The Effect of Muscular Strength on Depression Symptoms in Adults: A Systematic Review and Meta-Analysis

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
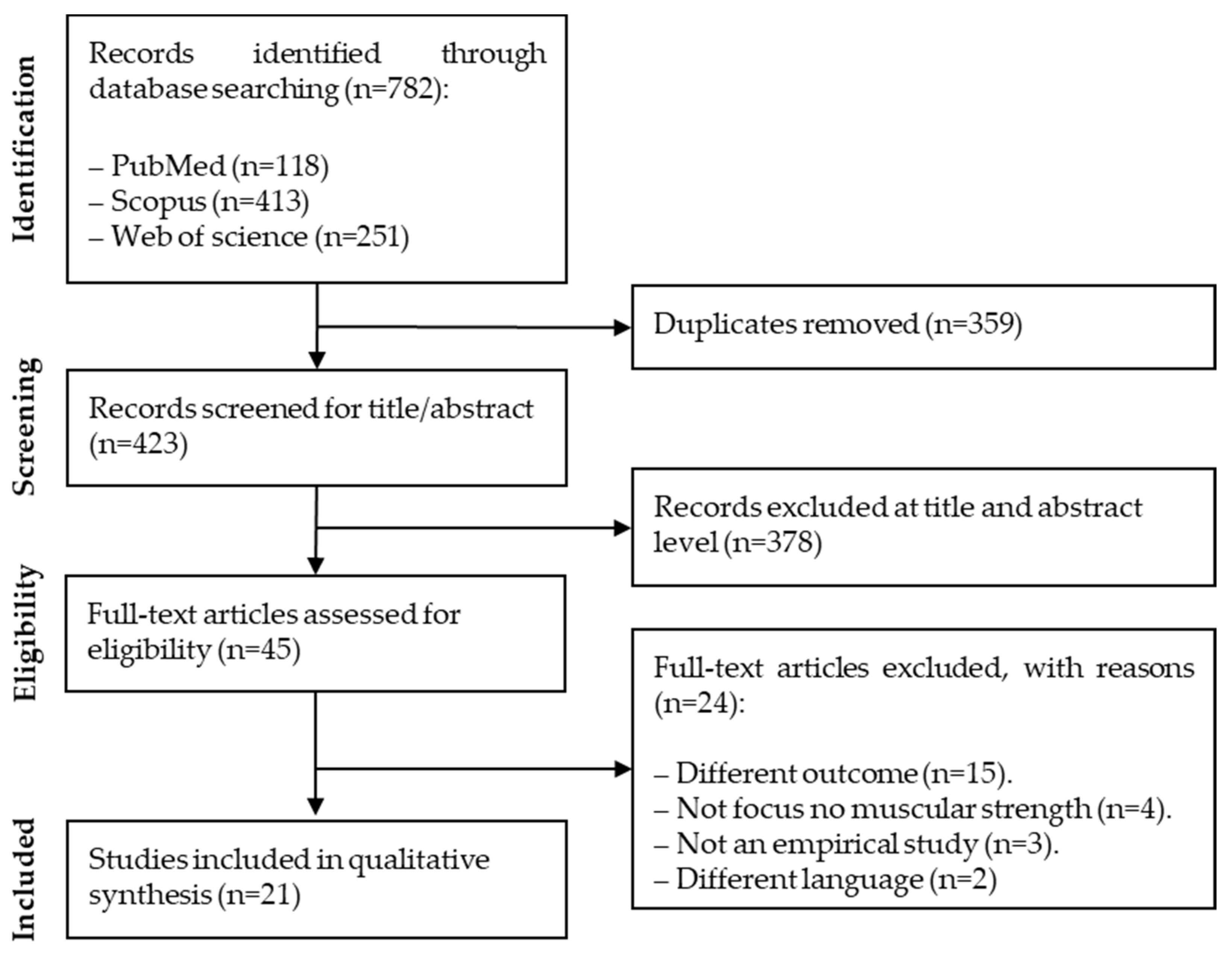
3.1. Literature Search
3.2. Study Characteristics
3.3. Principal Findings
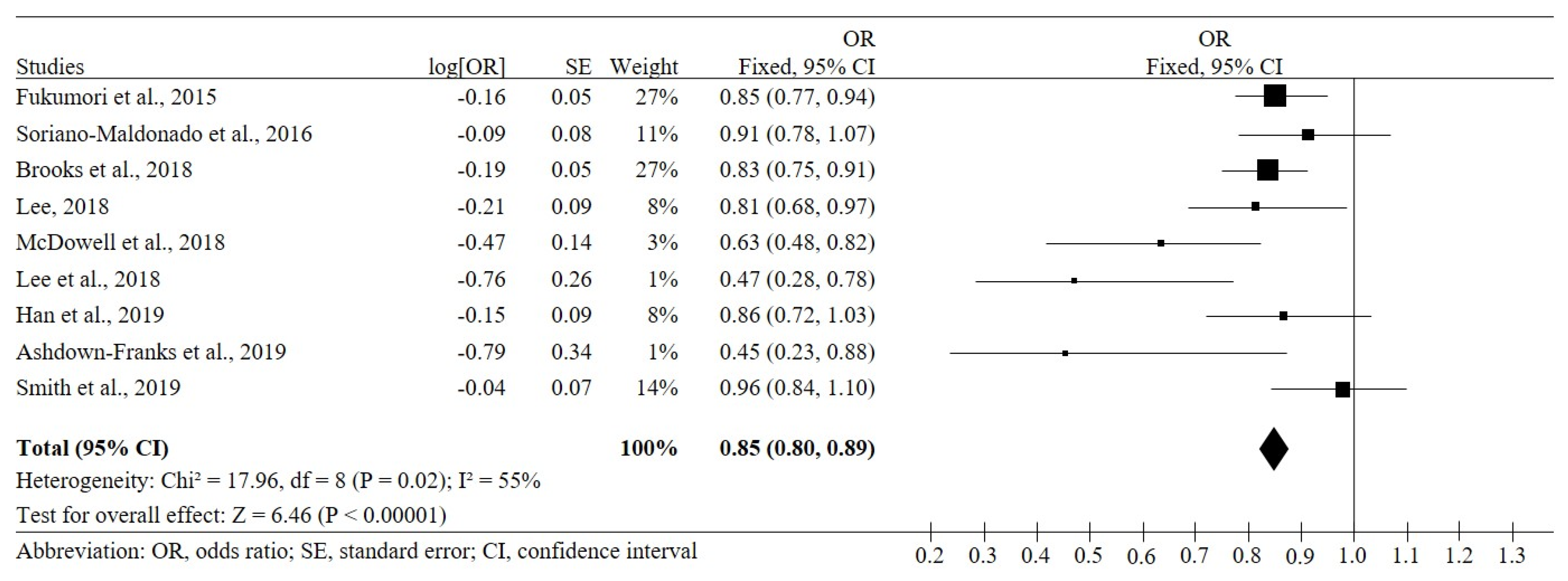
3.4. Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Depression and Other Common Mental Disorders. In Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Karyotaki, E.; Smit, Y.; Holdt Henningsen, K.; Huibers, M.J.; Robays, J.; de Beurs, D.; Cuijpers, P. Combining pharmacotherapy and psychotherapy or monotherapy for major depression? A meta-analysis on the long-term effects. J. Affect. Disord. 2016, 194, 144–152. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.; Faucett, J.; Lichtenberg, P.; Kirsch, I.; Brown, W.A. A systematic review of comparative efficacy of treatments and controls for depression. PLoS ONE 2012, 7, e41778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olfson, M.; Amos, T.B.; Benson, C.; McRae, J.; Marcus, S.C. Prospective service use and health care costs of Medicaid beneficiaries with treatment-resistant depression. J. Manag. Care Spec. Pharm. 2018, 24, 226–236. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [PubMed]
- Lindegard, A.; Wastensson, G.; Hadzibajramovic, E.; Grimby-Ekman, A. Longitudinal associations between cardiorespiratory fitness and stress-related exhaustion, depression, anxiety and sleep disturbances. BMC Public Health 2019, 19, 1726. [Google Scholar] [CrossRef] [Green Version]
- Papasavvas, T.; Bonow, R.O.; Alhashemi, M.; Micklewright, D. Depression symptom severity and cardiorespiratory fitness in healthy and depressed adults: A systematic review and meta-analysis. Sports Med. 2016, 46, 219–230. [Google Scholar] [CrossRef]
- Garcia-Hermoso, A.; Cavero-Redondo, I.; Ramirez-Velez, R.; Ruiz, J.R.; Ortega, F.B.; Lee, D.C.; Martínez-Vizcaíno, V. Muscular strength as a predictor of all-cause mortality in an apparently healthy population: A systematic review and meta-analysis of data from approximately 2 million men and women. Arch. Phys. Med. Rehabil. 2018, 99, 2100–2113 e5. [Google Scholar] [CrossRef]
- Yeung, S.S.Y.; Reijnierse, E.M.; Trappenburg, M.C.; Blauw, G.J.; Meskers, C.G.M.; Maier, A.B. Knee extension strength measurements should be considered as part of the comprehensive geriatric assessment. BMC Geriatr. 2018, 18, 130. [Google Scholar] [CrossRef]
- Bohannon, R.W. Muscle strength: Clinical and prognostic value of hand-grip dynamometry. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef]
- Fukumori, N.; Yamamoto, Y.; Takegami, M.; Yamazaki, S.; Onishi, Y.; Sekiguchi, M.; Otani, K.; Konno, S.; Kikuchi, S.; Fukuhara, S. Association between hand-grip strength and depressive symptoms: Locomotive Syndrome and Health Outcomes in Aizu Cohort Study (LOHAS). Age Ageing 2015, 44, 592–598. [Google Scholar] [CrossRef] [Green Version]
- Stessman, J.; Rottenberg, Y.; Fischer, M.; Hammerman-Rozenberg, A.; Jacobs, J.M. Handgrip Strength in Old and Very Old Adults: Mood, Cognition, Function, and Mortality. J. Am. Geriatr. Soc. 2017, 65, 526–532. [Google Scholar] [CrossRef]
- Gopinath, B.; Kifley, A.; Liew, G.; Mitchell, P. Handgrip strength and its association with functional independence, depressive symptoms and quality of life in older adults. Maturitas 2017, 106, 92–94. [Google Scholar] [CrossRef] [Green Version]
- Veronese, N.; Stubbs, B.; Fontana, L.; Trevisan, C.; Bolzetta, F.; Rui, M.; Sartori, L.; Musacchio, E.; Zambon, S.; Maggi, S.; et al. A comparison of objective physical performance tests and future mortality in the elderly people. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 362–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, O.P.; Hankey, G.J.; Yeap, B.B.; Golledge, J.; Hill, K.D.; Flicker, L. Depression Among Nonfrail Old Men is Associated with Reduced Physical Function and Functional Capacity after 9 Years Follow-up: The Health in Men Cohort Study. J. Am. Med. Dir. Assoc. 2017, 18, 65–69. [Google Scholar] [CrossRef]
- Kvael, L.A.H.; Bergland, A.; Telenius, E.W. Associations between physical function and depression in nursing home residents with mild and moderate dementia: A cross-sectional study. BMJ Open 2017, 7, e016875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- USDHHS. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; US Department of Health and Human Services: Washington, DC, USA, 2018.
- Marques, A.; Peralta, M.; Gouveia, E.R.; Martins, J.; Sarmento, H.; Gomez-Baya, D. Leisure-time physical activity is negatively associated with depression symptoms independently of the socioeconomic status. Eur. J. Sport Sci. 2019, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; Gaspar de Matos, M.; Bordado, J.; Gouveia, E.R.; Peralta, M.; Gomez-Baya, D. Different levels of physical activity and depression symptoms among older adults from 18 countries: A population-based study from the Survey of Health, Ageing and Retirement in Europe (SHARE). Eur. J. Sport Sci. 2020, 1–8. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Ashdown-Franks, G.; Stubbs, B.; Koyanagi, A.; Schuch, F.; Firth, J.; Veronese, N.; Vancampfort, D. Handgrip strength and depression among 34,129 adults aged 50 years and older in six low- and middle-income countries. J. Affect. Disord. 2019, 243, 448–454. [Google Scholar] [CrossRef] [Green Version]
- Brooks, J.M.; Titus, A.J.; Bruce, M.L.; Orzechowski, N.M.; Mackenzie, T.A.; Bartels, S.J.; Batsis, J.A. Depression and handgrip strength among U.S. adults aged 60 years and older from NHANES 2011–2014. J. Nutr. Health Aging 2018, 22, 938–943. [Google Scholar] [CrossRef]
- Han, K.M.; Chang, J.; Yoon, H.K.; Ko, Y.H.; Ham, B.J.; Kim, Y.K.; Han, C. Relationships between hand-grip strength, socioeconomic status, and depressive symptoms in community-dwelling older adults. J. Affect. Disord. 2019, 252, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Lee, K. Relative handgrip strength in relation to depressive mood and suicidal ideation in Koreans using the 2015 KNHANES data. J. Musculoskelet. Neuronal. Interact. 2018, 18, 333–338. [Google Scholar]
- Lee, M.R.; Jung, S.M.; Bang, H.; Kim, H.S.; Kim, Y.B. The association between muscular strength and depression in Korean adults: A cross-sectional analysis of the sixth Korea National Health and Nutrition Examination Survey (KNHANES VI) 2014. BMC Public Health 2018, 18, 1123. [Google Scholar] [CrossRef] [Green Version]
- McDowell, C.P.; Gordon, B.R.; Herring, M.P. Sex-related differences in the association between grip strength and depression: Results from the Irish Longitudinal Study on Ageing. Exp. Gerontol. 2018, 104, 147–152. [Google Scholar] [CrossRef]
- Smith, L.; Firth, J.; Grabovac, I.; Koyanagi, A.; Veronese, N.; Stubbs, B.; Soysal, P.; Yang, L.; Jackson, S.E. The association of grip strength with depressive symptoms and cortisol in hair: A cross-sectional study of older adults. Scand. J. Med. Sci. Sports 2019, 29, 1604–1609. [Google Scholar] [CrossRef]
- Soriano-Maldonado, A.; Estévez-López, F.; Segura-Jiménez, V.; Aparicio, V.A.; Álvarez-Gallardo, I.C.; Herrador-Colmenero, M.; Jonatan R Ruiz, M.H.; Henriksen, M.; Amris, K.; Delgado-Fernández, M.; et al. Association of physical fitness with depression in women with fibromyalgia. Pain Med. 2016, 17, 1542–1552. [Google Scholar] [CrossRef] [Green Version]
- Laredo-Aguilera, J.A.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I.; Garcia-Pinillos, F.; Latorre-Roman, P.A. Handgrip strength is associated with psychological functioning, mood and sleep in women over 65 years. Int. J. Environ. Res. Public Health 2019, 16, 873. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Cho, J.; Kim, D.; Jin, Y.; Lee, I.; Hong, H.; Kang, H. Handgrip strength, depression, and all-cause mortality in Korean older adults. BMC Geriatr. 2019, 19, 127. [Google Scholar] [CrossRef]
- Wu, H.; Yu, B.; Meng, G.; Liu, F.; Guo, Q.; Wang, J.; Du, H.; Zhang, W.; Shen, S.; Han, P.; et al. Both muscle mass and muscle strength are inversely associated with depressive symptoms in an elderly Chinese population. Int. J. Geriatr. Psychiatry 2017, 32, 769–778. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S.; O’Sullivan, D.M.; Shin, S.K. Can 24weeks strength training reduce feelings of depression and increase neurotransmitter in elderly females? Exp. Gerontol. 2019, 115, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Krogh, J.; Saltin, B.; Gluud, C.; Nordentoft, M. The DEMO trial: A randomized, parallel-group, observer-blinded clinical trial of strength versus aerobic versus relaxation training for patients with mild to moderate depression. J. Clin. Psychiatry 2009, 70, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Aidar, F.J.; de Matos, D.G.; de Oliveira, R.J.; Carneiro, A.L.; Cabral, B.; Dantas, P.M.S.; Reis, V.M. Relationship between depression and strength training in survivors of the ischemic stroke. J. Hum. Kinet. 2014, 43, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Moraes, H.S.; Silveira, H.S.; Oliveira, N.A.; Matta Mello Portugal, E.; Araujo, N.B.; Vasques, P.E.; Bergland, A.; Santos, T.M.; · Engedal, K.; · Coutinho, E.S.; et al. Is strength training as effective as aerobic training for depression in older adults? A randomized controlled trial. Neuropsychobiology 2020, 79, 141–149. [Google Scholar] [CrossRef]
- Sener, U.; Ucok, K.; Ulasli, A.M.; Genc, A.; Karabacak, H.; Coban, N.F.; Simsek, H.; Cevik, H. Evaluation of health-related physical fitness parameters and association analysis with depression, anxiety, and quality of life in patients with fibromyalgia. Int. J. Rheum. Dis. 2016, 19, 763–772. [Google Scholar] [CrossRef]
- Smith, L.; White, S.; Stubbs, B.; Hu, L.; Veronese, N.; Vancampfort, D.; Hamer, M.; Gardner, B.; Yang, L. Depressive symptoms, handgrip strength, and weight status in US older adults. J. Affect. Disord. 2018, 238, 305–310. [Google Scholar] [CrossRef]
- Suija, K.; Timonen, M.; Suviola, M.; Jokelainen, J.; Jarvelin, M.R.; Tammelin, T. The association between physical fitness and depressive symptoms among young adults: Results of the Northern Finland 1966 birth cohort study. BMC Public Health 2013, 13, 535. [Google Scholar] [CrossRef] [Green Version]
- Vancampfort, D.; Probst, M.; Scheewe, T.; De Herdt, A.; Sweers, K.; Knapen, J.; van Winkel, R.; de Hert, M. Relationships between physical fitness, physical activity, smoking and metabolic and mental health parameters in people with schizophrenia. Psychiatry Res. 2013, 207, 25–32. [Google Scholar] [CrossRef]
- Vancampfort, D.; Correll, C.U.; Galling, B.; Probst, M.; De Hert, M.; Ward, P.B.; Rosenbaum, S.; Gaughran, F.; Lally, J.; Stubbs, B. Diabetes mellitus in people with schizophrenia, bipolar disorder and major depressive disorder: A systematic review and large scale meta-analysis. World Psychiatry 2016, 15, 166–174. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, A.J.; Charlson, F.J.; Norman, R.E.; Patten, S.B.; Freedman, G.; Murray, C.J.; Vos, T.; Whiteford, H.A. Burden of depressive disorders by country, sex, age, and year: Findings from the global burden of disease study 2010. PLoS Med. 2013, 10, e1001547. [Google Scholar] [CrossRef] [Green Version]
- Walker, E.R.; McGee, R.E.; Druss, B.G. Mortality in mental disorders and global disease burden implications: A systematic review and meta-analysis. JAMA Psychiatry 2015, 72, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Silventoinen, K.; Magnusson, P.K.; Tynelius, P.; Batty, G.D.; Rasmussen, F. Association of body size and muscle strength with incidence of coronary heart disease and cerebrovascular diseases: A population-based cohort study of one million Swedish men. Int. J. Epidemiol. 2009, 38, 110–118. [Google Scholar] [CrossRef] [Green Version]
- Fraser, B.J.; Huynh, Q.L.; Schmidt, M.D.; Dwyer, T.; Venn, A.J.; Magnussen, C.G. Childhood Muscular Fitness Phenotypes and Adult Metabolic Syndrome. Med. Sci. Sports Exerc. 2016, 48, 1715–1722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manini, T.M.; Clark, B.C. Dynapenia and aging: An update. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 28–40. [Google Scholar] [CrossRef] [Green Version]
- McGrath, R.; Robinson-Lane, S.G.; Peterson, M.D.; Bailey, R.R.; Vincent, B.M. Muscle Strength and Functional Limitations: Preserving Function in Older Mexican Americans. J. Am. Med. Dir. Assoc. 2018, 19, 391–398. [Google Scholar] [CrossRef]
- Takahashi, T.; Sugie, M.; Nara, M.; Koyama, T.; Obuchi, S.P.; Harada, K.; Kyo, S.; Ito, H. Femoral muscle mass relates to physical frailty components in community-dwelling older people. Geriatr. Gerontol. Int. 2017, 17, 1636–1641. [Google Scholar] [CrossRef]
- Liu C-j Shiroy, D.M.; Jones, L.Y.; Clark, D.O. Systematic review of functional training on muscle strength, physical functioning, and activities of daily living in older adults. Eur. Rev. Aging Phys. Act. 2014, 11, 95–106. [Google Scholar]
- Vest, M.T.; Murphy, T.E.; Araujo, K.L.; Pisani, M.A. Disability in activities of daily living, depression, and quality of life among older medical ICU survivors: A prospective cohort study. Health Qual. Life Outcomes 2011, 9, 9. [Google Scholar] [CrossRef] [Green Version]
- Haynie, D.A.; Berg, S.; Johansson, B.; Gatz, M.; Zarit, S.H. Symptoms of depression in the oldest old: A longitudinal study. J. Gerontol. B Psychol. Sci. Soc. Sci. 2001, 56, P111–P118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musalek, C.; Kirchengast, S. Grip Strength as an Indicator of Health-Related Quality of Life in Old Age-A Pilot Study. Int. J. Environ. Res. Public Health 2017, 14, 1447. [Google Scholar] [CrossRef] [Green Version]
- Kohler, C.A.; Freitas, T.H.; Maes, M.; de Andrade, N.Q.; Liu, C.S.; Fernandes, B.S.; Stubbs, B.; Solmi, M.; Veronese, N.; Herrmann, N.; et al. Peripheral cytokine and chemokine alterations in depression: A meta-analysis of 82 studies. Acta Psychiatr. Scand. 2017, 135, 373–387. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Veronese, N.; Thompson, T.; Kahl, K.G.; Fernandes, B.S.; Prina, A.M.; Solmi, M.; Schofield, P.; Koyanagi, A.; Tseng, P.; et al. Relationship between depression and frailty in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2017, 36, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.N.; Choi, K.M. Sarcopenia: Definition, epidemiology, and pathophysiology. J. Bone Metab. 2013, 20, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steptoe, A.; Demakakos, P.; de Oliveira, C.; Wardle, J. Distinctive biological correlates of positive psychological well-being in older men and women. Psychosom. Med. 2012, 74, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Kaminsky, L.A.; Arena, R.; Beckie, T.M.; Brubaker, P.H.; Church, T.S.; Forman, D.E.; Franklin, B.A.; Martha, G.; Lavie, C.J.; Myers, J.; et al. The importance of cardiorespiratory fitness in the United States: The need for a national registry: A policy statement from the American Heart Association. Circulation 2013, 127, 652–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsen, P.O.; Termannsen, A.D.; Bramming, M.; Tully, M.A.; Caserotti, P. Effects of resistance training on self-reported disability in older adults with functional limitations or disability—A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2019, 16, 24. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Author, Year | Study Design | Country and Sample’s Characteristics | Depression Measure | Muscular Strength Measure | Main Results | Study Quality |
|---|---|---|---|---|---|---|
| Krogh et al., 2009 | Clinical trial | Denmark n = 165, 122 women, age range = 18–55, mean age 38.9 ± 9.46; strength training (n = 55); aerobic training (n = 55); relaxation training (n = 55). | Hamilton Depression Rating Scale (HAM-D17) | Knee extension; Chest press; Leg press | (Ø) At 4 months, the mean change in the HAM-D17 score was –1.3 (−3.7–1.2; p = 0.3) for the strength group vs. the relaxation group. At 12 months, the mean differences in the HAM-D17 score were −0.2 (−2.7–2.3) for the strength group vs. the relaxation group. Findings do not support a biologically mediated effect of strength exercise on symptom severity in depressed patients. | Strong |
| Suija et al., 2013 | Prospective | Finland n = 5497, 51% women, age = 31 (all participants were born in 1966). | Hopkins’ Symptom Checklist (HSCL-25) | Trunk extension test; Hand dynamometer | (+) Depressive symptoms were most common among males and females in the lowest quintile group of the trunk extension test and among the males in the lowest quintile group of the handgrip strength compared to the middle quintile group. | Strong |
| Vancampfort et al., 2013 | Cross-sectional | Belgium n = 120; schizophrenia: n = 80, mean age 36.8 ± 10.0; control: n = 40, mean age 37.1 ± 10.3. | Psychosis Evaluation Tool for Common use by Caregivers (PECC) | Standing broad jump; Sit-ups; Handgrip strength | (+) Standing broad jump (−0.35, p < 0.01), handgrip strength (−0.28, p < 0.01) and sit-ups (−0.33, p < 0.01) were inversely associated to depressive symptoms. Low physical fitness was associated with depressive symptoms. | Moderate |
| Aidar et al., 2014 | Clinical trial | Brazil Control group: n = 24, 6 men, mean age = 51.7 ± 0.8 Experimental group: n = 13, 9 men, mean age = 52.5 ± 7.7. | Beck Depression Inventory (BDI) | Squat; Bench press; Horizontal leg press; Military press; Abdominal crunch; Front lat pull-downs; Lunges | (+) There were significant differences in all indicators of depression between the experimental group and the control group after completing 12 weeks of training. A negative correlation between the strength gains as determined with the one-repetition maximum test and the levels of depression was found. | Weak |
| Fukumori, 2015 | Prospective | Japan n = 4314, 58.5% women, age range 40–79, mean age 66.3 ± 9.0. | Mental Health Inventory (MHI-5) | Digital dynamometer (Takei Scientific Instruments Co., Ltd.) | (+) Men and women with lower handgrip strength had higher odds of having depressive symptoms at baseline. Lower handgrip strength was associated with the longitudinal development of depressive symptoms after 1 year (odds ratio (OR) = 1.13, 95%CI = 1.01, 1.27). | Strong |
| Sener et al., 2016 | Clinical trial | Turkey n = 79; experimental group: n = 39 women with fibromyalgia; mean age 42 ± 10.3 years; control group: n = 40 women; mean age 38.3 ± 8.4 years. | Beck Depression Inventory (BDI) | Digital Grip Dynamometer (T.K.K.5401) | (+) In the fibromyalgia group, right and left handgrip strength were moderately negatively correlated with depression scores (r = 0.263 p = 0.025; r = 0.233 p = 0.048). Low muscle strength increased depression and anxiety symptomatology in patients with fibromyalgia. | Moderate |
| Soriano-Maldonado et al., 2016 | Cross-sectional | Spain n = 444 were included in the analysis; mean age 52.0 ± 8.0 years. | Beck Depression Inventory II (BDI II) | Digital Grip Dynamometer (T.K.K. 5101) | (+) The odds of severe symptoms of depression were 4.8% (95% CI: 8.2% to 1.2%; p = 0.010) lower for each additional kilogram in the handgrip test among women with fibromyalgia. | Weak |
| Gopinath et al., 2017 | Cross-sectional | Australia n = 947 men and women; aged ≥65 years. | Center for Epidemiologic Studies Depression Scale (CES-D-10) | Jamar hand dynamometer (Sammons Preston Inc.) | (Ø) Handgrip strength was not associated with depressive symptoms and quality of life. | Weak |
| Wu et al., 2017 | Cross-sectional | China n = 1046, 486 men, 560 women, aged ≥60. | Geriatric Depression Scale (GDS) | Dynamometer (EH101; CAMRY, Guangdong) | (+) Men and women in the lower quartile for muscle strength had a significantly higher risk for depressive symptoms compared with those in the fourth quartile. Muscle strength are inversely associated with depressive symptoms in elderly Chinese. | Weak |
| Brooks et al., 2018 | Cross-sectional | USA n = 3421 community-dwelling, non-institutionalized adults; 1660 men, 1761 women; aged ≥60 years, mean age was 69.9 ± 6.9 years. | Patient Health Questionnaire (PHQ-9) | Dynamometer | (+) Depression was significantly associated with reduced handgrip strength in older adults. | Weak |
| Lee, 2018 | Cross-sectional | South Korea n = 4810, 2167 men, 2643 women; mean age 50.9 ± 16.7 years. | Depressive mood was assessed using one question: ‘During the past year, did you ever feel so sad or hopeless for 2 weeks or more in a row that you stopped performing usual activities? | Digital Grip Dynamometer (T.K.K.5401) | (+) Handgrip strength was negatively associated with depressive mood (OR = 0.82, 95% CI: 0.69–0.99) and suicidal ideation (OR = 0.73, 95% CI: 0.54–0.99). In a sex-specific relationship, handgrip strength was negatively associated with depressive mood and suicidal ideation among women (OR = 0.71, 95% CI: 0.55–0.93) but not men. | Moderate |
| Lee et al., 2018 | Cross-sectional | South Korea n = 4298, 1860 men, 2438 women; age range (19–80 years); subjects were divided into three groups (young adult (19–39 years), middle aged (40–59 years), and elderly (60–80 years). | Patient Health Questionnaire (PHQ-9) | Digital Grip Dynamometer (T.K.K.5401) | (+) Handgrip strength was inversely associated with the PHQ-9 score. The odds ratios of depression symptoms were statistically significant for the participants in the first and second quartile of handgrip strength compared to those with the highest quartile. There was about a 50% mediation effect of EQ5D in the relationship between handgrip strength and depression. | Moderate |
| McDowell et al., 2018 | Prospective | Ireland n = 4505, 2544 men, 1961 women; aged ≥50 years. | EuroQol Five-Dimension Questionnaire (EQ5D) | Baseline hydraulic dynamometer | (+) In the total sample, the middle- and high-strength tertiles were significantly associated with 31.5% (p = 0.04) and 34.1% (p = 0.02) reduced odds of developing depression, respectively. The interaction between sex and strength was not statistically significant. | Strong |
| Smith et al., 2018 | Cross-sectional | USA n = 2812, 1380 men, 1432 women, mean age 68.9 ± 0.3 and 69.5 ± 0.3 | Center for Epidemiological Studies Depression Scale (CES-D) | Takei Digital Grip Strength Dynamometer | (+) Women with moderate to major depressive symptoms had 1.60 kg (95% CI: 0.91 to 2.30) lower handgrip strength compared to women with minimal or no depressive symptoms. No association was observed in men. Obese men (-3.72 kg, 95% CI:−7.00, −0.43) and women (−1.83 kg, 95% CI:−2.87, −0.78) with moderate to severe depressive symptoms had lower handgrip strength. | Moderate |
| Ashdown-Franks et al., 2019 | Cross-sectional | China, Ghana, India Mexico, Russia, South Africa n = 34,129, China 13,175, Ghana 4305, India 6560, Mexico 2313, Russia 3938, South Africa 3838; mean age 62.4 ± 16 years | Patient Health Questionnaire (PHQ-9) | Smedley Handgrip Dynamometer | (+) Individuals with weak handgrip strength had a higher prevalence of depression than those without (8.8% vs. 3.8%; p < 0.001). In all countries, weak handgrip strength was associated with a 1.45 (95% CI:1.12–1.88) times higher odds for depression, although some between country differences were noted (particularly in Ghana). Age and sex-stratified analysis showed similar results. | Strong |
| Han et al., 2019 | Cross-sectional | South Korea n = 3169, 1451 men, 1718 women; aged 59–69 years, mean age 55 ± 6.25 years. | Patient Health Questionnaire (PHQ-9) | Digital Grip Dynamometer (T.K.K.5401) | (+) Older adults in the lowest tertile of handgrip strength measures were more likely to have experienced depressive symptoms compared to those in the highest tertile. | Moderate |
| Kim et al., 2019 | Clinical trial | South Korea n = 21 women, aged 67–81 years, mean age 76.40 ± 3.27 years; control group (n = 10; mean age 76.40 ± 3.27 years) and intervention group (n = 11, mean age 76.10 ± 3.85 years). | Korean version of the Short form of the Geriatric Depression Scale (SGDS-K) | The exercise program was 3 times/week for 24 weeks. Part I from 1–4 weeks, Part II from 5–8 weeks, Part III from 9–15 weeks, and advanced long-term training from 16 to 24 weeks. The exercise program consists of warm-up (for 10 min), main exercise (for 30–60 min) and warm-down (for 10 min). | (Ø) In neurotransmitter factor, serotonin, dopamine, epinephrine, and norepinephrine were significantly decreased in the strength exercise group but not for the control group. There were no significant differences for both the strength exercise group and control group. | Weak |
| Laredo-Aguilera et al., 2019 | Cross-sectional | Spain n = 38 active women, aged >65 years, mean age 72.29 ± 5.21 years. | Spanish version of the Short form of the Geriatric Depression Scale (SGDS-S) | Digital Grip Dynamometer (T.K.K. 5101) | (+) The group with a higher handgrip strength result had a better total score for depression. Significant and negative correlations were found between the handgrip strength and depression. | Weak |
| Moraes et al., 2019 | Clinical trial | Brazil n = 27 older adults with major depressive disorder; aerobic training (n = 9, 1 man and 8 women, aged 60–78; 70.88 ± 5.94 years), strength training (n = 9, 8 men, 1 woman, aged 60–81; 72.89 ± 7.06 years), control group (n = 7, 2 men and 5 women, aged 61–77; 69.28 ± 5.28 years). | Hamilton Depression Rating Scale (HAM-D), and Beck Depression Inventory (BDI) | The 1-repetition maximum test was applied. The scale of perception of effort from 6 to 20 was used to quantify the subject’s effort during activity. | (+) The aerobic training and strength training intervention groups showed significant reductions in depressive symptoms from pre to post intervention when compared to the control group. | Moderate |
| Park et al., 2019 | Prospective | South Korea n = 13,901, 5996 men, 7905 women; aged > 60 year, mean age 69.54 ± 7.06 years. | Korean version of the Short form of the Geriatric Depression Scale (SGDS-K) | Handgrip Dynamometer (TANITA No. 6103, Tokyo) | (+) Individuals with depression only and individuals with low handgrip strength plus depression had significantly higher risks of all-cause mortality. Men and women with higher handgrip strength had significantly lower depression scores. | Strong |
| Smith et al., 2019 | Cross-sectional | United Kingdom n = 3741 community-dwelling, 1257 men, 2484 women; aged 54–89 years, mean age 68.4 years. | Center for Epidemiologic Studies Depression scale (CES-D8) | Hand-held dynamometer | (+) Grip strength was negatively associated with depressive symptoms, when the analysis was adjusted for sex and age. When fully adjusted, the association remained significant but was weaker. | Strong |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marques, A.; Gomez-Baya, D.; Peralta, M.; Frasquilho, D.; Santos, T.; Martins, J.; Ferrari, G.; Gaspar de Matos, M. The Effect of Muscular Strength on Depression Symptoms in Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 5674. https://doi.org/10.3390/ijerph17165674
Marques A, Gomez-Baya D, Peralta M, Frasquilho D, Santos T, Martins J, Ferrari G, Gaspar de Matos M. The Effect of Muscular Strength on Depression Symptoms in Adults: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(16):5674. https://doi.org/10.3390/ijerph17165674
Chicago/Turabian StyleMarques, Adilson, Diego Gomez-Baya, Miguel Peralta, Diana Frasquilho, Teresa Santos, João Martins, Gerson Ferrari, and Margarida Gaspar de Matos. 2020. "The Effect of Muscular Strength on Depression Symptoms in Adults: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 16: 5674. https://doi.org/10.3390/ijerph17165674