Games and Health Education for Diabetes Control: A Systematic Review with Meta-Analysis

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Elegibility Criteria
2.2. Information Sources and Search
2.3. Study Selection and Risk of Bias
2.4. Data Items and Collection Process
2.5. Data Analysis and Summary of Results
3. Results
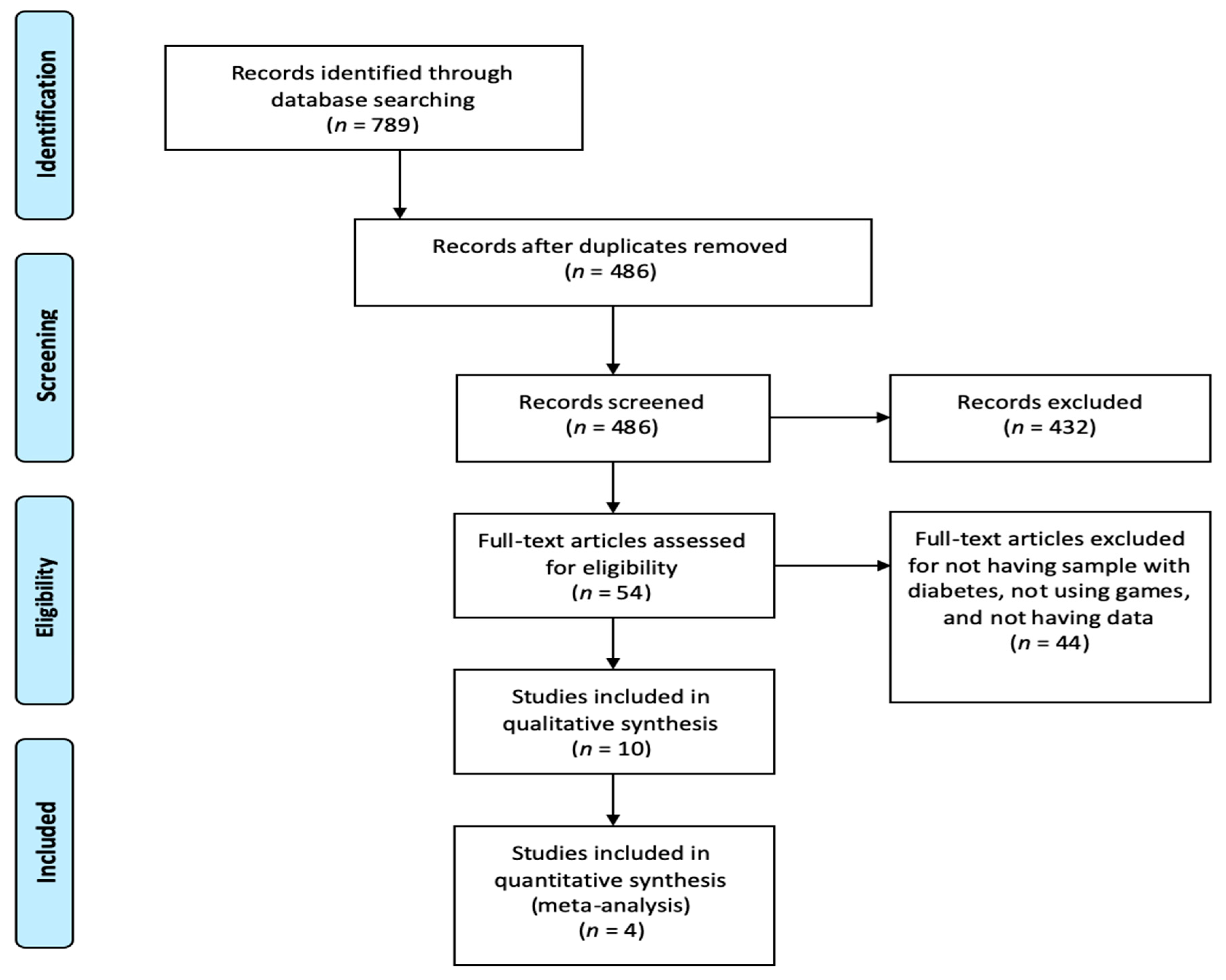
3.1. Study Selection and Study Characteristics
3.2. Electronic and Board Games for Diabetes Knowledge Acquisition
3.3. Electronic Simulation Games for Solving Problems and Situations Related to Diabetes
3.4. Electronic Games for Adherence to Physical Exercise in People with Diabetes
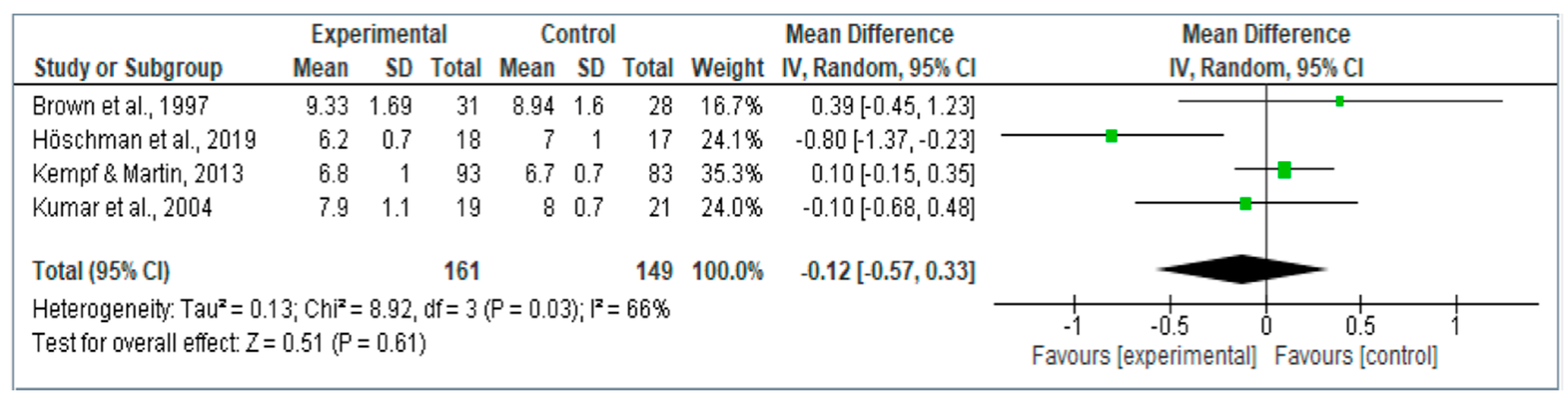
3.5. Meta-Analysis Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Khan, R.M.M.; Chua, Z.J.Y.; Tan, J.C.; Yang, Y.; Liao, Z.; Zhao, Y. From Pre-Diabetes to Diabetes: Diagnosis, Treatments and Translational Research. Medicina. 2019, 55, 546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, Y.; Yang, L.; Shao, F.; Yan, X.; Li, X.; Huang, G.; Xiao, Y.; Zhou, Z. Distinct secretion pattern of serum proinsulin in different types of diabetes. Ann. Transl. Med. 2020, 8, 452. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes. Diabetes Care 2018, 41 (Suppl. 1), S13–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaterjee, S.; Khunti, K.; Davies, M.J. Type 2 diabetes. Lancet 2017, 389, 51–2239. [Google Scholar] [CrossRef]
- Farabi, S.S.; Hernandez, T.L. Low-Carbohydrate Diets for Gestational Diabetes. Nutrients 2019, 11, 1737. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Report on Diabetes. 2016. Available online: https://www.who.int/diabetes/global-report/es/ (accessed on 27 June 2020).
- Ogurtsova, K.; Da Rocha, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, L.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Crandall, J.P.; Polsky, S.; Howard, A.A.; Perreault, L.; Bray, G.A.; Barrett-Connor, E.; Brown-Friday, J.; Whittington, T.; Foo, S.; Ma, Y.; et al. Alcohol consumption and diabetes risk in the diabetes prevention program. Am. J. Clin. Nutr. 2009, 595–601. [Google Scholar] [CrossRef]
- Brown, S.A.; García, A.A.; Brown, A.; Becker, B.J.; Conn, V.S.; Ramírez, G.; Winter, M.A.; Sumplin, L.L.; García, T.J.; Cuevas, H.E. Biobehavioral determinants of glycemic control in type 2 diabetes: A systematic review and meta-analysis. Patient Educ. Couns. 2016, 99, 1558–1567. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Standards of Medical Care in Diabetes. Diabetes Care 2014, 37 (Suppl. 1), S14–S80. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Roberts, S.; Barry, E.; Craig, D.; Airoldi, M.; Bevan, G.; Greenhalgh, T. Preventing type 2 diabetes: Systematic review of studies of cost-effectiveness of lifestyle programmes and metformin, with and without screening, for pre-diabetes. BMJ Open 2017, 7, e017184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudlay, B.; Heiland, B.; Kohler-Raush, E.; Kovic, M. Education and technology used to improve the quality of life for people with diabetes mellitus type II. J. Multidiscip. Health 2014, 7, 47–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamed, N.A.A.; Huassain, A.A.O. Impact of a multidisciplinary intensive education program on type 2 diabetes mellitus patients’ glycemic control and cardiovascular risk factors. Saudi Med. J. 2018, 39, 705–710. [Google Scholar] [CrossRef]
- Thompson, D.; Baranowski, T.; Buday, R. Conceptual Model for the Design of a Serious Video Game Promoting Self-Management among Youth with Type 1 Diabetes. J. Diabetes Sci. Technol. 2010, 4, 744–749. [Google Scholar] [CrossRef] [Green Version]
- Padman, R.; Jaladi, S.; Kim, S.; Kumar, S.; Orbeta, P.; Rudolf, K.; Tran, T. An evaluation framework and a pilot Study of a mobile platform for diabetes self-management: Insights from pediatric users. Stud. Health Technol. Inf. 2013, 192, 333–337. [Google Scholar]
- Sardi, L.; Idri, A.; Fernández-Alemán, J.L. A systematic review of gamification in e-health. J. Biomed. Inf. 2017, 31–48. [Google Scholar] [CrossRef]
- Lazem, S.; Webster, M.; Holmes, W.; Wolf, M. Games and Diabetes: A Review Investigating Theoretical Frameworks, Evaluation Methodologies, and Opportunities for Design Grounded in Learning Theories. J. Diabetes Sci. Technol. 2016, 10, 447–452. [Google Scholar] [CrossRef] [Green Version]
- Dé Cássia, V.; Fels, S.; Castanheira, L. The Value of Children’s Voices for a Video Game Development in the Context of Type 1 Diabetes: Focus Group Study. JMIR Diabetes 2017, 2, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- OCEBM Levels of Evidence Working Group. The Oxford 2011 Levels of Evidence. Oxford Centre for Evidence-Based Medicine. Available online: http://www.cebm.net/wp-content/uploads/2014/06/CEBM-Levels-of-Evidence-2.1.pdf (accessed on 10 April 2020).
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Caffazo, J.A.; Casselman, M.; Hamming, N.; Katzman, D.K.; Palmer, M.R. Design of an mHealth App for the Self-management of Adolescent Type 1 Diabetes: A Pilot Study. J. Med. Internet Res. 2012, 14, 1–70. [Google Scholar] [CrossRef]
- Dugas, M.; Crowley, K.; Gao, G.G.; Xu, T.; Agarwal, R.; Kruglanski, A.W.; Steinle, N. Individual differences in regulatory mode moderate the effectiveness of a pilot mHealth trial for diabetes management among older veterans. PLoS ONE 2018, 13, e019280. [Google Scholar] [CrossRef] [PubMed]
- Kerfoot, B.P.; Gagnon, D.R.; McMahon, G.T.; Orlander, J.D.; Kurgansky, K.E.; Conlin, P.R. A Team-Based Online GameImproves Blood Glucose Control in Veterans with Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Care 2017, 40, 1218–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, V.S.; Wentzell, K.J.; Mikkelsen, T.; Pentland, A.; Laffel, L.M. The DAILY (Daily Automated Intensive Log for Youth) Trial: A Wireless, Portable System to Improve Adherence and Glycemic Control in Youth with Diabetes. Diabetes Technol. Ther. 2004, 6, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Crawford, P.; Wiltz, S. Participation in the Journey to Life Conversation Map Improves Control of Hypertension, Diabetes, and Hypercholesterolemia. J. Am. Board Fam. Med. 2015, 28, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.J.; Lieberman, D.A.; Gemeny, B.A.; Fan, Y.C.; Wilson, D.M.; Pasta, D.J. Educational video game for juvenile diabetes: Results of a controlled trial. Med. Inf. 1997, 22, 77–89. [Google Scholar] [CrossRef]
- Joubert, M.; Armand, C.; Morera, J.; Tokayeva, L.; Guillaume, A.; Reznik, Y. Impact of a Serious Videogame Designed for Flexible Insulin Therapy on the Knowledge and Behaviors of Children with Type 1 Diabetes: The LUDIDIAB Pilot Study. Diabetes Technol. Ther. 2016, 18, 1–7. [Google Scholar] [CrossRef]
- Joshi, R.; Joshi, D.; Cheriyath, P. Improving adherence and outcomes in diabetic patients. Patient Prefer. Adherence 2017, 11, 271–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hochsmann, C.; Muller, O.; Ambuhl, M.; Klenk, C.; Konigstein, K.; Infanger, D.; Walz, S.P.; Schmidt, A. Novel Smartphone Game Improves Physical Activity Behavior in Type 2 Diabetes. Am. J. Prev. Med. 2019, 57, 41–50. [Google Scholar] [CrossRef]
- Kempf, K.; Martin, S. Autonomous exercise game use improves metabolic control and quality of life in type 2 diabetes patients—A randomized controlled trial. BMC Endocr. Disord. 2013, 13, 57. [Google Scholar] [CrossRef] [Green Version]
- Charlier, N.; Zupancic, N.; Fieuws, S.; Denhaerynck, K.; Zaman, B.; Moons, P. Serious games for improving knowledge and self-management in young people with chronic conditions: A systematic review and meta-analysis. J. Am. Med. Inform. Assoc. 2016, 23, 230–239. [Google Scholar] [CrossRef] [Green Version]
- Ebrahimpour, F.; Najafi, M.; Sadeghi, N. The Design and Development of a Computer Game on Insulin Injection. Electron. Physician 2014, 6, 845–855. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, D.; Fraticelli, F.; Polcini, F.; Lato, R.; Pintaudi, B.; Nicolucci, A.; Fulcheri, M.; Mohn, A.; Chiarelli, F.; Di Vieste, G.; et al. Preventing Adolescents’ Diabesity: Design, Development, and First Evaluation of “Gustavo in Gnam’s Planet”. Games Health J. 2015, 4, 344–351. [Google Scholar] [CrossRef] [Green Version]
- Koivisto, J.; Malik, A. Gamification for Older Adults: A Systematic Literature Review. Gerontologist 2020, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.; Feinglos, M.; Pereira, K.; Hassel, N.; Blascovich, J.; Nicollerat, J.; Beresford, H.F.; Levy, J.; Vorderstrasse, A. Feasibility and Preliminary Effects of a Virtual Environment for Adults with Type 2 Diabetes: Pilot Study. JMIR Res. Protoc. 2014, 3, 1–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Marshedi, A.; Wills, G.; Ranchhod, A. Gamifying Self-Management of Chronic Illnesses: A Mixed-Methods Study. JMIR Serious Games 2016, 4, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Markowitz, J.T.; Harrington, K.R.; Laffel, L.M. Technology to Optimize Pediatric Diabetes Management and Outcomes. Curr. Diabetes Rep. 2013, 13. [Google Scholar] [CrossRef] [Green Version]
- Ruggiero, L. Diabetes Prevention and Management: What does a Serious Game Have to Do with It? Games Health J. 2015, 4, 1–2. [Google Scholar] [CrossRef]
- Theng, Y.L.; Lee, J.W.Y.; Patindan, P.V.; Foo, S.S.B. The Use of Videogames, Gamification, and Virtual Environments in the Self-Management of Diabetes: A Systematic Review of Evidence. Games Health J. 2015, 4, 1–10. [Google Scholar] [CrossRef]
- Arthur, L.; Martins, R.; Alejandro, P.; Zonato, R.; Cristina, I. User Assessment of “InsuOnLine” a Game to Fight Clinical Inertia in Diabetes: A Pilot Study. Games Health J. 2015, 4, 335–343. [Google Scholar] [CrossRef]
- Swartwout, E.; El-Zein, A.; Deyo, P.; Sweenie, R.; Streisand, R. Use of Gaming in Self-Management of Diabetes in Teens. Curr. Diabetes Rep. 2016, 16, 59. [Google Scholar] [CrossRef]
- Larkin, A.T.; Hoffman, C.; Stevens, A.; Douglas, A.; Bloomgarden, Z. Determinants of adherence to diabetes treatment. J. Diabetes 2015, 7, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Martos, M.B.; Velando, A.; Pradas, L.; Suleiman, N.; Cañadas, G.A.; Albendín, L.; Gómez, J.L. Smartphones and Apps to Control Glycosylated Hemoglobin (HbA1c) Level in Diabetes: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basiri, R.; Spicer, M.T.; Levenson, C.W.; Ormsbee, M.J.; Ledermann, T.; Arjmandi, B.H. Nutritional Supplementation Concurrent with Nutrition Education Accelerates the Wound Healing Process in Patients with Diabetic Foot Ulcers. Biomedicines 2020, 8, 263. [Google Scholar] [CrossRef]
- Ramadas, A.; Chan, C.K.Y.; Oldenburg, B.; Hussein, Z.; Quek, K.F. Randomised-controlled trial of a web-based dietary intervention for patients with type 2 diabetes: Changes in health cognitions and glycemic control. BMC Public Health 2018, 18, 716. [Google Scholar] [CrossRef] [PubMed]
- Ersotelos, N.; Margioris, A.N.; Zang, X.; Dong, F. Review of mobile applications for optimizing the follow-up care of patients with diabetes. Hormones 2018, 17, 541–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenzuela, T.; Okubo, Y.; Woodbury, A.; Lord, S.R.; Delbaere, K. Adherence to Technology-Based Exercise Programs in Older Adults: A Systematic Review. J. Geriatr. Phys. Ther. 2018, 41, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Halbrook, Y.J.; O’Donnell, A.T.; Msetfi, R.M. When and how video games can be good: A review of the positive effects of video games on well-being. Perspect. Psychol. Sci. 2019, 14, 1096–1104. [Google Scholar] [CrossRef]
- Arnold, J.C. The Importance of Different Knowledge Types in Health-Related Decisions—The Example of Type 2 Diabetes. Sustainability 2020, 12, 3396. [Google Scholar] [CrossRef] [Green Version]
- Maillot, P.; Perrot, A.; Hartley, A.; Do, M.C. The braking force in walking: Age-related differences and improvement in older adults with exergame training. J. Aging Phys. Act. 2014, 22, 518–526. [Google Scholar] [CrossRef]
- Li, J.; Theng, Y.L.; Foo, S. Effect of exergames on depression: A systematic review and meta-analysis. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 34–42. [Google Scholar] [CrossRef]
- Brawley, L.R.; Rejeski, W.J.; King, A.C. Promoting physical activity for older adults. The challenges for changing behavior. Am. J. Prev. Med. 2003, 25, 172–183. [Google Scholar] [CrossRef]
- Keogh, J.W.L.; Power, N.; Wooller, L.; Lucas, P.; Whatman, C. Physical and psychosocial function in residential aged-care elders: Effect of Nintendo Wii Sports games. J. Aging Phys. Act. 2014, 22, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Douris, C.P.; McDonald, C.B.; Vespi, C.F.; Kelley, C.N.; Herman, C.L. Comparison between Nintendo Wii Fit aerobics and traditional aerobic exercise in sedentary young adults. J. Strength Cond. Res. 2012, 26, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- Yardley, L.; Bishop, F.L.; Beyer, N.; Hauer, K.; Kempen, G.; Piot-Ziegler, C.; Todd, C.J.; Cuttelod, T.; Horne, M.; Lanta, K.; et al. Older people’s views of falls-prevention interventions in six European countries. Gerontologist 2006, 46, 650–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, D.; Baranowski, T.; Buday, R.; Baranowski, J.; Thompson, V.; Jago, R.; Griffit, M.J. Serious video games for health how behavioral science guided the development of a serious video game. Simul. Gaming 2010, 41, 587–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |



{kind=link}
{kind=link}
| Search Equation Number | Search Equation Complete String |
|---|---|
| 1 | Diabetes AND (blood glucose OR HbA1c OR Glycated Hemoglobin A) AND (game OR games OR gamification OR virtual reality OR virtual environment OR video game OR video-game OR mobile game OR computer game OR serious game OR serious-games OR serious video- games OR serious games OR serious digital games OR serious electronic games OR serious gaming) |
| 2 | Diabetes AND (game OR games OR gamification OR virtual reality OR virtual environment OR video game OR video-game OR mobile game OR computer game OR serious game OR serious-games OR serious video-games OR serious games OR serious digital games OR serious electronic games OR serious gaming) |
| Author, Country (Year of Publication) | Study Design | Sample | Intervention | Main Results | EL/GR |
|---|---|---|---|---|---|
| Brown et al., USA (1997) [28]. | Randomized controlled trial | n = 59 children (between 8 and 16 years old) with DM1 (28 in the control group and 31 in the intervention group). | Packy and Marlon game for the Super Nintendo. People must face diabetes risk by choosing healthy habits to stay healthy. | After 6 months:
| 1a/A |
| Cafazzo et al., Canada (2012) [23]. | Pilot quasi-experimental study. | n = 20 adolescents (mean age 14.9) with DM1. | A mobile app receives glucometer readings. Points were gained for adhering to best-practice guidelines for blood glucose testing. Points and leveling up was rewarded with Apple Itunes and App Store purchases. | After 12 weeks:
| 3b/B |
| Crawford & Wiltz, USA (2015) [27]. | Case and control stduy | n = 411 people with diabetes (mean age 59.0) | Case group (n = 202 people with DM2). They play “Journey to Life Conversation Map”. Control group (n = 209). Usual care. | Case group HbA1c level decreased from 8.25% to 6.96%. Control group HbA1c level decreased from 8.57 to 8.27. p value between groups differences < than 0.001 | 3b/B |
| Dugas et al., USA (2018) [24]. | Randomized clinical trial | n = 29 people with DM2 (mean age 65.4). (5 in the control group and 24 in the intervention group). | Smartphone app to improve glucose control, exercise, nutrition and medication adherence. Points were given to the patients if the followed healthy habits related with glucose control. | After 13 weeks:
| 1a/A |
| Höschman et al., Switzerland (2019) [31]. | Randomized controlled trial | n = 36 people with DM2 (mean age 57). (18 in the control group and 18 in the intervention group). | Smartphone game following physical activity guidelines to increase physical activity behavior. The use of the game and reaching the activity goals make the person progress in the storyline of the game. | After 24 weeks:
| 1a/A |
| Joshi et al., USA (2017) [30]. | Randomized controlled trial | n = 97 people with DM2. (31 in the control group and 66 in the intervention group). | Game for Ipad with a 12-min duration. The game simulates multiple real-world pressures from job and family for people with diabetes including excuses for non-adherent health habits. The patients have to deal with those situations. | After 3 months:
| 1a/A |
| Joubert et al., France (2016) [29] | Cohorts study | n = 38 children with DM1 (mean age 13.7) | They used a game called “L’Affaire Birman” as an educative tool for insulin therapy. Children must solve the problems of the character (Alex) with his DM1 | After 3 months:
| 2b/B |
| Kempf and Martin, Deutschland (2013) [32]. | Randomized controlled trial | n = 220 people with DM2 (mean age 61). (100 in the control group and 120 in the intervention group). | The intervention group received a Wii console with the game Wii Fit Plus and the balance board. They should use it 30 min a day for 12 weeks. Control group received usual care. | After 12 weeks:
| 1a/A |
| Kerfoot et al., USA (2017) [25]. | Randomized controlled trial | n = 456 people with DM2 (mean age 59). (229 in the control group and 227 in the intervention group). | On-line game about diabetes self-management sends questions via e-mail or app to the patients about diabetes self-management. Points were earned if they answered correctly. The game made groups and individual and team scores were shown on a leaderboard. | After 12 months:
| |
| Kumar et al., USA (2004) [26]. | Randomized controlled trial | n = 40 children (mean age 13.6) (21 in the control group and 19 in the intervention group). | Motivational game through PDA with diabetes management software. Patients were challenged to predict their glucose level and they earned points for being accurate and for playing the game. | After 4 months:
| 1a/A |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martos-Cabrera, M.B.; Membrive-Jiménez, M.J.; Suleiman-Martos, N.; Mota-Romero, E.; Cañadas-De la Fuente, G.A.; Gómez-Urquiza, J.L.; Albendín-García, L. Games and Health Education for Diabetes Control: A Systematic Review with Meta-Analysis. Healthcare 2020, 8, 399. https://doi.org/10.3390/healthcare8040399
Martos-Cabrera MB, Membrive-Jiménez MJ, Suleiman-Martos N, Mota-Romero E, Cañadas-De la Fuente GA, Gómez-Urquiza JL, Albendín-García L. Games and Health Education for Diabetes Control: A Systematic Review with Meta-Analysis. Healthcare. 2020; 8(4):399. https://doi.org/10.3390/healthcare8040399
Chicago/Turabian StyleMartos-Cabrera, María Begoña, María José Membrive-Jiménez, Nora Suleiman-Martos, Emilio Mota-Romero, Guillermo Arturo Cañadas-De la Fuente, José L. Gómez-Urquiza, and Luis Albendín-García. 2020. "Games and Health Education for Diabetes Control: A Systematic Review with Meta-Analysis" Healthcare 8, no. 4: 399. https://doi.org/10.3390/healthcare8040399