
Key Factors Associated with Adherence to Physical Exercise in Patients with Chronic Diseases and Older Adults: An Umbrella Review

 , , ,
, , ,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection of Studies
2.2. Data Extraction
2.3. Data Synthesis
- Characteristics of the exercise program, that would comprise those factors related to how the physical exercise is planned, including the individualization, the evidence-based settings, and other characteristics such as frequency, duration, intensity, or volume.
- Involvement of professionals from different disciplines, that would be related to the convenience of including experts or methods from different disciplines.
- Supervision, which would include the significance or irrelevance of supervising the exercise interventions.
- Technology, which would be focused on the potential additional benefits or disadvantages of including technological devices and applications to conduct the physical exercise intervention.
- Initial exploration of participant’s characteristics, barriers, and facilitators, which would include the identification of relevant variables of the patients before the exercise interventions that could reduce or increase the adherence to exercise.
- Participants’ education, adequate expectations, and knowledge about risks and benefits, which would be related to what the participants know or learn about the relevance of physical exercise for their own health so that the expectations about the improvements were not inaccurate.
- Enjoyment and absence of unpleasant experiences, which would be related to the pleasure obtained while exercising and also by the absence of pain or discomfort.
- Integration in daily living, which includes the consideration of the participant’s preferences and background to adapt the exercise characteristics and settings.
- Social support and relatedness, which includes support from peers, staff, and family, as well as the establishment of positive social interactions and feelings of belonging to a group.
- Communication and feedback, which is related to the effective interaction between the staff and the participant.
- Available progress information and monitoring, providing enough information to the patient so that they can be aware of the changes and improvements from objective data.
- Self-efficacy and competence, which is related to the participant’s perception of what they can do and what they will be able to do.
- Participant’s active role, which would include self-management, self-control, self-monitoring, autonomy, and empowerment.
- Goal setting, which is related to the establishment of adequate objectives.
3. Results
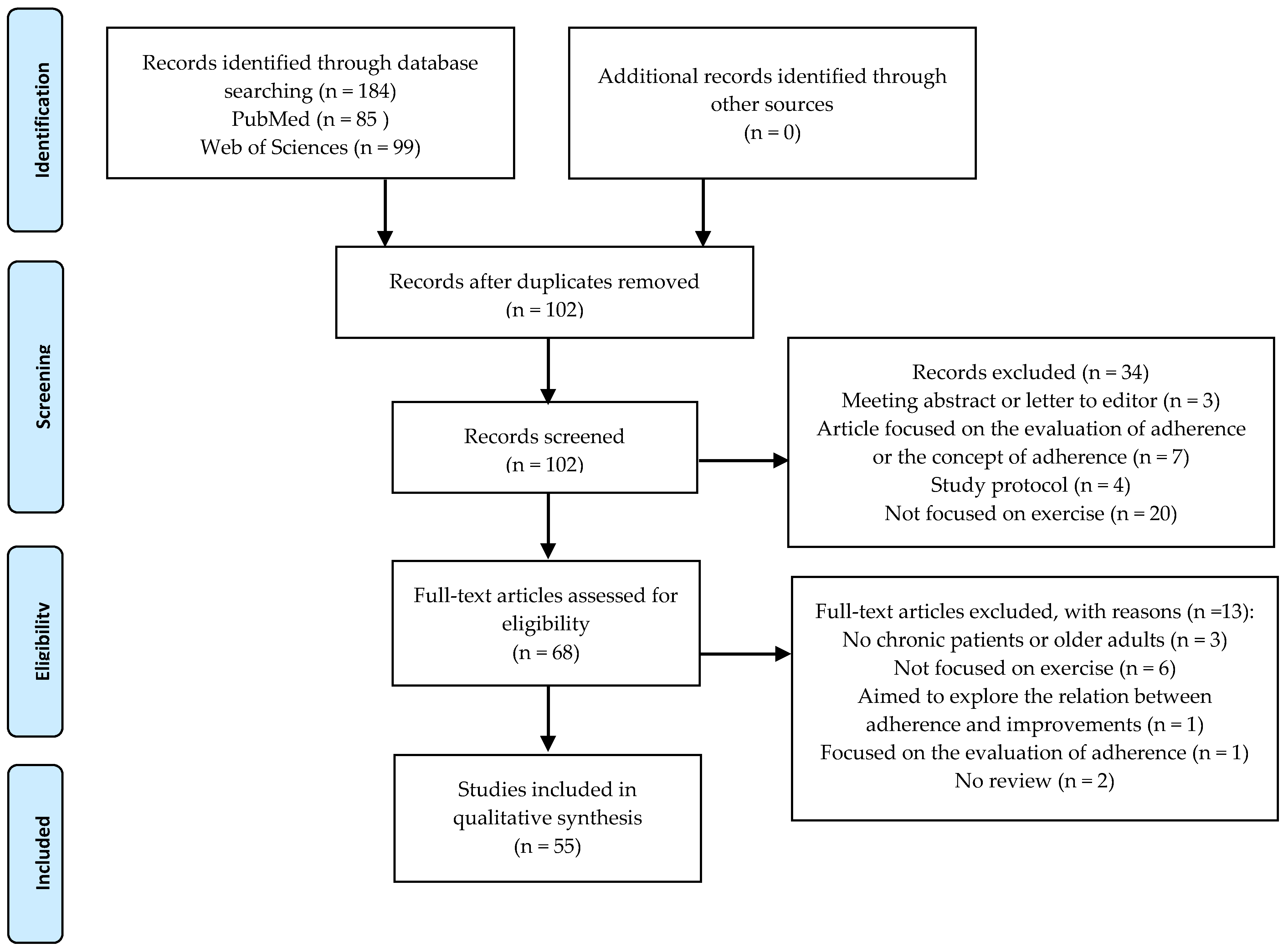
3.1. Study Selection
3.2. Study Characteristics
3.3. Outcome Results
4. Discussion
4.1. Design of the Exercise Intervention
4.2. Multidisciplinary Team
4.3. Supervision during the Exercise Sessions
4.4. The Use of Technology
4.5. Initial Exploration of Participant’s Characteristics, Barriers, and Facilitators
4.6. Participants Education, Adequate Expectations, and Knowledge about Risks and Benefits
4.7. Enjoyment and Absence of Unpleasant Experiences
4.8. Integration in Daily Living
4.9. Social Support and Relatedness
4.10. Communication and Feedback
4.11. Available Progress Information and Monitoring
4.12. Self-Efficacy and Competence
4.13. Participant’s Active Role
4.14. Goal Setting
4.15. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Desa, U. World Population Prospects 2019: Highlights; United Nations Department for Economic and Social Affairs: New York, NY, USA, 2019. [Google Scholar]
- Hajat, C.; Stein, E. The global burden of multiple chronic conditions: A narrative review. Prev. Med. Rep. 2018, 12, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. S3), 1–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary behavior, exercise, and cardiovascular health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef]
- WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour: At a Glance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Blair, S.; Sallis, R.; Hutber, A.; Archer, E. Exercise therapy—The public health message. Scand. J. Med. Sci. Sports 2012, 22, e24–e28. [Google Scholar] [CrossRef]
- Thomas, M.M.; Phongsavan, P.; McGill, B.; O’Hara, B.J.; Bauman, A.E. A review of the impact of physical activity mass media campaigns on low compared to high socioeconomic groups. Health Educ. Res. 2018, 33, 429–446. [Google Scholar] [CrossRef]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef] [Green Version]
- Rodulfo, J.I.A. Sedentarism, a disease from xxi century. Clínica Investig. Arterioscler. 2019, 31, 233–240. [Google Scholar] [CrossRef]
- Johnston, C.A.; Moreno, J.P.; Hernandez, D.C.; Link, B.A.; Chen, T.-A.; Wojtanowski, A.C.; Foster, G.D.; Foreyt, J.P. Levels of adherence needed to achieve significant weight loss. Int. J. Obes. 2018, 43, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Beaudry, R.; Kruger, C.; Liang, Y.; Parliament, M.; Haykowsky, M.; McNeely, M. Effect of super-vised exercise on aerobic capacity in cancer survivors: Adherence and workload predict variance in effect. World J. Meta-Anal. 2015, 3, 43–53. [Google Scholar] [CrossRef]
- Jansons, P.S.; Haines, T.P.; O’Brien, L. Interventions to achieve ongoing exercise adherence for adults with chronic health conditions who have completed a supervised exercise program: Systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 465–477. [Google Scholar] [CrossRef]
- Allen, N.E.; Sherrington, C.; Suriyarachchi, G.D.; Paul, S.S.; Song, J.; Canning, C.G. Exercise and motor training in people with Parkinson’s disease: A systematic review of participant characteristics, intervention delivery, retention rates, adherence, and adverse events in clinical trials. Parkinson’s Dis. 2012, 2012, 854328. [Google Scholar] [CrossRef] [PubMed]
- Sheill, G.; Guinan, E.; Brady, L.; Hevey, D.; Hussey, J. Exercise interventions for patients with advanced cancer: A systematic review of recruitment, attrition, and exercise adherence rates. Palliat. Support. Care 2019, 17, 686–696. [Google Scholar] [CrossRef] [PubMed]
- Wallen, M.P.; Skinner, T.L.; Pavey, T.G.; Hall, A.; Macdonald, G.A.; Coombes, J.S. Safety, adherence and efficacy of exercise training in solid-organ transplant candidates: A systematic review. Transplant. Rev. 2016, 30, 218–226. [Google Scholar] [CrossRef] [Green Version]
- Rogers, M.; Lemstra, M.; Bird, Y.; Nwankwo, C.; Rogers, M.; Moraros, J. Weight-loss intervention adherence and factors promoting adherence: A meta-analysis. Patient Prefer. Adherence 2016, 10, 1547–1559. [Google Scholar] [CrossRef] [Green Version]
- Sirur, R.; Richardson, J.; Wishart, L.; Hanna, S. The role of theory in increasing adherence to prescribed practice. Physiother. Can. 2009, 61, 68–77. [Google Scholar] [CrossRef] [Green Version]
- Lai, B.; Young, H.-J.; Bickel, C.S.; Motl, R.W.; Rimmer, J.H. Current trends in exercise intervention research, technology, and behavioral change strategies for people with disabilities: A scoping review. Am. J. Phys. Med. Rehabil. 2017, 96, 748–761. [Google Scholar] [CrossRef]
- Spring, B.; Champion, K.E.; Acabchuk, R.; Hennessy, E.A. Self-regulatory behaviour change techniques in interventions to promote healthy eating, physical activity, or weight loss: A meta-review. Health Psychol. Rev. 2020, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, B.D.; Curran, T.; Standage, M.; Sabiston, C.M.; Beauchamp, M.R. Predicting exercise motivation and exercise behavior: A moderated mediation model testing the interaction between perceived exercise variety and basic psychological needs satisfaction. Psychol. Sport Exerc. 2018, 36, 50–56. [Google Scholar] [CrossRef]
- Valenzuela, T.; Okubo, Y.; Woodbury, A.; Lord, S.R.; Delbaere, K. Adherence to technology-based exercise programs in older adults: A systematic review. J. Geriatr. Phys. Ther. 2018, 41, 49–61. [Google Scholar] [CrossRef]
- García-Bravo, S.; Cuesta-Gómez, A.; Campuzano-Ruiz, R.; López-Navas, M.J.; Domínguez-Paniagua, J.; Araújo-Narváez, A.; Barreñada-Copete, E.; García-Bravo, C.; Flórez-García, M.T.; Botas-Rodríguez, J.; et al. Virtual reality and video games in cardiac rehabilitation programs. A systematic review. Disabil. Rehabil. 2019, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Charness, G.; Gneezy, U. Incentives to exercise. Econometrica 2009, 77, 909–931. [Google Scholar] [CrossRef] [Green Version]
- Hawley-Hague, H.; Horne, M.; Skelton, D.A.; Todd, C. Review of how we should define (and measure) adherence in studies examining older adults’ participation in exercise classes. BMJ Open 2016, 6, e011560. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Slade, S.C.; Dionne, C.E.; Underwood, M.; Buchbinder, R. Consensus on Exercise Reporting Template (CERT): Explanation and elaboration statement. Br. J. Sports Med. 2016, 50, 1428–1437. [Google Scholar] [CrossRef] [Green Version]
- Albergoni, A.; Hettinga, F.J.; La Torre, A.; Bonato, M.; Sartor, F. The role of technology in adherence to physical activity programs in patients with chronic diseases experiencing fatigue: A systematic review. Sports Med. Open 2019, 5, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Marin, T.S.; Kourbelis, C.; Foote, J.; Newman, P.; Brown, A.; Daniel, M.; Coffee, N.T.; Nicholls, S.J.; Ganesan, A.; Versace, V.L.; et al. Examining adherence to activity monitoring devices to improve physical activity in adults with cardiovascular disease: A systematic review. Eur. J. Prev. Cardiol. 2019, 26, 382–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Driessen, E.J.; Peeters, M.E.; Bongers, B.C.; Maas, H.A.; Bootsma, G.P.; van Meeteren, N.L.; Janssen-Heijnen, M.L. Effects of prehabilitation and rehabilitation including a home-based component on physical fitness, adherence, treatment tolerance, and recovery in patients with non-small cell lung cancer: A systematic review. Crit. Rev. Oncol. Hematol. 2017, 114, 63–76. [Google Scholar] [CrossRef]
- Husebø, A.M.L.; Dyrstad, S.M.; Søreide, J.A.; Bru, E. Predicting exercise adherence in cancer patients and survivors: A systematic review and meta-analysis of motivational and behavioural factors. J. Clin. Nurs. 2013, 22, 4–21. [Google Scholar] [CrossRef]
- Kampshoff, C.S.; Jansen, F.; Van Mechelen, W.; May, A.M.; Brug, J.; Chinapaw, M.J.; Buffart, L.M. Determinants of exercise adherence and maintenance among cancer survivors: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 80. [Google Scholar] [CrossRef] [Green Version]
- McCahon, D.; Daley, A.J.; Jones, J.; Haslop, R.; Shajpal, A.; Taylor, A.; Wilson, S.; Dowswell, G. Enhancing adherence in trials promoting change in diet and physical activity in individuals with a diagnosis of colorectal adenoma; a systematic review of behavioural intervention approaches. BMC Cancer 2015, 15, 505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ormel, H.; Van Der Schoot, G.; Sluiter, W.; Jalving, M.; Gietema, J.; Walenkamp, A. Predictors of adherence to exercise interventions during and after cancer treatment: A systematic review. Psychooncology 2018, 27, 713–724. [Google Scholar] [CrossRef]
- Ruano-Ravina, A.; Pena-Gil, C.; Abu-Assi, E.; Raposeiras, S.; van ‘t Hof, A.V.; Meindersma, E.; Bossano Prescott, E.I.; González-Juanatey, J.R. Participation and adherence to cardiac rehabilitation programs. A systematic review. Int. J. Cardiol. 2016, 223, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Tierney, S.; Mamas, M.; Skelton, D.; Woods, S.; Rutter, M.K.; Gibson, M.; Neyses, L.; Deaton, C. What can we learn from patients with heart failure about exercise adherence? A systematic review of qualitative papers. Health Psychol. 2011, 30, 401–410. [Google Scholar] [CrossRef]
- Tierney, S.; Mamas, M.; Woods, S.; Rutter, M.K.; Gibson, M.; Neyses, L.; Deaton, C. What strategies are effective for exercise adherence in heart failure? A systematic review of controlled studies. Heart Fail. Rev. 2012, 17, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Li, F.; Zhou, C.; Li, J.; Hong, C.; Tong, Q. The effect of mobile applications for improving adherence in cardiac rehabilitation: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 2019, 19, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matata, B.M.; Williamson, S.A. A Review of interventions to improve enrolment and adherence to cardiac rehabilitation among patients aged 65 years or above. Curr. Cardiol. Rev. 2017, 13, 252–262. [Google Scholar] [CrossRef]
- Karmali, K.N.; Davies, P.; Taylor, F.; Beswick, A.; Martin, K.; Ebrahim, S. Promoting patient uptake and adherence in cardiac rehabilitation. Cochrane Database Syst. Rev. 2010, CD007131. [Google Scholar] [CrossRef]
- Simek, E.M.; McPhate, L.; Haines, T.P. Adherence to and efficacy of home exercise programs to prevent falls: A systematic review and meta-analysis of the impact of exercise program characteristics. Prev. Med. 2012, 55, 262–275. [Google Scholar] [CrossRef]
- Farrance, C.; Tsofliou, F.; Clark, C. Adherence to community based group exercise interventions for older people: A mixed-methods systematic review. Prev. Med. 2016, 87, 155–166. [Google Scholar] [CrossRef] [Green Version]
- Picorelli, A.M.A.; Pereira, L.S.M.; Pereira, D.S.; Felício, D.; Sherrington, C. Adherence to exercise programs for older people is influenced by program characteristics and personal factors: A systematic review. J. Physiother. 2014, 60, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Hughes, K.J.; Salmon, N.; Galvin, R.; Casey, B.; Clifford, A.M. Interventions to improve adherence to exercise therapy for falls prevention in community-dwelling older adults: Systematic review and meta-analysis. Age Ageing 2019, 48, 185–195. [Google Scholar] [CrossRef] [PubMed]
- McPhate, L.; Simek, E.M.; Haines, T.P. Program-related factors are associated with adherence to group exercise interventions for the prevention of falls: A systematic review. J. Physiother. 2013, 59, 81–92. [Google Scholar] [CrossRef] [Green Version]
- Horne, M.; Tierney, S. What are the barriers and facilitators to exercise and physical activity uptake and adherence among South Asian older adults: A systematic review of qualitative studies. Prev. Med. 2012, 55, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Room, J.; Hannink, E.; Dawes, H.; Barker, K. What interventions are used to improve exercise adherence in older people and what behavioural techniques are they based on? A systematic review. BMJ Open 2017, 7, e019221. [Google Scholar] [CrossRef]
- Beinart, N.A.; Goodchild, C.E.; Weinman, J.A.; Ayis, S.; Godfrey, E.L. Individual and intervention-related factors associated with adherence to home exercise in chronic low back pain: A systematic review. Spine J. 2013, 13, 1940–1950. [Google Scholar] [CrossRef]
- Bishop, F.L.; Fenge-Davies, A.L.; Kirby, S.; Geraghty, A.W. Context effects and behaviour change techniques in randomised trials: A systematic review using the example of trials to increase adherence to physical activity in musculoskeletal pain. Psychol. Health 2015, 30, 104–121. [Google Scholar] [CrossRef] [PubMed]
- Eisele, A.; Schagg, D.; Krämer, L.V.; Bengel, J.; Göhner, W. Behaviour change techniques applied in interventions to enhance physical activity adherence in patients with chronic musculoskeletal conditions: A systematic review and meta-analysis. Patient Educ. Couns. 2019, 102, 25–36. [Google Scholar] [CrossRef]
- Ezzat, A.M.; MacPherson, K.; Leese, J.; Li, L.C. The effects of interventions to increase exercise adherence in people with arthritis: A systematic review. Musculoskelet. Care 2015, 13, 1–18. [Google Scholar] [CrossRef]
- Jack, K.; McLean, S.M.; Moffett, J.K.; Gardiner, E. Barriers to treatment adherence in physiotherapy outpatient clinics: A systematic review. Man. Ther. 2010, 15, 220–228. [Google Scholar] [CrossRef]
- Jordan, J.L.; Holden, M.A.; Mason, E.E.; Foster, N.E. Interventions to improve adherence to exercise for chronic musculoskeletal pain in adults. Cochrane Database Syst. Rev. 2010, 2010, CD005956. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.T.; Siebert, S.; Coulter, E.H.; McDonald, D.A.; Paul, L. Level of adherence to prescribed exercise in spondyloarthritis and factors affecting this adherence: A systematic review. Rheumatol. Int. 2019, 39, 187–201. [Google Scholar] [CrossRef] [Green Version]
- McLean, S.M.; Burton, M.; Bradley, L.; Littlewood, C. Interventions for enhancing adherence with physiotherapy: A systematic review. Man. Ther. 2010, 15, 514–521. [Google Scholar] [CrossRef] [Green Version]
- Meade, L.B.; Bearne, L.M.; Sweeney, L.H.; Alageel, S.H.; Godfrey, E.L. Behaviour change techniques associated with adherence to prescribed exercise in patients with persistent musculoskeletal pain: Systematic review. Br. J. Health Psychol. 2019, 24, 10–30. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, P.J.A.; Bennell, K.L.; Dobson, F.L.; Van Ginckel, A.; Holden, M.A.; Hinman, R.S. Interventions to increase adherence to therapeutic exercise in older adults with low back pain and/or hip/knee osteoarthritis: A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Peek, K.; Sanson-Fisher, R.; MacKenzie, L.J.; Carey, M. Interventions to aid patient adherence to physiotherapist prescribed self-management strategies: A systematic review. Physiotherapy 2016, 102, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, I.B.; Armstrong, J.J.; Adachi, J.D.; MacDermid, J.C. Facilitators and barriers to exercise adherence in patients with osteopenia and osteoporosis: A systematic review. Osteoporos. Int. 2017, 28, 735–745. [Google Scholar] [CrossRef]
- Willett, M.; Duda, J.; Fenton, S.; Gautrey, C.; Greig, C.; Rushton, A. Effectiveness of behaviour change techniques in physiotherapy interventions to promote physical activity adherence in lower limb osteoarthritis patients: A systematic review. PLoS ONE 2019, 14, e0219482. [Google Scholar] [CrossRef]
- Burgess, E.; Hassmén, P.; Pumpa, K.L. Determinants of adherence to lifestyle intervention in adults with obesity: A systematic review. Clin. Obes. 2017, 7, 123–135. [Google Scholar] [CrossRef]
- Burgess, E.; Hassmén, P.; Welvaert, M.; Pumpa, K. Behavioural treatment strategies improve adherence to lifestyle intervention programmes in adults with obesity: A systematic review and meta-analysis. Clin. Obes. 2017, 7, 105–114. [Google Scholar] [CrossRef]
- Bullard, T.; Ji, M.; An, R.; Trinh, L.; MacKenzie, M.; Mullen, S.P. A systematic review and meta-analysis of adherence to physical activity interventions among three chronic conditions: Cancer, cardiovascular disease, and diabetes. BMC Public Health 2019, 19, 636. [Google Scholar] [CrossRef] [Green Version]
- Emmerson, K.B.; Harding, K.E.; Taylor, N.F. Providing exercise instructions using multimedia may improve adherence but not patient outcomes: A systematic review and meta-analysis. Clin. Rehabil. 2019, 33, 607–618. [Google Scholar] [CrossRef] [PubMed]
- Shore, C.B.; Hubbard, G.; Gorely, T.; Polson, R.; Hunter, A.; Galloway, S.D. Insufficient reporting of factors associated with exercise referral scheme uptake, attendance, and adherence: A systematic review of reviews. J. Phys. Act. Health 2019, 16, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Harwood, A.-E.; Smith, G.E.; Cayton, T.; Broadbent, E.; Chetter, I.C. A systematic review of the uptake and adherence rates to supervised exercise programs in patients with intermittent claudication. Ann. Vasc. Surg. 2016, 34, 280–289. [Google Scholar] [CrossRef]
- Lin, E.; Nguyen, C.H.; Thomas, S.G. Completion and adherence rates to exercise interventions in intermittent claudication: Traditional exercise versus alternative exercise–a systematic review. Eur. J. Prev. Cardiol. 2019, 26, 1625–1633. [Google Scholar] [CrossRef] [PubMed]
- Van Der Wardt, V.; Hancox, J.; Gondek, D.; Logan, P.; Das Nair, R.; Pollock, K.; Harwood, R.H. Adherence support strategies for exercise interventions in people with mild cognitive impairment and dementia: A systematic review. Prev. Med. Rep. 2017, 7, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Vseteckova, J.; Deepak-Gopinath, M.; Borgstrom, E.; Holland, C.; Draper, J.; Pappas, Y.; McKeown, E.; Dadova, K.; Gray, S. Barriers and facilitators to adherence to group exercise in institutionalized older people living with dementia: A systematic review. Eur. Rev. Aging Phys. Act. 2018, 15, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Sumlin, L.L.; Garcia, T.J.; Brown, S.A.; Winter, M.A.; García, A.A.; Brown, A.; Cuevas, H.E. Depression and adherence to lifestyle changes in type 2 diabetes: A systematic review. Diabetes Educ. 2014, 40, 731–744. [Google Scholar] [CrossRef]
- Gaikwad, S.B.; Mukherjee, T.; Shah, P.V.; Ambode, O.I.; Johnson, E.G.; Daher, N.S. Home exercise program adherence strategies in vestibular rehabilitation: A systematic review. Phys. Ther. Rehabil. Sci. 2016, 5, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Bachmann, C.; Oesch, P.; Bachmann, S. Recommendations for improving adherence to home-based exercise: A systematic review. Phys. Med. Rehabil. Kurortmed. 2017, 28, 20–31. [Google Scholar] [CrossRef] [Green Version]
- Eynon, M.; Foad, J.; Downey, J.; Bowmer, Y.; Mills, H. Assessing the psychosocial factors associated with adherence to exercise referral schemes: A systematic review. Scand. J. Med. Sci. Sports 2019, 29, 638–650. [Google Scholar] [CrossRef]
- Pavey, T.; Taylor, A.; Hillsdon, M.; Fox, K.; Campbell, J.; Foster, C.; Moxham, T.; Mutrie, N.; Searle, J.; Taylor, R. Levels and predictors of exercise referral scheme uptake and adherence: A systematic review. J. Epidemiol. Community Health 2012, 66, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Morgan, F.; Battersby, A.; Weightman, A.L.; Searchfield, L.; Turley, R.; Morgan, H.; Jagroo, J.; Ellis, S. Adherence to exercise referral schemes by participants—what do providers and commissioners need to know? A systematic review of barriers and facilitators. BMC Public Health 2016, 16, 227. [Google Scholar] [CrossRef] [PubMed]
- Barmentloo, L.M.; Olij, B.F.; Erasmus, V.; Smilde, D.; Schoon, Y.; Polinder, S. Personal preferences of participation in fall prevention programmes: A descriptive study. BMC Geriatr. 2020, 20, 185. [Google Scholar] [CrossRef]
- Davis, A.M.; Palaganas, M.; Li, L.C. Public opinion on community-based education and exercise programs for managing hip and knee osteoarthritis-like symptoms: Results of a survey. Patient Prefer. Adherence 2016, 10, 283–290. [Google Scholar] [CrossRef] [Green Version]
- Craike, M.; Gaskin, C.J.; Courneya, K.S.; Fraser, S.F.; Salmon, J.; Owen, P.J.; Broadbent, S.; Livingston, P.M. Predictors of adherence to a 12-week exercise program among men treated for prostate cancer: ENGAGE study. Cancer Med. 2016, 5, 787–794. [Google Scholar] [CrossRef]
- Catala, P.; Lopez-Roig, S.; Ecija, C.; Suso-Ribera, C.; Peñacoba Puente, C. Why do some people with severe chronic pain adhere to walking prescriptions whilst others won’t? A cross-sectional study exploring clinical and psychosocial predictors in women with fibromyalgia. Rheumatol. Int. 2020, 1–6. [Google Scholar] [CrossRef]
- Stubbs, B.; Vancampfort, D.; Rosenbaum, S.; Ward, P.B.; Richards, J.; Soundy, A.; Veronese, N.; Solmi, M.; Schuch, F.B. Dropout from exercise randomized controlled trials among people with depression: A meta-analysis and meta regression. J. Affect. Disord. 2016, 190, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Plotnikoff, R.C.; Hotz, S.B.; Birkett, N.J.; Courneya, K.S. Exercise and the transtheoretical model: A longitudinal test of a population sample. Prev. Med. 2001, 33, 441–452. [Google Scholar] [CrossRef]
- Gatt, K.; Schembri, J.; Katsanos, K.H.; Christodoulou, D.; Karmiris, K.; Kopylov, U.; Pontas, C.; Koutroubakis, I.E.; Foteinogiannopoulou, K.; Fabian, A.; et al. Inflammatory Bowel disease [IBD] and physical activity: A study on the impact of diagnosis on the level of exercise amongst patients with IBD. J. Crohn’s Colitis 2019, 13, 686–692. [Google Scholar] [CrossRef]
- Midtgaard, J.; Baadsgaard, M.T.; Møller, T.; Rasmussen, B.; Quist, M.; Andersen, C.; Rørth, M.; Adamsen, L. Self-reported physical activity behaviour; exercise motivation and information among Danish adult cancer patients undergoing chemotherapy. Eur. J. Oncol. Nurs. 2009, 13, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.-C.; Weng, S.-C.; Chou, M.-C.; Tang, Y.-J.; Lee, S.-H.; Chen, D.-Y.; Chuang, Y.-W.; Yu, C.-H.; Kuo, H.-W. How family support affects physical activity (PA) among middle-aged and elderly people before and after they suffer from chronic diseases. Arch. Gerontol. Geriatr. 2011, 53, 274–277. [Google Scholar] [CrossRef]
- Neutel, C.I.; Campbell, N.R. Changes in lifestyle after hypertension diagnosis in Canada. Can. J. Cardiol. 2008, 24, 199–204. [Google Scholar] [CrossRef] [Green Version]
- Dontje, M.L.; Krijnen, W.P.; De Greef, M.H.; Peeters, G.G.; Stolk, R.P.; Van Der Schans, C.P.; Brown, W.J. Effect of diagnosis with a chronic disease on physical activity behavior in middle-aged women. Prev. Med. 2016, 83, 56–62. [Google Scholar] [CrossRef]
- Westmaas, J.L.; Newton, C.C.; Stevens, V.L.; Flanders, W.D.; Gapstur, S.M.; Jacobs, E.J. Does a recent cancer diagnosis predict smoking cessation? An analysis from a large prospective US cohort. J. Clin. Oncol. 2015, 33, 1647–1652. [Google Scholar] [CrossRef] [PubMed]
- Flocke, S.A.; Clark, E.; Antognoli, E.; Mason, M.J.; Lawson, P.J.; Smith, S.; Cohen, D.J. Teachable moments for health behavior change and intermediate patient outcomes. Patient Educ. Couns. 2014, 96, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Hochbaum, G.M. Public Participation in Medical Screening Programs: A Socio-Psychological Study; US Department of Health, Education, and Welfare: Washington, DC, USA, 1958. [Google Scholar]
- Jasmine, T.J.X.; Wai-Chi, S.C.; Hegney, D.G. The impact of knowledge and beliefs on adherence to cardiac rehabilitation programs in patients with heart failure: A systematic review. JBI Libr. Syst. Rev. 2012, 10, 399–470. [Google Scholar] [CrossRef]
- Woolley, K.; Fishbach, A. Immediate rewards predict adherence to long-term goals. Pers. Soc. Psychol. Bull. 2017, 43, 151–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, D.M.; Papandonatos, G.D.; Napolitano, M.A.; Lewis, B.A.; Whiteley, J.A.; Marcus, B.H. Perceived enjoyment moderates the efficacy of an individually tailored physical activity intervention. J. Sport Exerc. Psychol. 2006, 28, 300–309. [Google Scholar] [CrossRef]
- Wankel, L.M. The importance of enjoyment to adherence and psychological benefits from physical activity. Int. J. Sport Psychol. 1993, 24, 151–169. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Simmich, J.; Deacon, A.J.; Russell, T.G. Active video games for rehabilitation in respiratory conditions: Systematic review and meta-analysis. JMIR Serious Games 2019, 7, e10116. [Google Scholar] [CrossRef] [PubMed]
- Barry, G.; Van Schaik, P.; Macsween, A.; Dixon, J.; Martin, D. Exergaming (XBOX Kinect™) versus traditional gym-based exercise for postural control, flow and technology acceptance in healthy adults: A randomised controlled trial. BMC Sports Sci. Med. Rehabil. 2016, 8, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinnafick, F.-E.; Thøgersen-Ntoumani, C.; Shepherd, S.O.; Wilson, O.J.; Wagenmakers, A.J.; Shaw, C.S. In It Together: A qualitative evaluation of participant experiences of a 10-week, group-based, workplace HIIT Program for insufficiently active adults. J. Sport Exerc. Psychol. 2018, 40, 10–19. [Google Scholar] [CrossRef]
- Hagberg, L.A.; Lindahl, B.; Nyberg, L.; Hellénius, M.-L. Importance of enjoyment when promoting physical exercise. Scand. J. Med. Sci. Sports 2009, 19, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Backhouse, S.H.; Ekkekakis, P.; Biddle, S.J.; Foskett, A.; Williams, C. Exercise makes people feel better but people are inactive: Paradox or artifact? J. Sport Exerc. Psychol. 2007, 29, 498–517. [Google Scholar] [CrossRef] [Green Version]
- Rose, E.A.; Parfitt, G. Pleasant for some and unpleasant for others: A protocol analysis of the cognitive factors that influence affective responses to exercise. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Leone, L.A.; Ward, D.S. A mixed methods comparison of perceived benefits and barriers to exercise between obese and nonobese women. J. Phys. Act. Health 2013, 10, 461–469. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, M.S.; Goodman, J.M.; Alter, D.A.; John, L.K.; Oh, P.I.; Pakosh, M.T.; Faulkner, G.E. Financial incentives for exercise adherence in adults. Am. J. Prev. Med. 2013, 45, 658–667. [Google Scholar] [CrossRef]
- Ryan, R.; Deci, E. Intrinsic Motivation and Self Determination in Human Behaviour; Plenum: New York, NY, USA, 1985. [Google Scholar]
- Helgadóttir, B.; Hallgren, M.; Kullberg, C.L.; Forsell, Y. Sticking with it? Factors associated with exercise adherence in people with mild to moderate depression. Psychol. Sport Exerc. 2018, 35, 104–110. [Google Scholar] [CrossRef]
- Ashworth, N.L.; Chad, K.E.; Harrison, E.L.; Reeder, B.A.; Marshall, S.C. Home versus center based physical activity programs in older adults. Cochrane Database Syst. Rev. 2005, 2005, CD004017. [Google Scholar] [CrossRef] [PubMed]
- Lin, N.; Simeone, R.S.; Ensel, W.M.; Kuo, W. Social support, stressful life events, and illness: A model and an empirical test. J. Health Soc. Behav. 1979, 20, 108–119. [Google Scholar] [CrossRef]
- Ozbay, F.; Johnson, D.C.; Dimoulas, E.; Morgan, C.A.; Charney, D.; Southwick, S. Social support and resilience to stress: From neurobiology to clinical practice. Psychiatry 2007, 4, 35–40. [Google Scholar] [PubMed]
- Essery, R.; Geraghty, A.W.A.; Kirby, S.; Yardley, L. Predictors of adherence to home-based physical therapies: A systematic review. Disabil. Rehabil. 2017, 39, 519–534. [Google Scholar] [CrossRef] [Green Version]
- Gordon, C.R.; Rezzadeh, K.S.; Li, A.; Vardanian, A.; Zelken, J.; Shores, J.T.; Sacks, J.M.; Segovia, A.L.; Jarrahy, R. Digital mobile technology facilitates HIPAA-sensitive perioperative messaging, improves physician-patient communication, and streamlines patient care. Patient Saf. Surg. 2015, 9, 21. [Google Scholar] [CrossRef] [Green Version]
- Rosen, Z.; King-Dowling, S.; Petersen, J.M.; Kemps, E.; Lewis, L.K.; Prichard, I. Associations between commercial app use and physical activity: Cross-sectional study. J. Med. Internet Res. 2020, 22, e17152. [Google Scholar] [CrossRef]
- Oeldorf-Hirsch, A.; High, A.C.; Christensen, J.L. Count your calories and share them: Health benefits of sharing mhealth information on social networking sites. Health Commun. 2019, 34, 1130–1140. [Google Scholar] [CrossRef]
- Santarossa, S.; Kane, D.; Senn, C.Y.; Woodruff, S.J. Exploring the role of in-person components for online health behavior change interventions: Can a digital person-to-person component suffice? J. Med. Internet Res. 2018, 20, e144. [Google Scholar] [CrossRef] [PubMed]
- Dobson, F.; Bennell, K.L.; French, S.D.; Nicolson, P.J.; Klaasman, R.N.; Holden, M.A.; Atkins, L.; Hinman, R.S. Barriers and facilitators to exercise participation in people with hip and/or knee osteoarthritis: Synthesis of the literature using behavior change theory. Am. J. Phys. Med. Rehabil. 2016, 95, 372–389. [Google Scholar] [CrossRef]
- Rodrigues, F.; Bento, T.; Cid, L.; Pereira Neiva, H.; Teixeira, D.; Moutão, J.; Almeida Marinho, D.; Monteiro, D. Can Interpersonal behavior influence the persistence and adherence to physical exercise practice in adults? A systematic review. Front. Psychol. 2018, 9, 2141. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, M.; Murphy, M.M.; Guell, C. Barriers and facilitators to physical activity amongst overweight and obese women in an Afro-Caribbean population: A qualitative study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 97. [Google Scholar] [CrossRef] [Green Version]
- Abramson, L.Y.; Seligman, M.E.; Teasdale, J.D. Learned helplessness in humans: Critique and reformulation. J. Abnorm. Psychol. 1978, 87, 49. [Google Scholar] [CrossRef]
- Pourhoseinzadeh, M.; Gheibizadeh, M.; Moradikalboland, M. The relationship between health locus of control and health behaviors in emergency medicine personnel. Int. J. Community Based Nurs. Midwifery 2017, 5, 397–407. [Google Scholar]
- Bhat, A.A.; DeWalt, D.A.; Zimmer, C.R.; Fried, B.J.; Callahan, L.F. The role of helplessness, outcome expectation for exercise and literacy in predicting disability and symptoms in older adults with arthritis. Patient Educ. Couns. 2010, 81, 73–78. [Google Scholar] [CrossRef]
- DeWalt, D.A.; Berkman, N.D.; Sheridan, S.L.; Lohr, K.N.; Pignone, M.P. Literacy and health outcomes: A systematic review of the literature. J. Gen. Intern. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef]
- Thompson, E.L.; Broadbent, J.; Bertino, M.D.; Staiger, P.K. Do Pain-related beliefs influence adherence to multidisciplinary rehabilitation? A systematic review. Clin. J. Pain 2016, 32, 164–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emanuel, E.J.; Emanuel, L.L. Four models of the physician-patient relationship. JAMA 1992, 267, 2221–2226. [Google Scholar] [CrossRef] [PubMed]
- Reach, G. Patient autonomy in chronic care: Solving a paradox. Patient Prefer. Adherence 2013, 8, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, K.S.; Lee, E. Relationships of health literacy to self-care behaviors in people with diabetes aged 60 and above: Empowerment as a mediator. J. Adv. Nurs. 2018, 74, 2363–2372. [Google Scholar] [CrossRef]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bovend’Eerdt, T.J.H.; Botell, R.E.; Wade, D.T. Writing SMART rehabilitation goals and achieving goal attainment scaling: A practical guide. Clin. Rehabil. 2009, 23, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. From intentions to actions: A theory of Planned Behavior. In Action Control: From Cognition to Behavior; Springer: Berlin/Heidelberg, Germany, 1985; pp. 11–39. [Google Scholar]


{kind=link}
| Patients Characteristics | Number of Studies | Type of Exercise Interventions Revised | |
|---|---|---|---|
| Cancer | Cancer patients or survivors | 4 | Home-based: 1 review Any: 6 reviews |
| Advanced cancer | 1 | ||
| Non-small cell lung cancer | 1 | ||
| Colorectal cancer | 1 | ||
| Cardiovascular disease | Heart failure | 2 | Center-based: 1 review Any: 6 reviews |
| Under cardiac rehabilitation program | 4 | ||
| General cardiovascular conditions | 1 | ||
| Older adults | Falls prevention | 3 | Center-based: 2 review Home-based: 1 review Any: 5 reviews |
| Healthy elderly | 5 | ||
| Musculoskeletal disorders | Low back pain | 1 | Center-based: 1 review Home-based: 1 review Any: 10 reviews |
| Arthritis | 3 | ||
| Osteoporosis/osteopenia | 1 | ||
| General/multiple musculoskeletal pain or chronic conditions | 7 | ||
| Obesity or weight loss | 3 | Center-based: 3 review | |
| Intermittent claudication | 2 | Center-based: 1 review Any: 1 review | |
| Mild cognitive impairment and dementia | 2 | Center-based: 1 review Any: 1 review | |
| Parkinson | 1 | Any: 1 review | |
| Type 2 diabetes | 1 | Any: 1 review | |
| Solid-organ transplant candidates | 1 | Any: 1 review | |
| Under vestibular rehabilitation | 1 | Home-based: 1 review | |
| Different chronic diseases | 6 | Center-based: 1 review Home-based: 2 reviews Any: 3 reviews | |
| Exercise Referral schemes | 4 | Center-based: 2 reviews Any: 2 reviews | |
| Key Factors | Sub-Key Factors | Number of Reviews Including Each Key Factor | |||||
|---|---|---|---|---|---|---|---|
| Total | Cancer | CVD | Musculo-Skeletal Disorders | Older Adults | Obesity/Weight Loss | ||
| Exercise characteristics design | Characteristics of the exercise are individualized and scientifically correct | 23 | 3 | 3 | 4 | 4 | 2 |
| The duration of the exercise intervention is not too long | 10 | - | 1 | 1 | 3 | 1 | |
| Multidisciplinarity | Multidisciplinary program | 12 | - | 1 | 5 | 2 | 2 |
| Supervision | Supervision | 17 | 1 | 1 | 4 | 4 | 1 |
| Technology | Use of adequate technology | 12 | - | 3 | 1 | 3 | 1 |
| Initial exploration of participant’s characteristics, barriers, and facilitators | Previous habits and physical and mental health status of the participants are known | 36 | 7 | 6 | 5 | 2 | 3 |
| Barriers and facilitators are explored before the exercise program is delivered to search for alternatives | 29 | 5 | 6 | 5 | 3 | 2 | |
| Participants education, adequate expectations, and knowledge about risks and benefits | Participants are educated about physical exercise in their condition | 17 | 2 | 4 | 3 | 2 | 1 |
| Participants are adequately informed about the risks and benefits of the program | 15 | - | 3 | 1 | 4 | 1 | |
| Adequate expectations | 15 | - | 3 | 3 | 3 | 1 | |
| Enjoyment and absence of unpleasant experiences | Enjoyment | 10 | - | 1 | 3 | 2 | 1 |
| Absence of unpleasant experiences | 9 | 1 | - | 3 | 1 | 1 | |
| Integration in daily living | Participant’s preferences and background are considered in the program to enhance its integration into their lifestyle | 29 | 3 | 2 | 5 | 5 | 3 |
| Good accessibility, adequate place, and flexibility in the schedule | 21 | 4 | 3 | 3 | 4 | 2 | |
| Social support and relatedness | Social support from peers and family | 22 | 1 | 5 | 4 | 3 | 1 |
| Social support from the professional | 22 | 2 | 3 | 5 | 2 | 1 | |
| Relatedness | 11 | - | 2 | 2 | 3 | - | |
| Communication and feedback | Intra-session feedback | 11 | 2 | 2 | 3 | 2 | 1 |
| Bilateral and fluid communication with the staff | 16 | - | 2 | 3 | 3 | 1 | |
| Available progress information and monitoring | Objective information for patients to know their progress | 17 | 1 | 3 | 2 | 5 | 2 |
| Exercise is monitored | 16 | 2 | 4 | - | 3 | 2 | |
| Self-efficacy and competence | Self-efficacy | 21 | 2 | 3 | 3 | 3 | 2 |
| Competence | 7 | - | 3 | - | 1 | - | |
| Participant’s active role | Self-management, self-control, and self-monitoring | 16 | 1 | 3 | 4 | 1 | - |
| Autonomy and empowerment | 8 | - | 1 | 1 | 2 | - | |
| Goal setting | Objectives are clear and established with the patient | 12 | 1 | 2 | 5 | - | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collado-Mateo, D.; Lavín-Pérez, A.M.; Peñacoba, C.; Del Coso, J.; Leyton-Román, M.; Luque-Casado, A.; Gasque, P.; Fernández-del-Olmo, M.Á.; Amado-Alonso, D. Key Factors Associated with Adherence to Physical Exercise in Patients with Chronic Diseases and Older Adults: An Umbrella Review. Int. J. Environ. Res. Public Health 2021, 18, 2023. https://doi.org/10.3390/ijerph18042023
Collado-Mateo D, Lavín-Pérez AM, Peñacoba C, Del Coso J, Leyton-Román M, Luque-Casado A, Gasque P, Fernández-del-Olmo MÁ, Amado-Alonso D. Key Factors Associated with Adherence to Physical Exercise in Patients with Chronic Diseases and Older Adults: An Umbrella Review. International Journal of Environmental Research and Public Health. 2021; 18(4):2023. https://doi.org/10.3390/ijerph18042023
Chicago/Turabian StyleCollado-Mateo, Daniel, Ana Myriam Lavín-Pérez, Cecilia Peñacoba, Juan Del Coso, Marta Leyton-Román, Antonio Luque-Casado, Pablo Gasque, Miguel Ángel Fernández-del-Olmo, and Diana Amado-Alonso. 2021. "Key Factors Associated with Adherence to Physical Exercise in Patients with Chronic Diseases and Older Adults: An Umbrella Review" International Journal of Environmental Research and Public Health 18, no. 4: 2023. https://doi.org/10.3390/ijerph18042023