Van Cutsem, E.; Lee, K.W.; Wyrwicz, L.; Schenker, M.; Alsina, M.; Ryu, M.H.; Chung, H.C.; Evesque, L.; et al. Phase III, randomised trial of avelumab versus physician’s choice of chemotherapy as third-line treatment of patients with advanced gastric or gastro-oesophageal junction cancer: Primary analysis of JAVELIN Gastric 300. Ann. Oncol. 2018, 29, 2052–2060. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S.; et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017, 357, 409–413. [Google Scholar] [CrossRef] [Green Version]
- Mandal, R.; Samstein, R.M.; Lee, K.W.; Havel, J.J.; Wang, H.; Krishna, C.; Sabio, E.Y.; Makarov, V.; Kuo, F.; Blecua, P.; et al. Genetic diversity of tumors with mismatch repair deficiency influences anti-PD-1 immunotherapy response. Science 2019, 364, 485–491. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, S.; Sahnane, N.; Tibiletti, M.G.; Magnoli, F.; Vanoli, A.; Sessa, F.; Chiaravalli, A.M. EBV(+) and MSI Gastric Cancers Harbor High PD-L1/PD-1 Expression and High CD8(+) Intratumoral Lymphocytes. Cancers 2018, 10, 102. [Google Scholar] [CrossRef] [Green Version]
- Panda, A.; Mehnert, J.M.; Hirshfield, K.M.; Riedlinger, G.; Damare, S.; Saunders, T.; Kane, M.; Sokol, L.; Stein, M.N.; Poplin, E.; et al. Immune Activation and Benefit From Avelumab in EBV-Positive Gastric Cancer. J. Natl. Cancer Inst. 2018, 110, 316–320. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Valderrama, A.; Bang, Y.J.; Fuchs, C.; Shitara, K.; Janjigian, Y.Y.; Qin, S.; Larson, T.; Shankaran, V.; Stein, S.; et al. Health-Related Quality of Life (HRQoL) Impact of Pembrolizumab (P) Versus Chemotherapy (C) as First-Line (1L) Treatment in PD-L1–Positive Advanced Gastric or Gastroesophageal Junction (G/GEJ) Adenocarcinoma. Ann. Oncol. 2019, 30, v879. [Google Scholar] [CrossRef]
- Auer, R.C.; Sivajohanathan, D.; Biagi, J.; Conner, J.; Kennedy, E.; May, T. Indications for hyperthermic intraperitoneal chemotherapy with cytoreductive surgery: A systematic review. Eur. J. Cancer 2020, 127, 76–95. [Google Scholar] [CrossRef]
- Auer, R.C.; Sivajohanathan, D.; Biagi, J.; Conner, J.; Kennedy, E.; May, T. Indications for hyperthermic intraperitoneal chemotherapy with cytoreductive surgery: A clinical practice guideline. Curr. Oncol. 2020, 27, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.J.; Huang, C.Q.; Suo, T.; Mei, L.J.; Yang, G.L.; Cheng, F.L.; Zhou, Y.F.; Xiong, B.; Yonemura, Y.; Li, Y. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy improves survival of patients with peritoneal carcinomatosis from gastric cancer: Final results of a phase III randomized clinical trial. Ann. Surg. Oncol. 2011, 18, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Bozzetti, F.; Arends, J.; Lundholm, K.; Micklewright, A.; Zurcher, G.; Muscaritoli, M. ESPEN Guidelines on Parenteral Nutrition: Non-surgical oncology. Clin. Nutr. 2009, 28, 445–454. [Google Scholar] [CrossRef]
- Virizuela, J.A.; Camblor-Alvarez, M.; Luengo-Perez, L.M.; Grande, E.; Alvarez-Hernandez, J.; Sendros-Madrono, M.J.; Jimenez-Fonseca, P.; Cervera-Peris, M.; Ocon-Breton, M.J. Nutritional support and parenteral nutrition in cancer patients: An expert consensus report. Clin. Transl. Oncol. 2018, 20, 619–629. [Google Scholar] [CrossRef]
- Cotogni, P.; De Carli, L.; Passera, R.; Amerio, M.L.; Agnello, E.; Fadda, M.; Ossola, M.; Monge, T.; De Francesco, A.; Bozzetti, F. Longitudinal study of quality of life in advanced cancer patients on home parenteral nutrition. Cancer Med. 2017, 6, 1799–1806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, M.; Zhou, Y.X.; Jin, Y.; Wang, Z.X.; Wei, X.L.; Han, H.Y.; Ye, W.F.; Zhou, Z.W.; Zhang, D.S.; Wang, F.H.; et al. Nutrition support can bring survival benefit to high nutrition risk gastric cancer patients who received chemotherapy. Support. Care Cancer 2015, 23, 1933–1939. [Google Scholar] [CrossRef] [PubMed]
- Senesse, P.; Tadmouri, A.; Culine, S.; Dufour, P.R.; Seys, P.; Radji, A.; Rotarski, M.; Balian, A.; Chambrier, C. A prospective observational study assessing home parenteral nutrition in patients with gastrointestinal cancer: Benefits for quality of life. J. Pain Symptom Manag. 2015, 49, 183–191.e2. [Google Scholar] [CrossRef]
- Ozcelik, H.; Gozum, S.; Ozer, Z. Is home parenteral nutrition safe for cancer patients? Positive effects and potential catheter-related complications: A systematic review. Eur. J. Cancer Care 2019, 28, e13003. [Google Scholar] [CrossRef] [PubMed]
- Deans, D.A.; Tan, B.H.; Wigmore, S.J.; Ross, J.A.; de Beaux, A.C.; Paterson-Brown, S.; Fearon, K.C. The influence of systemic inflammation, dietary intake and stage of disease on rate of weight loss in patients with gastro-oesophageal cancer. Br. J. Cancer 2009, 100, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Haj Mohammad, N.; Bernards, N.; van Putten, M.; Lemmens, V.; van Oijen, M.G.H.; van Laarhoven, H.W.M. Volume-outcome relation in palliative systemic treatment of metastatic oesophagogastric cancer. Eur. J. Cancer 2017, 78, 28–36. [Google Scholar] [CrossRef]
- Kim, E.Y.; Song, K.Y.; Lee, J. Does Hospital Volume Really Affect the Surgical and Oncological Outcomes of Gastric Cancer in Korea? J. Gastric. Cancer 2017, 17, 246–254. [Google Scholar] [CrossRef] [Green Version]






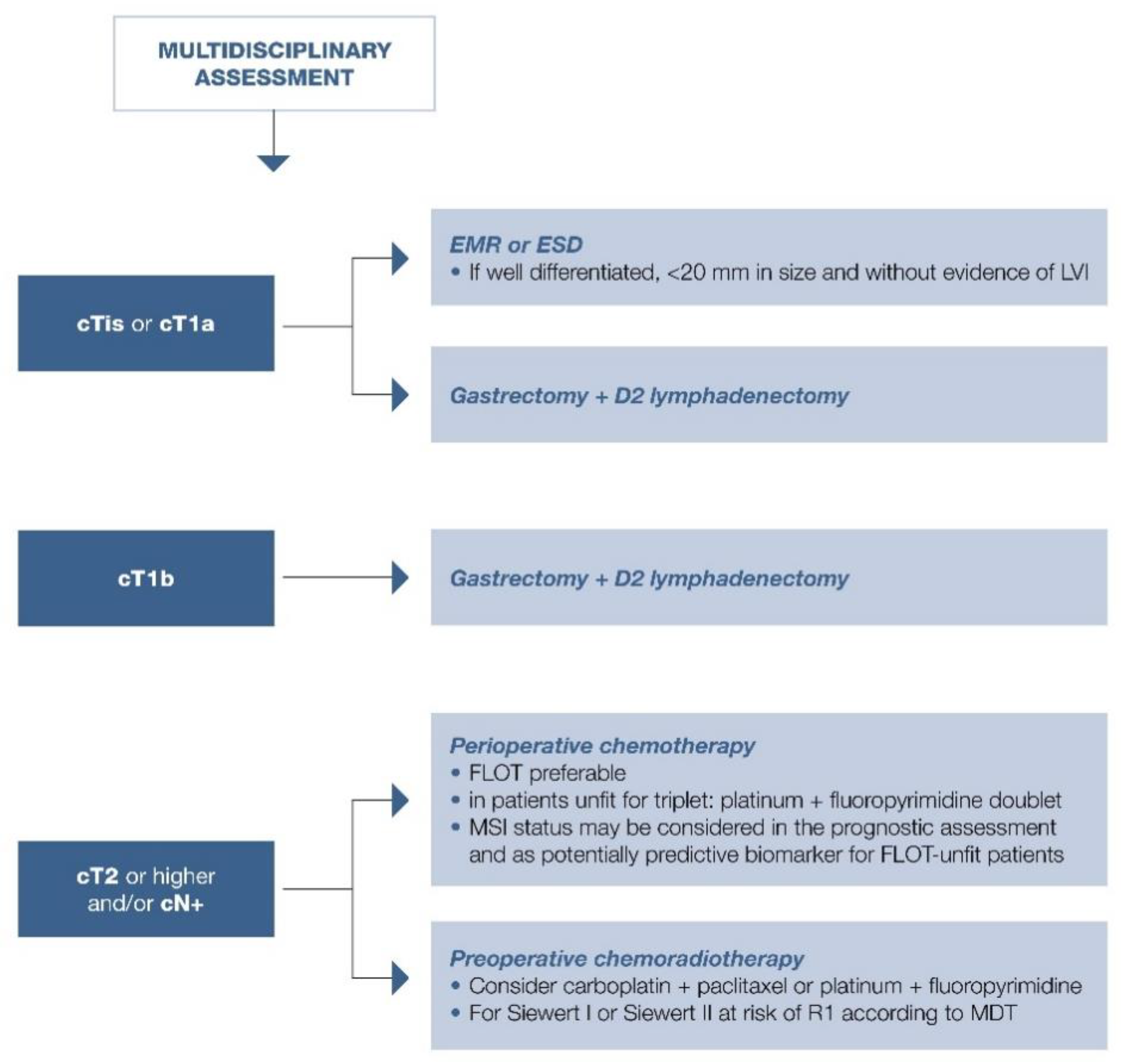{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Precancerous Conditions | Timing of Endoscopic Follow-Up | Statement |
|---|---|---|
| Intestinal metaplasia limited to the gastric antrum or body | Every 3 years | Endoscopic surveillance with EGDS at least every 3 years must be considered mainly for patients with familial gastric neoplasia, autoimmune gastritis, or non-eradication of H. pylori infection. |
| Chronic atrophic gastritis and/or diffuse intestinal metaplasia. | Every 1–2 years | Scheduled endoscopic follow-up with controls 1–2 years is recommended. |
| Gastric dysplasia | Within 6 months for high-grade dysplasia and within 1 year for low-grade dysplasia. | In patients with dysplasia without suspicious lesions, first, an endoscopic evaluation at a third-level center should be performed, and possibly a review by expert pathologists to confirm the previous diagnosis and guide endoscopic follow-up. In the absence of evident lesions, even at the subsequent endoscopic evaluation, a new EGDS must be performed within 6 months for high-grade dysplasia and within 1 year for low-grade dysplasia. |
| Exam | Timing | Statement |
|---|---|---|
| CT scan | Diagnosis | CT scan is essential in gastric cancer staging |
| Echoendoscopy | Diagnosis | EUS is the most accurate staging method for definition of T parameter; its execution is therefore recommended when this impacts the treatment approach (endoscopic resection, upfront surgery, perioperative treatment). |
| FDG PET/CT | Diagnosis | Consider FDG PET/CT with 18F-FDG in addition to radiologic imaging in patients with locally advanced gastric cancer when there is no evidence of metastatic disease and in case of suspected secondary lesions at CT scan. |
| CT scan | Response to neoadjuvant treatment | CT scan is the gold standard in evaluating the response after neoadjuvant chemotherapy. |
| Echoendoscopy | Response to neoadjuvant treatment | The usefulness of EUS in evaluating the response after neoadjuvant chemotherapy or chemoradiotherapy appears limited and so it should not be used as restaging method outside clinical trials. |
| FDG PET/CT | Response to neoadjuvant treatment | FDG PET/CT during treatment or after the end of treatment should be useful to identify patients without any benefit from neoadjuvant treatment; however, this role is marginal outside clinical trials. |
| CT scan | Metastatic | Imaging for disease assessment should be preferentially performed every 2 months with metastatic disease and should be accompanied by detailed and close monitoring of patient clinical conditions. |
| Nutritional Action | Stage of Disease | Statement |
|---|---|---|
| Role of nutrition experts | All | The presence of a clinical nutrition specialist in the MDT allows the possibility of performing multimodal treatments. The nutrition team should include at least one physician (internist, gastroenterologist, endocrinologist, or nutritionist) and a dietitian. |
| Nutritional screening | All | Validated screening test to assess the presence of malnutrition should be provided to all patients with gastric cancer before any anticancer treatment. For pathologic screening, the nutritional team must be involved in setting up an intervention. |
| Nutritional counseling | All | For pathologic nutritional screening, nutritional counseling should be the first intervention. Nutritional counseling aims to maintain adequate weight and QoL during chemotherapy. |
| Enteral nutrition | Localized disease | Enteral nutrition support in patients treated with radical gastrectomy should be considered in (neo-)adjuvant settings. |
| Parenteral nutrition | Metastatic | Parenteral nutrition is effective in improving nutritional status and QoL, and in some selected patients with advanced gastric cancer. It is a valid therapeutic option for malnourished patients with advanced gastric cancer. |
| Nutritional status assessment | Metastatic | Nutritional status assessment must be performed upfront in all patients who are candidates for systemic therapies. The need for nutritional support and the program for such support should be established by a dedicated nutrition expert. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fornaro, L.; Spallanzani, A.; de Vita, F.; D’Ugo, D.; Falcone, A.; Lorenzon, L.; Tirino, G.; Cascinu, S.; on behalf of GAIN (GAstric Cancer Italian Network). Beyond the Guidelines: The Grey Zones of the Management of Gastric Cancer. Consensus Statements from the Gastric Cancer Italian Network (GAIN). Cancers 2021, 13, 1304. https://doi.org/10.3390/cancers13061304
Fornaro L, Spallanzani A, de Vita F, D’Ugo D, Falcone A, Lorenzon L, Tirino G, Cascinu S, on behalf of GAIN (GAstric Cancer Italian Network). Beyond the Guidelines: The Grey Zones of the Management of Gastric Cancer. Consensus Statements from the Gastric Cancer Italian Network (GAIN). Cancers. 2021; 13(6):1304. https://doi.org/10.3390/cancers13061304
Chicago/Turabian StyleFornaro, Lorenzo, Andrea Spallanzani, Ferdinando de Vita, Domenico D’Ugo, Alfredo Falcone, Laura Lorenzon, Giuseppe Tirino, Stefano Cascinu, and on behalf of GAIN (GAstric Cancer Italian Network). 2021. "Beyond the Guidelines: The Grey Zones of the Management of Gastric Cancer. Consensus Statements from the Gastric Cancer Italian Network (GAIN)" Cancers 13, no. 6: 1304. https://doi.org/10.3390/cancers13061304